Positive Approaches Journal, Volume 8, Issue 1
| Site: | My ODP |
| Course: | My ODP |
| Book: | Positive Approaches Journal, Volume 8, Issue 1 |
| Printed by: | |
| Date: | Sunday, June 28, 2026, 12:49 PM |
Positive Approaches Journal | 5

Volume 8 ► Issue 1 ► 2019
The Science and Art of Support
Introduction
Considering how to most effectively support someone, especially someone with complex needs, is not about one approach, philosophy, or theoretical perspective. Sometimes, it is about finding the balance between the “Art and Science” of support. What does that entail? Building a foundation of relationships, trust, and rapport in which someone feels safe based on the individual’s preferences, interests, and desires is the “art” that you cannot learn from a textbook. Yet, we need to hone those skills to figure out how to establish a base from which good supports evolves. Coupled with that foundation, empirically validated science, tools, interventions, and techniques like Cognitive Behavioral Therapy or Functional Communication Training should be employed. Implementing this science, what other people have proven works, capitalizes on the sometimes limited window of opportunity, time, energy and resources to teach prosocial and necessary living skills, as well as to decrease socially unacceptable or dangerous behaviors like ingesting inedible objects or isolating oneself. This integration already exists in the Positive Behavior Support (PBS) movement which encourages us, as supporters, to think about holistic ways to support people through their lives. “PBS is an approach that blends values about the rights of people with a practical science about how learning and behavior change can occur” (Horner, 2000)1. In this issue, esteemed professionals from Pennsylvania provide their perspectives and experiences on both the art and science needed to be considered as we support people with autism, intellectual disabilities, other developmental disabilities and mental illness.
—Stacy L. Nonnemacher, Ph.D.
1Horner, R.H. (2000). Positive Behavior Supports. Focus on Autism and Other Developmental Disabilities, 15, 97-105.
Positive Approaches Journal | 6
Volume 8 ► Issue 1 ► 2019
Data Discoveries
Data Discoveries presents useful data in ways that are interesting and customizable. Data presented will be focused on a topic that is relevant for each issue theme and seek to promote new ideas about what data to use and how to use it.
Employment plays an important role in helping individuals with and without a disability live independently and participate in their communities. Providing employment support services is a specialty for some providers, providers include it across multiple types of services they provide, or providers link to employment services separately.
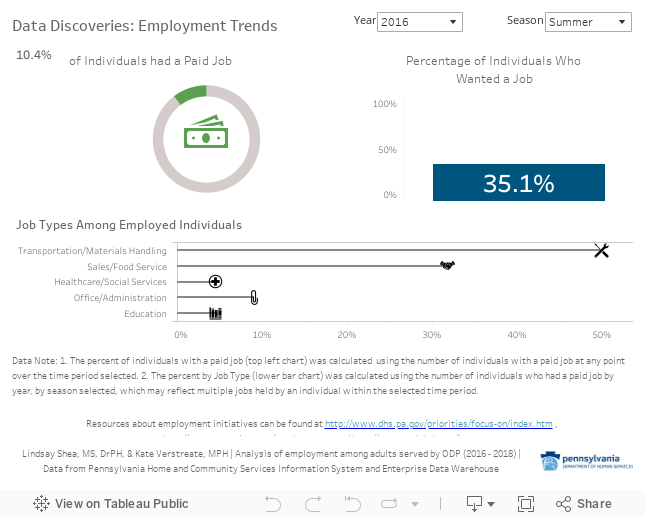
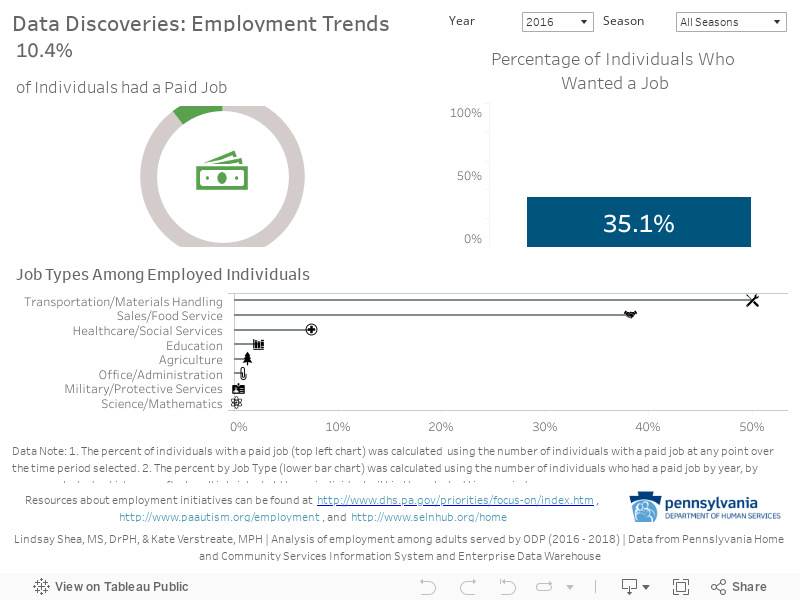
In this issue, Data Discoveries presents employment data from the Office of Developmental Programs (ODP). ODP instituted new questions asking program participants if they have a job and, among those who are working, a variety of questions including the type of job they have and the number of hours they work each week. In this issue of Positive Approaches, Data Discoveries includes employment data that can be filtered over time:
The doughnut chart displays the proportion of people in ODP programs who had a competitive, integrated job.
The suitcase figure shows the proportion of people with an employment goal on their ISP.
Among people who are employed, job types are shown in the bottom bar chart.
Use the filters for year and season to see how these numbers change over time and to familiarize yourself with Tableau. The filter for seasons applies only to the Job Type figure at the bottom since seasons and corresponding weather impact Job Type trends. The interactive features, including drop down filters, allow for easy viewing of changes over the three years.

Bambara | 7-12
Volume 8 ► Issue 1 ► 2019
False
Dichotomies in Positive Behavior Support:
One More Time with Emphasis
Linda M. Bambara, Ed. D.
Abstract
In this article I reflect on my personal experiences in the evolution of positive behavior support. I emphasize that positive behavior support integrates scientifically based behavioral practices, person-centered values, and other theoretical perspectives to address the complex support needs of individuals who present challenging behaviors. Each of these orientations work in concert with one another and should not be separated. Beware of the false dichotomies that cause supporters to argue about the better approach, form allegiances to specific methodologies, rather than the individuals we support, and reject effective practices.
I am truly honored to contribute to the inaugural issue of Positive
Approaches. This provides me with an
opportunity to reflect on my over 30-year history in the positive behavior
support evolution. Of course, like many
of my contemporaries, my approach was not always positive. In my first teaching position in a
residential school for children and adolescents with emotional and behavior
disorders and autism, I demanded compliance.
I praised plenty, but behavioral infractions were met with time outs,
seclusion, and physical restraint. It
did not take me long to realize though that my power to positively influence my
students, came not from my negative consequences, but through forming positive,
genuine, caring relationships with them and honoring their needs.
In the late 1980’s, I came to Lehigh University and directed Lehigh Support for Community Living, a university-based program that provided residential supports to adults with developmental disabilities recently deinstitutionalized from Pennsylvania’s state institutions. Here, as a young assistant professor, I was faced with the enormous responsibility of facilitating the integration and community acceptance of 18 individuals whose lives had been broken and who communicated their anguish through various forms of self-injury and aggression. It is hard to say where my staff and I drew our strength from to go against conventional practices, but within a few short years, we eliminated all token economy programs and other forms of artificial consequences that were intended to control problem behaviors. “Emergency” restraints, easily misused by staff, were also eliminated. Reactive, consequence interventions did not reduce the very problem behaviors we sought to reduce, but rather exacerbated them.
