Positive Approaches Journal, Volume 8, Issue 2
| Site: | My ODP |
| Course: | My ODP |
| Book: | Positive Approaches Journal, Volume 8, Issue 2 |
| Printed by: | |
| Date: | Wednesday, June 24, 2026, 12:37 PM |
Positive Approaches Journal | 5

Volume 8 ► Issue 2 ► 2019
Meaningful Community Engagement
Introduction
As we strive to support individuals with disabilities to live an Everyday Life, one crucial facet for consideration is meaningful engagement with one’s community in which relationships are built, sense of purpose is developed, and quality of life
is enhanced. In 2001, Metzel and Walker highlighted that “physical inclusion has not brought about social inclusion, full community membership and belonging and valued social roles for people with disabilities.”1 Almost 20 years later,
we continue to have these conversations about truly increasing community engagement and social inclusion for individuals with disabilities. As a service system, we have made great strides in increasing community presence, but we have much more
work to be done to achieve full community engagement. Being seen in everyday places is a start, but it does not guarantee that one feels connected or that one belongs. Encouragingly, the topic of community engagement or community participation
has been explored in mental health, autism, and intellectual disability research and has been gaining momentum; however, research findings have supported that individuals with disabilities are more socially isolated than their non-disabled peers
and are less likely to engage in their communities to the degree that they would prefer (Orsmond et al, 2013; Thomas et al, 2017; Amado et al, 2013). On a positive note, research has begun to demonstrate encouraging results in increasing community
inclusion and the development of relationships with community members for individuals with disabilities using a variety of strategies (Amado et al, 2015). Identifying the strategies that are the most effective in promoting community engagement
and social inclusion will help propel us forward. In this issue, authors provide the necessary insight, experiences, and recommendations to guide us in our work to support individuals with intellectual and developmental disabilities and
mental illness to engage in their communities in ways that are meaningful to them.
—Pamela Treadway, M. Ed.
1D. Metzel and P. Walker (2001). The illusion of inclusion: Geographies of the lives of people with developmental disabilities in the United States. Disability Studies Quarterly, 21(4): 144-128.
Positive Approaches Journal | 6
Volume 8 ► Issue 2 ► 2019
Data Discoveries
The goal of Data Discoveries is to present useful data using new methods and platforms that can be customized.
Participating in communities is an important part of everyday life that allows us to meet new people, learn, and grow. Communities may be our families and our homes or where we live. Communities can also be our building, block, or neighborhood. Whether you live in a city or on a farm, being a part of our communities helps us meet new friends and learn about other people and ourselves.
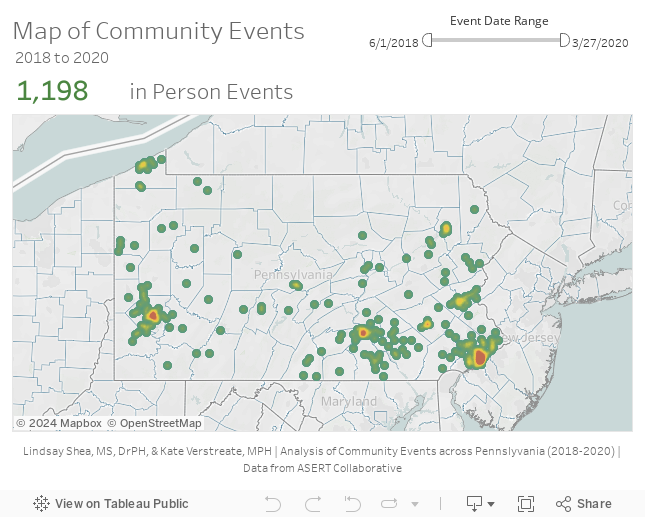
In this issue, Data Discoveries presents a map of one type of participation in communities: community events gathered by the Autism Services, Education, Resources, and Training Collaborative (ASERT). Each dot on the map represents a zip code where an event or multiple events were held or will be held (through 2020). This map is a heat map, where multiple events are represented by changing colors of the dots, moving from green for one or fewer events to red for many events. Hovering over the dots also displays a bar graph displaying the number of community events within each zip code, within each the county, and compared the statewide average by zip code. A slider bar for date ranges is in the upper left hand corner to allow you to filter the dates between 6/1/2018 through 3/27/2020.
Zip codes and counties with the most events are the areas of Pennsylvania with the most people (population centers, or cities including Pittsburgh, Philadelphia, and Harrisburg). Maps like this can be used to help people learn about community events near them or determine new parts of Pennsylvania where community events are needed or can be developed.

Learn more about participating in your community by visiting the ASERT Collaborative or Philadelphia Autism Project calendars of events. The ADA National Network also has a Planning Guide for Making Temporary Events Accessible to People with Disabilities.
Cherundolo | 7-13
Volume 8 ► Issue 2 ► 2019
Case Study of Independence: Daniel’s Journey
Susan Cherundolo
Abstract
This case study provides insight to the challenges and barriers to independence for participants who are dually diagnosed with Autism and mental health issues. This article will identify action steps that are replicable across community settings to increase independence for individual clinical needs and profiles. The following case study focuses on an individual named Daniel, who was living in a state hospital for individuals with psychiatric diagnoses. Today, Daniel is living in his own apartment with three housemates. He is active in his community and exploring friendships and intimate relationships, as well as the challenges that may present.
Being Misunderstood
Daniel has a long history of state hospital and residential placements beginning at the age of 15, when he was diagnosed with Depression, Bipolar Disorder, and Intermittent Explosive Disorder. He had various mental health services in place throughout his childhood starting at age 9. This included outpatient therapy and in-home behavioral health services. In-home services include therapy and therapeutic support to assist parents with learning how to manage difficult behaviors. As he got older, he received services through Assertive Community Treatment Program (ACT), partial hospitalization programs, and various stays in residential treatment facilities. ACT assisted him with medication management and learning various independent living skills. Daniel was given the opportunity to move into his own apartment at age 20 after a long stay in a residential facility. In a short time, he was evicted for setting small fires outside and damaging property resulting, unfortunately, in being admitted to a psychiatric inpatient setting. At this time, he reported feeling suicidal and depressed. Various mental health residential rehabilitation placements refused to support him due to his previous fire-setting behaviors, and his parents did not want him back in the home due to alleged sexually inappropriate behaviors toward his younger sister when he had lived at home. This downward spiral of lack of appropriate supports, misconceptions, and lack of understanding, led to an admission to a state hospital for psychiatric treatment when Daniel was just 20 years old.
During his stay at the state hospital, Daniel actively participated in various therapeutic and social groups. He learned how to complete chores such as laundry and cleaning his room. He had a job in the hospital, where he was able to earn money by completing clerical tasks. Daniel was excited about these opportunities as he knew he was taking steps toward his own independence. Generally, Daniel struggled with maintaining friendships and intimate relationships that he expressed as important to him. He identified as being bisexual and stated that his parents have never accepted this about him. Beyond consensual, casual sexual relations with peers at the hospital, there were not many positive peer relationships, although Daniel reported later that he was engaged to another man at the hospital. Other than his interest in romantic and intimate relationships, Daniel reportedly liked to keep to himself. He was unsure how to pursue platonic friendships, even when others tried to be friendly. Daniel often engaged with others on Facebook, but this seemed to be used more as a way of connecting with the broader LGBT culture (individuals who identify as Lesbian, Gay, Bisexual, and Transgender) than making friends