A change in approach, a positive approach, was needed, and I, like many of my colleagues nationwide, drew from a variety of sources. I was influenced by Ted Carr and Mark Durand, behavioral scientists who documented through various research studies that challenging behavior is communicative, and can be eliminated by teaching people alternative means of expressing their needs. They also made it clear that non-functional interventions, such as imposed punishment or rewards, are nonsensical if the intervention does not address the underlying function of behavior or change problematic contexts that created the need for challenging behaviors. I was also influenced by Herb Lovett, clinical psychologist and disability advocate, who argued that meaningful change, requires understanding people’s histories and social context, learning to listen to the what and how of people’s communication, and responding in ways that maintain personal dignity and respect in ways that all of us want to be treated. Leaders of the person-centered planning and community integration movements, such as Beth Mount, John O’Brien, Marsha Forrest, and Steve Taylor, were also strongly influential. Their messages about building capacity rather than remediating deficits and improving quality of life revolutionized the types of supports offered to people with developmental disabilities. The synergy of all these influences from different orientations gave birth to positive behavior support, or positive approaches as known in Pennsylvania. In the mid-late 90’s, I was a member of the state’s Positive Approaches Committee that was responsible for changing state regulations for residential settings by delimiting or prohibiting “restrictive interventions,” including the use of non-functional rewards, restraints, and seclusion. As one of the first states to establish policy on restrictive interventions, I proudly wore a “PA in PA” pin (Positive Approaches in Pennsylvania) at national conferences for all to see.
The evolution toward positive behavior support was not met without any controversy. At first, many argued against the complete elimination of aversives, for after all, some people who present the most extreme challenging behaviors might need it, the logic went. Overtime as professionals gained confidence by making meaningful changes for people with disabilities with difficult behaviors through prevention, teaching, and lifestyle change, arguments about the need for aversive interventions were repudiated and the positive behavior support movement gained nation-wide acceptance. In a seminal article, Positive Behavior Support: Evolution of an Applied Science, Carr and colleagues1, argued that the uniqueness of positive behavior support rests on the integration of multiple approaches and perspectives (e.g., person-centered planning, systems theory) with an applied science rooted in applied behavior analysis. These various approaches, they explained, are integrated into a cohesive whole with the primary goal of improving the quality life and happiness of people with developmental disabilities and the secondary goal of reducing problem behavior.
In other words, positive behavior support is a mash-up of scientifically based behavioral practices, person-centered values, and other theoretical orientations, driven by a comprehensive understanding of individual needs. This makes sense to me, but as soon as these thoughts on PBS were promulgated, a new form of controversy emerged which continues to exist in various forms today. People often like to argue about what is the better, more positive approach, and in the upshot often lose perspective on the most important thing: the lives of people with disabilities. In my article, Are you a Behaviorist or Bonder?2, I wrote about the false dichotomies within the positive behavior support movement that divides us. Do you ascribe to a behavioral, scientific position or a more person-centered, relationship-oriented position when supporting people with disabilities? Are you a follower of Herb Lovett or Ted Carr? Do you ascribe to trauma informed care? Dual diagnoses interventions? Should we use only evidence-based practices in our work, or do you reject scientific practices because of their limitations? These dichotomies, intentionally created or not, cause us to form allegiances around certain approaches rather than form an allegiance to the people we are called upon to support. People with disabilities deserve the best, and we are best when we are informed by what works and what truly makes a difference in their lives.
Beware of false dichotomies. Positive behavior support is the marriage between person-centered values, scientific practices, and different theoretical orientations. These constructs work in coordination with one another and are not meant to be opposing forces. Person-centered values ensure that the supports and services we provide to people with disabilities are meaningful to them and contributes to their happiness. Person-centered values guide us to consider people’s preferences, hopes and dreams, make changes to improve their quality of life, and treat them respectfully. The actions taken from a person-centered perspective can by itself reduce challenging behaviors by making positive lifestyle changes, but for many individuals with complex support needs, it is not enough. I know of loving families who provide the best for their children and still struggle with their children’s difficult behaviors. Such families would benefit from behavioral strategies to first identify factors that are contributing to challenging behaviors, and then learn how to prevent problem behaviors by making environmental adaptations and teaching specific skills so that their children can cope with difficulties, better communicate, or better control their environments in ways that others can accept and understand. Being person-centered, does not necessarily mean that professionals and families intuitively know how to address the needs of individuals with challenging behaviors even in the best of environments. Further, values in the absence of scientifically based practices, can lead families and professionals down a perilous path of selecting interventions based on hopes and beliefs, and maybe the testimonials from others, without a shred of evidence of effectiveness. The autism field, in particular, is replete with unsubstantiated “treatments” that are not only ineffective, but potentially harmful.
On the other hand, the implementation of scientifically based practices in the absence of person-centered values, can create equally disastrous outcomes for people with disabilities and their families. It is true that of all the intervention approaches developed to teach people with disabilities new skills and reduce problem behaviors, applied behavior analysis-based methods are highly and perhaps, most effective.3 However, in the absence of person-centered values, the application of behavioral approaches can miss the big picture, and trivialize the intervention. For example, we can easily teach a young man working in a sheltered workshop to appropriately request staff assistance when bored, rather than screaming, however, if the big picture is missed—the young man is bored out of his mind doing repetitive tasks—then what has been accomplished? In this scenario I predict that the young man would repeatedly request staff attention, albeit appropriately for a while, until the staff find his constant requests intolerable, they ignore him, and then he reverts back to problem behaviors. One of the chief criticisms of behavioral interventions, is not that they are ineffective, but that they are often not well integrated into a meaningful whole of a person’s life, resulting in socially unacceptable, and at times morally abhorrent practices (e.g., electric shock), causing some supporters to reject anything behavioral. However, it is not that behavioral approaches per se are faulty, but the way they have been applied. Applied behavior analysis is not a set of discrete techniques, a pre-packaged program or curriculum. Rather it is a scientific process that guides us to understand and then positively influence human behavior. It offers a systematic way of comprehensively understanding and changing problematic situations at both proximal (immediately surrounding the person) and distal (broader contextual factors) levels of support. When used within the context of person-centered values and applied in ecologically valid ways to improve quality of life, the form of intervention changes, resulting in powerful and meaningful outcomes for people with disabilities as documented by a vast volume of research.
Finally, person-centered values and behaviorally based scientific practices do not hold all the answers, opening PBS to integrate other theoretical perspectives. For example, systems theory, ecological psychology, and community psychology have had a huge impact on positive behavior support1. These perspectives have been responsible for the multi-tiered systems of support in school-wide positive behavior support, collaborations with families and other stakeholders, and the idea that supporting the people who support individuals with challenging behaviors is essential for success. Opening ourselves to well informed, but different theoretical frameworks requires a certain amount of humility to know what we do not know, so that we can learn from one another. This does not mean that we reject the basic precepts of PBS, but rather seek to integrate new ideas and approaches to improve and expand supports.
In summary, positive behavior support is an evolving practice that integrates person-centered values with behaviorally based scientific practices and other theoretical orientations to address the comprehensive needs of individuals with developmental disabilities. At the heart of positive behavior support is the person we are seeking to support. Our allegiance is to that person, requiring us to be person-centered while drawing from the most effective approaches science and our collective professional wisdom has to offer.
References
Carr, E. G., Dunlap, G., Horner, R. H., et al. Positive behavior support: Evolution of an applied science. Journal of Positive behavior Interventions 2002;4(1):4-16.
Bambara, L. M. Are you a behaviorist or a bonder? Smashing artificial dichotomies and entering into a dialogue of shared knowledge and multiple perspectives. Journal of Positive Behavior Interventions 2002;4(1):17-20.
Smith, T., & Iadarola, S. Evidence base update for autism spectrum disorder. Journal of Clinical Child & Adolescent Psychology 2015;44(6):897-922.
Barol | 13-26
Volume 8 ► Issue 1 ► 2019
Revisiting the Fourfold Positive Approaches Paradigm: Environment, Communication, Assessment,
and Hanging in There.
Beth I. Barol
Abstract
This article briefly reviews some of the advances in knowledge and treatment over the past 20 years for individuals with Intellectual Disability who have challenging behaviors. Revisiting the Positive Approaches Paradigm of “Environment, Communication, Assessment, and Hanging in There” the author explores the importance of continuing to focus on the compassionate education and training of the direct supporters to bring advances into the lives of people most in need of trauma-informed person-centered supports. She offers the Biographical Timeline process as one approach that can help transform the helping relationships, coordinate available resources and supports, and thereby assure positive outcomes.
Twenty-two years ago, the PA Positive Approaches Journal was launched with the intent to advocate for practices that would support people with behaviors that got in the way of living a fulfilling life. The journal was focused on sharing the successes and lessons learned in enacting the Positive Approaches fourfold paradigm: Environment, Communication, Assessment, and Hanging in There. Drawing on our original Positive Approaches article, the four elements of the paradigm are excerpted as follows1:

Environment: Most of the time when people exhibit challenging behaviors * we discover that a close look at that person’s environment shows us why the person is having difficulty. In roughly three-quarters of the situations in which we have been asked to consult, a person’s behaviors change for the better when they are helped to live in a manner that better meets their needs.
Communication: Often the person challenging us to understand cannot articulate wants and needs. Positive Approaches obliges supporters of a person with challenging behaviors to do whatever is possible to enable the person to communicate When a person cannot communicate, frustration becomes part of every interaction. When a person can communicate, the frustration disappears, and often, so does the problematic behavior.
Assessment: Even after the environmental and communication needs have been addressed, some individuals still evince challenging behaviors. Prompt assessment, diagnosis and syndrome- related treatment are vital tools in the Positive Approaches repertoire. Every concern that is relevant to typical citizens is also relevant to people with developmental disabilities. Problems such as trauma, loss, sexuality issues and abuse, loneliness, powerlessness, and addiction should be addressed.
Hanging
in There:
Even with all of the needed supports, opportunities, and conditions in place, a
person who has lived a life full of hardship, isolation, stigma, and sorrow may
have problems that continue for a long time. For those with the most serious
challenges, finding someone to persevere with them has proven difficult, once
found, that person has more impact on their lives than anything or anyone else.
As part of our drive for better person-centered assessment, we advocated for a rich appreciation of the impact of trauma on people’s lives, neurological differences, syndrome-based diagnosis, rather than the then predominant diagnosis only based on individual behaviors, diagnosis-based psychopharmacology rather than the practice at the time of using medications mainly for sedation and behavior control, and the relationship between physical health and mental health. We worked to broaden the array of effective treatments, interventions, and supports surrounding these issues without allowing the diagnosis of intellectual disability (ID) to automatically exclude diagnosis and treatment co-occurring mental and physical health issues.
Advances in Knowledge
The past 20 years has seen many advances in our knowledge about the brain, the brain/body continuum, trauma and its treatment, physical and mental health diagnosis, new medications, a better understanding of genetics, genetic testing2, and environmental factors as they relate to health and disability, to name a few. The array of treatment options that are effective for the neurotypical population has also grown, from a wider range of “talking therapies” to somatic therapies3,4 holistic health approaches, and neuro feedback5 and neuro entrainment; external stimulation to promote certain frequencies in the brain6,7. The possibilities expand on a continuous basis with very promising potentials to help people heal and recover from head injuries, traumas, neurological challenges and mental illness.8,9,10
However, as exciting as these new discoveries and innovations are, I have observed in my practice that there is still a wide gap between what is known or know-able and what is available to most of the population in need of these creative approaches. The gap between knowledge and practice is wider still for people who have intellectual and cognitive differences (i.e., ID). There are relatively few clinicians and practitioners who are skilled in the aforementioned advancements and are willing and able to offer their skills to people with ID. Many clinicians have told me that the diagnosis of ID continues to supersede any other assessment of root causes for the observed challenging behavior. They say that their clinical training has been to only offer behavior management as their primary treatment modality. We continue to focus on helping these clinicians broaden their assessment beyond the context of intellectual disability, noticing and addressing issues such as the wide array of mental illness, trauma, and neurological differences and applying promising practices, available to the neurotypical population to address the person’s specific issues.
In this article I will briefly focus on how the role of direct supporters is one of the key means to assure that many of the advances in knowledge and practice will become available to people with developmental disabilities. I will discuss the concept of the Social Therapist as the direct support person who, with training and support, implements promising practices, advocates for necessary services, and plays a vital role in the team. I will also describe how the use of a biographical timeline approach to transform a team’s view of a person, in conjunction with person-oriented trauma training, results in powerfully positive results.
The Social Therapist
Pivotal to the fourfold paradigm of Positive Approaches are the “social therapists.” This term, as used in this article, is an elaboration upon the wording as used by Anthroposophist, Karl Koenig through the curative education focus of the international Camphill Movement.11 A social therapist can be a family member, friend, direct care professional, teacher, supports coordinator, or any other person who comes in regular contact with an individual. Social therapists have the training and skills to intentionally gear interactions, environments, and activities towards the well-being, healing, and empowerment of those they are supporting.
Social therapists are, with the exception of the person they are supporting, the most crucial members of the team. They are the ones who deeply know the person, are attuned to the person’s rhythms, needs, joys, health, and relevant details in their daily lives. They are the people who help the person experience warmth and a positive mirror of themselves. They offer the opportunity for the person they support to feel known, emotionally held, safe to explore their environment, develop new skills, and grow when they are ready. A social therapist is skilled at timing, knowing when to press for opportunities for further growth, such as learning new skills and practicing mastered skills, and when to back off and offer supports to relax and unwind. They know when their immediate presence is necessary and when space and time to oneself is the preferable option.
Social therapists give vital information to the rest of the team to use when designing clinical and additional therapeutic supports. They help assure that the clinicians and other professionals have an opportunity to apply their valuable skill in a person-centered manner and they are the key to implementing a person-directed holistic support model, including attention to calming practices, exercise, and healthy nutrition on a daily basis. These are the people in one’s daily life who are trustworthy, dependable, present, and compassionate. Through their relationships, they provide the human environment where a person can flourish and an environment in which any additional therapeutic intervention has a chance to make a meaningful impact.
And yet, very often the direct supporters are not thought of as social therapists or those who have the potential to be social therapists. They are seen as “babysitters,” physical care givers, safety monitors, and enforcers. While there are many agencies, facilities, and providers of service that do focus on developing the social therapist, sadly, this vital component is overlooked by most. Staff training is focused more on meeting regulations and safety procedures than on inspiration, knowledge enhancement, creative approaches to everyday situations, role modeling and processing the day or week with an experienced mentor.
Through years of consulting and training nationally and internationally, I have observed a common theme. Direct supporters are often assigned to work with a person without knowing anything about the person except their challenging behaviors and the behavior plan to address these behaviors. In this experience, without training, ongoing mentoring and support, direct supporters are often left conceptualize their role as being responsible for containing or extinguishing the challenging behaviors without being afforded the opportunity to have the full context for these behaviors. Facing individuals with challenging behaviors on a regular basis without feeling that they have the skills or resources to feel safe and to make a positive difference can be very stressful, frustrating and intimidating for the support person. Their image of the person they are assigned to support often becomes one of a mean-spirited or manipulative troublemaker, or as someone who is totally different from anyone they can understand.
When this type of othering and demonizing occurs, there are several tools and processes that can be employed to help transform the relationship between the person being supported and their caregiver. One such tool is the Biographical Timeline, a process that helps transform the caregivers into a social therapist working on the behalf of the person.
The Biographical Timeline - Teaching to the Adult Learner
The Biographical Timeline is a tool that we use to achieve a deeper and more meaningful understanding of a human being who is struggling, and with whom we need to transform our relationship. In sum, the Biographical Timeline can be described as:
A tool that works best when the entire team is present and can together examine the information gleaned from records, interviews, and first-hand knowledge about the person. Events and personal experiences (often thought of as “insignificant” in other contexts) that were previously stored in compartmentalized reports and files, are grouped according to their occurrence along a linear life-timeline.12
The facilitator, who brings the team together, guides the group process, gleans the information from the participating team and use the opportunity to identify wounds (painful emotional and physical experiences), issues, and missed opportunities in the person’s life. Together they explore the meaning of these experiences and how they shape the person’s worldview, sense of self, and when relevant the person’s trauma story. This provides the facilitator, or members of the team, an opportunity to teach others about trauma, neurological differences, and mental illness as they relate to the subject of the biographical timeline. By filling in the knowledge-gap, the social therapists and other team members are better prepared to creatively come up with daily life supports and make specific treatment recommendations. The following two scenarios demonstrate the increased potential of social therapists when they have the opportunity to build compassion towards the person they struggle to support, in conjunction with training on elements specific to the person’s biography and issues.
Scenario 1
Eric was an 18-year-old young man who had very challenging behaviors. He would consistently hurt himself and lash out at others. A few weeks before his biographical timeline he had bitten one of his thumbs so severely that the doctors had to amputate it. After that, he was made to wear mitts on both hands most of the time. He was locked in his bedroom room day and night, because he was so violent towards staff, particularly women, often punching them in their faces if they were in his vicinity. His school refused to let him return to class due to his aggressive behavior. He was not verbal but had a creative sign language repertoire that he invented to communicate. Staff would often refuse to respond to his signs, insisting that he use the “correct” signs to communicate. His staff indicated that they were afraid of him and that they hated working with him. At the point of the timeline, he did not have any therapeutic program or a diagnosis other than “ID”. He was placed on antipsychotic medications for sedation, but according to the staff the medication was not effective.
The staff completed a record review prior to the biographical timeline meeting and the adoptive father also attended the meeting in order to fill in the knowledge gap about Eric’s early life. The story that unfolded was one of abandonment, and abuse and pain. He was dropped off at a hospital when he was one-day-old by a mother that was presumed to abuse alcohol. He never saw her again. He was then placed in a ward that was severely overcrowded, and afforded no individual attention, touch or comfort. He lived in a crib in that ward for the first year of his life. At this point we stopped the narrative and invited the staff to talk about early development and the possible ramification of this experience, neurologically and socially, supplementing the staff’s knowledge with mini lectures on development, trauma, and so on. The staff was moved by his experience and was able to compassionately talk about what he needed as a baby to have a better chance in life.
As the day continued, the staff saw that each stage of this child’s early life, before his eventual adoption by a caring family, was full of abuse and neglect. They were able to identify the effects of his traumatic experiences on his body, his responses to others, and his communication. They articulated how they now saw that their well-meaning, initial interventions were not tailored to his needs and his challenging behaviors increased as a result. As his fear-driven behavior issues escalated, the staff’s punitive responses escalated in return. It had never occurred to them that someone as scary as Eric could be afraid and just trying to survive.
After examining Eric’s life for a day and a half, the entire group listed the many painful emotional and physical wounds, issues, and missed opportunities in his life. They then moved into a brainstorming session where they excitedly postulated what it might take for him to heal and grow in the future, given their understanding of development and trauma. They then developed a very creative approach to his daily living. Several men volunteered to be his mentors observing what he enjoyed doing and introducing him to crafts and activities, including painting, pottery and gardening. They decided to learn his signs and work with him to add pictures to enhance their communication. They also decided to focus on developing trust and realized that it was their responsibility to become present and predictable. They decided to find out which affective styles worked with him and to pitch their responses to the affective mode that best met his needs. Their primary focus was going to be soothing, calming, and helping his body de-escalate from years of trauma. Later they shared their findings with the psychiatrist, who was in turn able to make an informed diagnosis and prescribe medication to address Eric’s anxiety rather than resorting to sedation medications.
Six months later, the staff was jubilant about the progress that they and Eric had made. No longer confined to his bedroom, Eric was spending time skateboarding and riding a bicycle, he was eating meals with his house mates, he was no longer aggressing against women on staff and even liked one or two. He was going outside and painting with one of the direct supporters (now social therapist) who was an artist. They discovered that he found pushing a heavy wheelbarrow in the garden to be a calming activity and so they included this in his daily routine. They all reveled in being creative and enjoyed working with Eric.
Scenario 2
Joey was a nice man. He was very social and loved being with people. While he couldn’t read or write, and he had trouble with articulation, he loved to talk with people. He was caring and would ask how the other person was doing, showing empathy in his responses. He would often say that he was upset. He would express being “scared” and worried though he was not always able to explain why. He would not want to be alone. There were other times when Joey was in his own world, he would shut himself in his room, he would yell, cry, and destroy his possessions. Sometimes he would wet himself. Sometimes he would wander off and get lost. Sometimes he would get cut while destroying a piece of equipment. He would often try to cover up what he had done with excuses, other times, he would just look blankly and say that he didn’t know what had happened.
Joey was often considered to be very competent. He was allowed to go out on his own all day. During those times, he would take public transportation independently, hang out in stores or the mall, and drink soda all day. Sometimes he would not come home when expected, having unexplainably have gotten lost, or forgotten where he lived. Once found, he usually had a distant, vague expression and affect, and would take a few minutes to hours to return to his usually friendly self. All change was unnerving for Joey. Staff change in particular was unnerving, he was afraid that he might again be victimized and neglected by new caregivers. He was afraid to say something that might anger staff, afraid that an angry person might abandon him, or abuse him, or send him away. It seemed to him that not answering accurately about what happened was the safest option.
The direct care staff didn’t know what to make of this. They were worried for him and afraid for their jobs when he did this. Despite being deemed to be able to spend time unsupervised, staff became strict and scolding when he didn’t behave in a manner that met their expectations. They would respond as if he had personally let them down when he would become upset, destroy property, hurt himself, yell or cry. They wanted to control his challenging behaviors. They wanted to force him to own up to his behavior with the idea that this would make him stop the behavior. “What did you do?” “Did you do that?”, they would ask using accusing voice tones. Their relationships spiraled downhill. Staff started to question if Joey should be hospitalized for self-harm.
The direct support staff did not know anything about Joey’s past, even though it was known to the agency directors. Perhaps they felt that the direct support staff did not need to know about the years of trauma and abandonment he had experienced from infancy forward, the multiple losses of loved ones, or his nagging fear that if things changed, he might end up back in an institution (an experience in his childhood that he hated and feared). Perhaps they thought, like many people in our field thought, that the past was not relevant to the present behaviors and intervention strategies. When the staff learned about elements of his life story and the array of traumatic experiences, they showed more empathy towards him, however they did not have appropriate training for trauma-informed care.
Joey then transferred to another agency with a different culture, and which also trained their staff on trauma-informed care and how to be social therapists. When they were given information about Joey’s history, they had the necessary tools to create an effective plan. Trained as social therapists, staff were able to recognize triggers and worked proactively to meet Joey’s need for warmth, predictability, and reassurance. They created opportunities to build his self-esteem and engage in meaningful activities. This informed approach had an immediate impact on Joey. He became clearer, more articulate, and much more relaxed. He enjoyed being with his social therapists, engaging in meaningful activities and practicing mindfulness in his daily life. He was also supported in making friends, something for which he had been searching for years.
As we saw in the two scenarios, staff may be left on their own without education, training or supervisory support, and yet we expected them to be able to effectively help the individuals they are supporting. Furthermore, many culturally normative child-rearing practices are counterproductive and unhelpful to the people who are overcoming trauma. Untrained staff may respond to challenging behaviors with the same harshness they may have experienced from their own caregivers and teachers to make them toe the line. They will often say “see, I turned out alright”, and credit the harsh treatment with their success. We need to consciously help staff see another way to get positive results without resorting to violent communication.13,14
Our staff training therefore needs to start with the basics of human interaction, non-violent communication styles, and affirmative relating, including bonding, attachment and rich communication. Direct supporters need to be taught the fundamentals of trauma and how it effects the body, the cognitions, and the emotions. They need to be able to brainstorm, with clinical support and guidance, and have the means to apply what they are now being exposed to regarding trauma and its treatment, to the daily, even hour by hour needs of the person they are endeavoring to support. They need to be able to talk about the style of interactions they want to pursue, drilling down to tones of voice for example, and the relevant activities that would further the person’s wishes and desires. They also need to explore together the helpful versus harmful use of power in their relationships with the individuals they support.
The well-trained social therapists understand that the health of the body directly affects the mental health of the individuals they support. They continuously seek the means to ensure that the healthy lifestyles recommended to all of us, to maintain health and to heal from so many physical and emotional issues are part of daily life: that people they support live in a healthy environment, eat a diet that supports their health, exercise daily, and have a good night’s sleep. They become versed in a variety of techniques that can sooth the autonomic nervous system and relieve stress, such as art, music, mindfulness, and yoga, and help incorporate them into daily life.
Summary
During the past 22 years there has been considerable advancement in our understanding of the root causes and treatment of many of the issues that affect us all. This includes an evolution of knowledge in our understanding of trauma, mental illness, and physical health. Bringing the benefits of these advances to the people we support is all of our responsibility. While we each need to continuously explore new knowledge and promising practices to best support people regardless of our role, we have to simultaneously realize that the most important people in the lives of the people we support are the social therapists. If we cherish them and assure that they have the knowledge, skill, and resources to create a healing environment, promote rich communication, and build the personal supports to enable them to hang in there for as long as possible, we will see the people we have struggled to support reap the benefits of these advances and live more fulfilling lives.
References
Barol, B. (1996). The Pennsylvania Journal on Positive Approaches: An overview. Positive Approaches.Vol1. No.1 pp.1-3.
Finucane, B., Haas-Givler, B, & Simon, E. (@)16). Knowledge and perceptions about Fragile X Syndrome: Implications for diagnosis, intervention, and research. Intellectual and Developmental Disabilities.5(4) 226-236.
Levine, P. A. (1997). Chapter 13: Blueprint for repetition. In Waking the tiger: Healing trauma: The innate capacity to transform overwhelming experiences (pp. 173-191). Berkeley, CA.: North Atlantic Books.
Rothschild, B. (2000). The body remembers: The psychophysiology of trauma and trauma treatment. New York, NY: Norton.
Fisher, S. (2014). Neurofeedback in the treatment of developmental trauma. New York, NY: Norton & Company.
Joyce, M. & Siever, D. (2000). Audio-visual entrainment program as a treatment for behavior disorders in a school setting. Journal of Neurotherapy, 4,(2), 9-25.
Collura, T. & Siever, D. (2009) Audio-visual entrainment in relation to mental health and EEG. In J.R. Evans & A. Abarbanel (Eds.) Quantitative EEG and Neurofeedback (2nd Ed.) (pp. 155-183) San Diego, CA: Academic Press.
Doidge, N. (2007). The brain that changes itself: Stories of personal triumph from the frontiers of brain science. New York, NY: Penguin Books.
Doidge, N. (2016). The brain’s way of healing: Remarkable discoveries and recoveries from the frontiers of neuroplasticity. New York, NY: Penguin Books.
van der Kolk, B. (2014). The body keeps the score: Brain, mind, and body in the healing of trauma. New York, NY: Penguin Books.
Root, W. Social Therapy, the Fellowship, Youth Guidance. AnthroMedLibrary.
http://www.anthromed.org/Article.aspx?artpk=492. Accessed February 25, 2019.
Barol, B. (2001). Learning from a person’s biography: An introduction to the Biographical Timeline Process. Positive Approaches. Vol.3 No. 4 pp. 20-29.
Rosenberg, M. (2003). Nonviolent communication: A language of life. Encinitas, CA: Puddle Dancer Press.
D’Andrea, W., Ford, J., Stalbach, B., Spinazzola, J., & van der Kolk, B. (2012). Understanding interpersonal trauma in children: Why we need a developmentally appropriate trauma diagnosis. Journal of Orthopsychiatry, 82, 187-200.
Knoster | 27-34
Volume 8 ► Issue 1 ► 2019
Providing Individual-Intensive Positive Behavior Support: Do the Ends Justify the Means or Do the Ends and Means Need to be Mutually Justifiable?
Tim Knoster
Abstract
Providing multi-component Positive Behavior Support with children, youth and adults with complex histories of social-emotional-behavioral challenges continues to be perplexing across school, home and community settings. There are various, inter-related reasons behind the perplexing nature of providing such supports that extend beyond the unique needs of each individual in need of individualized Positive Behavior Support. To this end, and as a way to provide some food for thought and perhaps challenge to the field, the following highlights a series of guiding questions for consideration when providing individual-intensive Positive Behavior Support.
___
In 2008, Nancy Weis and I published an article in the Journal of Positive Behavior Interventions entitled “It May be Non-aversive but is it a Positive Approach?”1 In that article, we provided a series of questions to consider when providing individual-intensive behavioral assessment and subsequent interventions and supports. Many of those questions continue to be germane today. However, the questions we posed at that time should be further informed today through the integration of the increasing body of knowledge that continues to emerge concerning social-emotional-behavioral wellness and trauma informed approaches. To this end, the following questions are intended to provide important ethical considerations for those of us involved in various forms of behavior change endeavors.
Has the Person Experienced Adverse Childhood Experiences and Trauma?
A growing body of literature highlights the negative impact
that adverse experiences early in life can have on physical, social, emotional
and behavioral wellbeing long-term2,3,4,5,6.
Adverse Childhood Experiences (ACEs) have been associated with poor health
outcomes and lowered quality of life. In this same vein, trauma has as well
been linked to undesired outcomes. Chronic exposure to trauma (such as repeated
exposure to abuse) can lead to toxic stress that can profoundly alter growth
and healthy development. The seminal ACEs Study7 identified
three types of ACEs with these three ACEs further broken down as follows:
|
Abuse |
Physical Emotional Sexual |
|
Neglect |
Physical Emotional |
|
Household Dysfunction |
Presence of Mental Illness in the Home Mother Treated Violently Divorce Incarcerated Relative Substance Abuse |
More recent examples of ACEs have been expanded to include Foster Care Placement, Exposure to Harassment & Bullying, Death of Parent/Caregiver, Forced Separation from Caregiver, Life Threatening Illness, Experiencing Violence, and Exposure to Discrimination. It is important to consider screening for ACEs and exposure to trauma in light of the impact that these factors have on healthy growth and development. To this end, alignment (if not integration) of behavioral technologies with evidence-based approaches that support what is increasingly being referred to as trauma informed practice is highly encouraged.
To What Degree Does the Person Have Opportunities to Make Meaningful
Choices
Throughout the Ebb and Flow of a Typical Day?
Many ethical issues related to behavior change programs revolve around issues of self-determination and locus of control. There can be an inherent imbalance of power whenever one person who has greater authority endeavors to alter the behavior of another person with less autonomy. The natural inclination of many caregivers and service providers when working with a person with behavioral challenges is to limit choice opportunities in the individual’s daily routine. As alluring as this can be in the short term, it can create longitudinal challenges when we consider that the best way to teach someone to make “good” choices requires naturally occurring opportunities to learn to make meaningful choices. This is not to suggest that structuring choice opportunities when teaching decision-making skills is ineffective or near sighted. Rather, the focus should be on how to structure such instructional situations in a manner that does not inadvertently limit choice opportunities to trivial matters as opposed to more personally meaningful age appropriate opportunities (e.g., choosing to complete as task or go to “time out” vs. providing opportunities in task sequences to allow the person…based on how resilient s/he is feeling that day…to exert influence over what they do first and what they do last – presuming of course that the tasks to be completed has some degree of value/importance from that person’s perspective).
How Do We Minimize the Likelihood of Future Problem Behavior?
Exclusive application of short-term consequence procedures, or the delivery of reactive consequences following problem behavior, unfortunately continue to be a primary emphasis in many behavior-change endeavors today. To be clear, consequence strategies certainly have a place in behavior change programs…but just one place in a multi-component approach that places greatest emphasis on prevention through proactive environmental changes in tandem with teaching an array of alternative skills (replacement behavior, general skills and self-regulatory/coping skills). Understanding the function of the person’s behavior, through functional behavior assessment culminating in the development of hypothesis statements from which to design a Positive Behavior Support Plan, best positions caregivers and service providers to emphasize prevention through environmental changes in tandem with promotion of prosocial skills thus reducing over reliance on reactive consequence in response to undesired behavior. Consideration of the personal history (or narrative) of the person should be incorporated within the assessment process to increase sensitivity to trauma that may have been previously experienced. This should also facilitate alignment or integration of multi-disciplinary approaches in a person-centered manner.
How Will Our Actions Impact Personal Wellness and Quality of Life of This
Person, His/Her Family and Friends,
and Others Who Directly Interact with this
Individual on a Regular Basis?
One significant shortcoming of traditional behavior
management approaches that primarily emphasize reduction in problem behavior is
that they can come at a cost to personal relationships and impede the person of
concern from realizing a sense of belonging inclusive of feeling valued by
others. Certainly, reduction of problem behavior is one desired outcome through
the application of Positive Behavior Support. However, reductions in problem
behavior actually become a constructive byproduct of adjusting environmental
factors that trigger problem behavior in concert with teaching an array of more
habilitative alternative skills (or behaviors). In this sense, the primary
focus of Positive Behavior Support is on understanding the person’s behavior in
context of that person’s personal history and his or her goals and aspirations
for the future. Asking questions such as the following can help to gain
perspective and insight that is valuable:
|
Who is this person? |
|
Given the full range of options that typical same age peers have, what would this person choose to change about his/her life circumstances? |
|
What has changed about this person’s life circumstances that may be inconsistent with his/her personal goals or aspirations? |
|
With whom does this person have meaningful relationships and with whom would this person desire to have more meaningful relations? |
True application of Positive Behavior Support is more than the linear application of scientifically validated behavioral technologies. Rather, it is the application of those technologies in a manner that reflects personal understanding, empathy and focus on the longer term. In essence, Positive Behavior Support is about supporting individuals on their personal journey towards social, emotional and behavioral wellness.
How Will We Measure Progress in Terms of Both 1: Fidelity of Implementation
(Treatment Integrity)
and 2: Impact of Interventions?
There are two primary facets of meaningful assessment related to implementation of Positive Behavior Support. The first is that of ensuring the integrity of implementation of the designed multi-component behavior support plan. This requires stakeholders…those that will be directly impacted through implementation of the support plan… to self-monitor their implementation of 1) short-term prevention through environmental changes; 2) delivery of proactive instruction in a) the replacement behavior, b) general skills and c) self-regulatory or coping skills; 3) consequence strategies (both reinforcement of desired behavior and redirection of undesired behavior), and 4) long term prevention through strategies to a) increase meaningful choice opportunities, b) maintain and generalize learned alternative skills, c) address chronic health concerns (as relevant), and d) enhance personal connections and relationships with others based on common interests. The degree to which meaningful gains can be realized are, in large part, dependent on the integrity of implementation of the agreed upon strategies across these four component parts of the multi-component support plan.
The second facet of meaningful assessment associated with the delivery of Positive Behavior Support emphasizes impact in terms of socially valid outcomes. Measuring progress and outcomes in this regard focusses on 1) reductions in problem behavior, 2) increases in use of alternative skills and 3) improvement in quality of life. Each of these three domains of impact should be viewed as inextricably connected to best ensure that progress and outcomes realized are truly meaningful as well as sustainable.
In summary, the design and delivery of Positive Behavior Support requires applying scientifically supported behavioral technology in a manner that is firmly grounded in person-centered approaches that take in to account both the person of concern’s personal history…his or her life narrative…as well as his or her goals or aspirations for the future. Certainly, this differs in terms of age appropriateness when providing Positive Behavior Support (e.g., with a six-year-old child as compared to a sixteen or sixty-year-old individual). However, at the core, the basic tenants highlighted through these guiding questions best position us to ensure that the ends of behavior change and the means (our application of behavioral support strategies) are mutually justifiable
References
- Weiss, N., & Knoster, T. (2008).
It May Be Nonaversive, But Is It a Positive Approach? Relevant Questions to Ask Throughout the Process of Behavioral Assessment and Intervention
- Anda, R.F., Felitti, V.J. , Bremner, J.D. , Walker, J.D. , Whitfield, C. , Perry, B.D. , et al. (2006). The enduring effects of abuse and related adverse experiences in childhood. A convergence of evidence from neurobiology and epidemiology. European Archive Psychiatry Clinical Neuroscience; 256 (3): 174 – 86.
- De Bellis, M.D., & Zisk, A (2014). The biological effects of childhood trauma. Child Adolescent Psychiatry Clinic; 23 (2): 185 – 222.
- Kuehn, B. (2014). AAP: toxic stress threatens kids’ long-term health. JAMA; 312 (6): 585 – 6.
- Shonkoff, J.P., Garner, A.S. (2012). Committee on Psychosocial Aspects of Child and Family Health; Committee on Early Childhood, Adoption, and Dependent Care; Section on Developmental and Behavioral Pediatrics. The lifelong effects of early childhood adversity and toxic stress. Pediatrics; 129 (1): e232 – 46.
- Hertzman, C. (2013). The significance of early childhood adversity. Pediatric Child Health; 18 (3): 127 – 8.
-
Felitti, Vincent J; Anda,
Robert F; et al. (May 1998). "Relationship
of Childhood Abuse and Household Dysfunction to Many of the Leading Causes of
Death in Adults: The Adverse Childhood Experiences (ACE) Study". American Journal of
Preventive Medicine, 14 (4):
245–258.
Legare | 35-48
Volume 8 ► Issue 1 ► 2019
Positive Approaches & The Wisdom of Herb Lovett
Guy Legare
Abstract
In Positive Approaches & the Wisdom of Herb Lovett, the author, by revisiting an article written almost twenty years ago, explores how something seemingly so simple, listening, requires mindfulness, feedback, humility and ongoing practice. The implications from years of outcome research are shared and cannot be dismissed; the person you are trying to help is the engine of change. Simple and practical ways of getting regular feedback are discussed to help anyone interested in learning to listen, integrate the art and the science of being helpful.
“Of all tyrannies, a tyranny sincerely exercised for the good
of its victims
may be the most oppressive…those who torment us for our own good
will do so
without end for they do so with the approval of their own
conscience…
This very kindness stings with intolerable insult.”
– C.S. Lewis
It was exciting to hear that a group of people from the Office of Developmental Programs (ODP) and Office of Mental Health and Substance Abuse Services (OMHSAS) in Pennsylvania were working toward reviving the Pennsylvania Journal on Positive Approaches. Being invited to contribute and offer an occasion to revisit an article submitted almost twenty years ago as a way to reconnect with the spirit of Positive Approaches, is a wonderful opportunity to reflect on how it influenced my ability to listen over the years, how it helped me be present and helpful with others is simply great timing.
In one issue of the original Pennsylvania Journal on Positive Approaches in 2000, a good friend, Susannah Joyce and I collaborated on an article titled: Remembering Herb Lovett 1. Two years before in 1998, Herb had died in a car accident on his way home from work he was doing in New Hampshire at the time. Years before, when Herb was in Pennsylvania facilitating some workshops and working with small groups, supporting the work of dedicated people who were involved in supporting people with challenging behaviors, he was asked to give these events a title and he simply suggested “positive approaches for people with difficult behavior.” All of a sudden, Positive Approaches was born2.
It is impossible for me to think about Positive Approaches without reconnecting with the times I shared with Herb and what I learned from him. Like many others whose lives were touched and transformed by Herb, I believe that both Susannah and I were deeply impacted and transformed by Herb’s capacity for empathy and the way he could attune himself to and be with another person. At the time, as Susannah wrote, we discovered that even between ourselves it was not that simple for us to convey what we felt or all we had learned from Herb. We were simply hoping to share through some personal reflections and stories, some of the gifts and wisdom we had received from Herb and in turn try to stay connected with the spirit of Positive Approaches; to this powerful yet inhabitual way of being with others while trying to listen and help them.
Susannah described beautifully how Herb would try to listen to the person first, be present, even when people were very difficult, appreciating their experiences and the context of their lives. She also wrote about how Herb was constantly inviting others to connect first person to person, while providing respectful and effective clinical expertise to the team supporting that person when needed.
Although I could not articulate it clearly at the time we initially wrote this article as I believe I could do today, I had started to realize that developing a relationship with someone, one based on equality and mutual respect was, as Susannah wrote, the context and the true vehicle for any “help.” In sharing James’s story, someone who I found very challenging to support and help, I was focused on describing how Positive Approaches turned out to be a powerful awakening for me. I had first met James, a very smart, funny and cynical 43-year-old man in 1991. During the previous 25 years, he had been admitted more than 20 times to a large psychiatric institution in our community. Over a period of several months a group of clinicians were involved in developing with him the supports he needed to stay out of the psychiatric facility and successfully live in the community. Despite our best efforts to listen and support James, it became a frustrating experience for everyone involved, especially for James. Positive Approaches allowed me to reconnect with James in ways that I could not have imagined. When I finally heard James and realized I had unintentionally been getting in the way, it transformed the conversation I had with him and my ability to partner with James. What wasn’t as clear to me at the time was why it took me so long to hear him and appreciate something that then became so obviously simple.
In the foreword of Herb’s second book, Learning to Listen: Positive Approaches and People with Difficult Behaviors, Nancy R. Thaler3 who knew Herb well, described two important aspects of the work Herb was doing in Pennsylvania. She explained how he was introducing a new way of thinking and how he was fostering an openness to doing things differently. She also shared how Herb, through personal stories, reflections on his own thinking and actions, would gently expose the harm being done in the name of treatment. Herb would do so without demeaning our past efforts to help and allow us to face the truth about the possible impact of our actions without debilitating embarrassment or shame. Nancy went on to write: “Here the truth was we’d been hurting some people instead of helping them. In fact, we’d been hurting them in the name of helping them.”3
Herb was gifted at presenting the truth in ways that others could see and accept. He would often present information with humor and create an opportunity for the listeners to consider something important he was suggesting, something painful we were unintentionally doing, something we may need to change to be more helpful from the person’s perspective. In 1992 during a two-day workshop Herb was facilitating in New Brunswick, Canada, I heard Herb say something that really resonated with me: “The day I realized as a psychologist I was my clients’ biggest problem, they all started to do a whole lot better.”
At the time of his presentation like many others attending, I smiled and laughed when I heard him, appreciating his humor and wit. I thought about this profound and wise statement often the last twenty some years. I wish I could have a conversation with Herb about this, what it meant to him, how that realization actually happened for him and how he was able to use these lessons to help him learn to listen, be present and connect empathically with others. This would be I am sure, a fascinating conversation.
Similarly, I also have thought about James’s story over the years. I wasn’t, and am not a bad person, I was well intentioned, I was passionate about helping, about making a difference in people’s lives and I was just trying to assist James in having a stable and meaningful life in the community, away from the psychiatric facility he was so often visiting. I was not actively hurting James, but for seven months while I was simply trying to help him, sadly and painfully, I did not really hear him, and I had no idea that was happening.
It was a true gift to meet Herb years ago since it literally changed my life. Of all the things I learned from Herb, two in particular have stood the test of time. They are present in my mind every day, important reminders of what I need to be mindful of when I am trying to listen and hear someone. I have always believed these two critical lessons to be at the core of what Herb called Positive Approaches:
- Despite my best intent as a helper, I could unintentionally be dismissing someone and not knowingly, be doing something that the person is experiencing as frustrating, unhelpful or hurtful. This was a big part of what happened with James.
- To implement and practice what Herb was teaching, I would have to be humble, recognize and be comfortable with the fact that I am the one who will first have to change the way I am thinking and acting in order to connect more meaningfully with someone as a person, hopefully becoming more helpful with them. It is only when I started to look at James and his life differently that it became possible for me to consider another possibility.
I am truly grateful for the opportunity to share some reflections on Positive Approaches in the new version of this journal, to consider the art and science of being helpful with individuals we find challenging to support, share some thoughts on how Herb is still influencing my life today and how it has led over time to simple daily practices that are transforming me and others personally as well as professionally.
The Art Being Helpful: Learning to Listen
“The world as we have created
it is a process of our thinking.
It cannot be changed without changing our
thinking.”
– Albert Einstein
If I were sharing James’s story today, the emphasis would be on helping others appreciate how much of a gift these kinds of experiences are and how transformative they can be if you take the opportunity to learn from them. James was one of the first few times I had that kind of humbling and transforming experience, but it wasn’t the only one, it was only the beginning of a long learning process for me. This journey the last twenty years has been surprising, sobering, exciting, sometimes painful, difficult, yet very powerful and always meaningful. Since that initial awakening with James, I have been interested in better appreciating why it took me so long, seven months, to hear something that was so obvious once I heard him. Ever since, I have been obsessed with the idea of learning to listen and curious about understanding why something seemingly so simple as listening is actually so much harder to do in practice. I started to explore the following questions:
- How can I be listening to someone without hearing them?
- How is it that in the name of helping him over a period of seven months, I also unintentionally created multiple subtle experiences where James’s identity, feelings, needs, preferences or experiential reality could also be invalidated?
- How could I unintentionally spend so much time with someone, simply trying to listen to and also unknowingly create an outcome where James could be dehumanized as a partner and fellow human being?
- How is that possible?
- What could I do differently?
It made sense at the time to continue exploring these
questions within the context of Positive Approaches since these powerful
learning experiences were possible because of the transformation I was
experiencing implementing it. As Nancy Thaler wrote2 the name Positive Approaches communicated a
stance, an attitude, a set of values that should direct what approaches we take
in supporting people. The approaches themselves were many.
A really good friend, Beth I. Barol, PhD offered an overview4 of Positive Approaches in the premiere issue of the Pennsylvania Journal on Positive Approaches, a quarterly publication created to help people with developmental disabilities and challenging behaviors live fulfilling Everyday Lives. Beth reminded everyone at the time that Positive Approaches was a worldview, one where everyone is treated with dignity and respect. She also introduced the Positive Approaches paradigm, an attempt to conceptualize and organize this worldview in terms relevant to all interacting and supporting individuals we found challenging. The paradigm was a helpful way to organize all these different approaches and perspectives into four major areas: Environment, Communication, Assessment and Hanging in There4.
For years I believed I simply needed to become more knowledgeable, practice, pay attention, be mindful and honor what I was learning. I spent a lot of time learning various helpful perspectives or approaches and what I eventually referred to as lenses. The goal was to develop the flexibility and knowledge I thought I needed to be able to explore multiple possibilities, to navigate the four major areas of the Positive Approaches paradigm competently so I could respectfully, based on need, look at things and people differently.
My hope was that all this knowledge would help me improve my ability and capacity to better appreciate someone else’s experience and connect empathically with them in a deeper way. It was important to look at someone’s quality of life; at how they are spending their days; at how lonely and disfranchised the person could be; at how little control someone might have over their life; at what they could be communicating; at how dual diagnosis, trauma, their biography and history could be impacting their ability to have the life they want; how sensory issues could affect someone, how pain or medical conditions could influence the person, etc. There was something very helpful in learning to appreciate how all these lenses were helping me understand various aspects of the person’s life. This indeed helped me assist teams and provide respectful and effective clinical expertise when it was needed.
What I also learned from people during those years is that all these lenses and approaches actually got in the way and did not really help me connect with people in a deeper empathic way. In fact, I started to realize that even though these lenses can help you focus, help you see something new, all these lenses, when you adopt them, come with some risks. It is important to know that they also limit what you can see and hear when you chose to use them. For example, when I start to think that the person may be showing signs and symptoms of a mental health issue, it is hard to focus on something else. It is also easy to forget that as human beings, we have a tendency to search for, interpret and favor information in a way that confirms one’s preexisting beliefs or hypothesis.
I became increasingly aware that when I was looking at, or listening to someone through these lenses, when I was trying to interpret, assess, evaluate or make sense of what I saw and heard through them, I actually was not listening to the person. I was busy thinking, trying to make connections but I was not present with them, not really listening to their experiences, especially appreciating how I could be impacting them in the name of helping.
The larger lesson I was learning was not just about the value of these lenses or approaches, but much more about how I was using them in the moment with someone. It became clear that I also needed to pay attention to my own thinking, I needed to become much more aware of the choices I was making in the moment when listening to someone. To be able to really move from control to empathy and true collaboration, I would really need to increase my awareness of how my own needs and thoughts (in the moment) could shape and influence what I saw, heard and understood. I needed to develop and practice the kind of mindfulness and presence that I could use to develop a deeper empathic connection with someone. So I started exploring different kinds of questions:
- What kind of practices could help me grow and become more attuned to others in the moment?
- What can I practice daily that would decrease the likelihood that I might unintentionally recreate that experience with someone I am supporting and trying to help?
- What kind of safeguards can I put in place to ensure I first really connect with the person?
- How could I make sure (as Herb would say) that I would never be or become the person’s biggest problem?
- More importantly, how would I know in the moment that I am listening, that I am helpful?
Looking back again at James’s story, seven months in and because I
felt frustrated and had no clue what else I should do, out of desperation I
asked James what he thought and asked him for help. Today I cannot help but wonder
how much sooner I would have been able to hear him, had I been present, aware
that I could be his biggest problem or if I had simply checked in and asked him
how helpful I actually was.
The Science of Being Helpful: Being Driven by Feedback
“Divorced from systemic, reliable, and valid feedback about
the process
and outcomes (subjective experience of the person) for almost
everything we do,
the field has become a jumble of competing, complicated and
often
contradictory approaches to treatment, services and supports.”
– Institute for the Study of Therapeutic Change (ISTC), 2001
In the early 1990s, Mark Hubble, Barry Duncan and Scott Miller, three clinicians, got together and started to collaborate in an effort to share helpful information about what works in therapy based on the lessons learned from the important work of outcome researchers the last previous years. The Institute for the Study of Therapeutic Change (ISTC) was created. Eventually, their work led to the publication in 1999 of the first edition of The Heart & Soul of Change: What Works in Therapy5. The second and updated edition The Heart & Soul of Change: Delivering What Works in Therapy6 was published in 2010. As editors, they assembled the best outcome researchers and practitioners and summarized what works in psychotherapy and how to best deliver it.
The outcome research was challenging the prevailing view that to be an accomplished psychotherapist one must be well versed in evidence-based treatments (EBTs) or in those models that have been shown in randomized clinical trials (RCTs) to be efficacious for different “disorders.” In reality, the role of various models or approaches as a specific factor in the change turned out to be minimal.
The implications from years of outcome research are clear and cannot be dismissed; the person you are trying to help is the engine of change.5,6,7 Therefore, the person’s perspective and involvement in the planning and delivery of how we do what we do to help them, is absolutely critical. It suggests that as helpers we need to take our direction from the person, follow their lead, accept (when it is safe to do so) the person’s goal and also have a way for the person to confirm that what we do is actually helpful for them.
From this perspective there are no a priori assumptions about the person or challenging behaviors, or solutions, no special questions or series of questions that are best to ask, and no invariant or systematic methodology that needs to be followed. Rather, as a support person or a helper, you follow the person’s lead, listening intently and carefully. The person’s perception of the problem and what would be helpful is what really matters in all this.
Early on the Institute for the Study of Therapeutic Change (ISTC) developed the Session Rating Scale (SRS) and the Outcome Rating Scale (ORS) to help clinicians appreciate the person’s perspective on all this. Both the SRS and ORS are simple four item scales. They are actually soliciting the person’s perspective or feedback regarding factors proven to predict success, regardless of the population, treatment modality, or presenting problem. Both are simple measures a therapist could use to quickly get feedback from the person every time they met5,6,7,8.
Since then, these simple measures were implemented, tested, evaluated and eventually validated. They became part of a larger outcome management system: The Partners for Change Outcome Management System (PCOMS)9,10. The Substance Abuse and Mental Health Administration is now listing PCOMS as an evidence-based practice. It is different from what is usually considered evidence based because feedback is a theoretical and therefore something you can add to any therapeutic orientation or approach and it can apply to people and clients of all diagnostic categories11. The work being done to help someone is literally feedback informed and driven.
The use of these scales is helpful but the conversation that should ensue with the person once you genuinely ask for feedback is what has the potential to transform your abilities and effectiveness as a helper. Having the person rating how well you are doing as a helper and how effective you are can be scary and it is a powerful act. This brings the person’s voice back in the partnership as long as the helper you can receive the feedback you sought as a gift. Feedback is a gift since it allows us as helpers to adjust and correct what we do quickly, to attune to the person’s preferences, it allows us to focus on the quality of the relationship and maximizes the person participation in the partnership. Soliciting systematic feedback and the opportunity for real conversations it creates provides a transparent, ongoing interpersonal process that solicits the person’s help in creating the necessary partnership and collaboration to ensure a positive outcome.
Today, when I reflect back on the journey I embarked on since I first met James and the search for a way to ensure that I would not become someone’s biggest problem when trying to help, seems so obvious. The key was simply to be mindful and attentive to the feedback from James and be humble enough to simply check in with him to ensure that what I believed was happening was also what he was experiencing. Had I been able to do this at the time, it would have allowed me to appreciate the impact I had on him; it would have been an early-warning system, giving me a chance to adjust quickly, maybe chart a different course with him, minimize his frustration, increase the likelihood we were going to reach the outcome we were both hoping for sooner and in the process to boot, assist me in becoming a better helper.
Final Thoughts
We collectively as a system have changed a lot since Herb was last here in Pennsylvania. However, most systems of support or helpers still have a tremendous amount of influence or power over the people who need assistance and supports. This power can be visible and obvious, but it is more often hidden and communicated through assumptions, language, and expectations. Even though we mean well, we have learned that what we do in the name of helping often unintentionally creates conditions where the people we are trying to support also experience situations where their most basic human needs are not being met.
When most of us start in this field we are convinced that we have the best intentions when we are trying to help. Very few of us have had the opportunity to realize and appreciate that the person’s responses to what we do are often the only way they have to let us know that even though we mean well, our actions and what we do to help them, is actually not that helpful for them. Over the past twenty years I have often experienced that even with the best intentions to help, my words and actions often have unintended consequences. Examining how you might unintentionally be contributing to the person’s problems when you are convinced you are only trying to help requires a willingness to learn; it can be hard work, but it is also exciting and rewarding.
In the preface of his second book, Learning to Listen: Positive Approaches and People with Difficult Behaviors3, Herb was already recognizing that naming this attitude, this way of thinking, this way of speculating empathically or this way of life where one, as a helper, moves from control to collaboration was a mixed blessing. Herb understood that nothing named can hope to remain the same and that new names and phrases always run the risk of becoming spiffy euphemisms for “business as usual”3. What Herb feared is exactly what happened. Over the last twenty years from my point of view, it seems like we have gradually shifted towards a more clinical perspective in nature. We have unintentionally lost sight of the importance of truly being present with someone, of listening deeply to another and to fully appreciate the transforming power of empathy and collaboration. In the original article1, Susannah shared a powerful story about Herb at his best, listening, present and Michael, a young man who was living in a large mental health institution. Herb had started a circle of support a few years before to help Michael find a meaningful life in the community. She described how one afternoon while they were out with Michael, sitting at a picnic table in a park, planning how to best support Michael, sharing sodas and fries, Michael started to sob. In response Herb put his arm around Michael, held him for many minutes before they had to leave and bring Michael back to his ward. Herb offered him what comfort he could in an impossible situation; everything else Herb did trying to help, sprang from that center of compassion.
It is my hope that restarting The Pennsylvania
Journal on Positive Approaches will not only be an opportunity to explore and
celebrate best practices but more importantly, to revisit and reconnect with
the spirit of exploration; to honor the feedback the people are always offering
us about how helpful we are; to reconsider the possibilities we know exist
beyond a clinical lens and to continue getting better at working with – rather
than on – people.
References
- Legare G, Joyce S. Remembering Herb Lovett. The Pennsylvania Journal on Positive Approaches. 2000; Volume 3, Number 1, pp 10-13.
- Thaler N. The Beginning of Positive Approaches in Pennsylvania. The Pennsylvania Journal on Positive Approaches. 1997; Volume 1, Number 2, pp 1-2
- Lovett H. Learning to Listen: Positive Approaches and People with Difficult Behavior. Brookes Publishing, Toronto. 1996
- Barol BI. The Pennsylvania Journal on Positive Approaches: An Overview. The Pennsylvania Journal on Positive Approaches. 1996; Volume 1, Number 1, pp 1-3.
- Hubble MA, Duncan BL, Miller SD. The Heart and Soul of Change. American Psychological Association. 1999.
- Duncan BL, Miller SD, Wampold BE, Hubble MA. The Heart and Soul of Change: Delivering What Works, 2nd Edition. American Psychological Association. 2010
- Bohart A, Tallman K. Clients: The Neglected Common Factor. In B. Duncan, S. Miller, B. Wampold, & M. Hubble (Eds.), The Heart and Soul of Change: Delivering What Works (2nd ed.,) Washington, DC: American Psychological Association Press. 2010; pp 83-111.
- Miller S, Bargmann S. The Outcome Rating Scale (ORS) and the Session Rating Scale (SRS). Integrating Science and Practice. 2012; Volume 2, Number 2, November, www.ordrepsy.qc.ca/scienceandpractice
- PCOMS Information: Better Outcomes Now - https://betteroutcomesnow.com. 2019. Updated October 1, 2018.
- PCOMS Information: Center for Clinical Excellence (ICCE) - https://www.centerforclinicalexcellence.com. 2019.
- Duncan B. The Partners for Change Outcome Management System (PCOMS): The Heart and Soul of Change Project. Canadian Psychology. 2012; 53, pp 93-104.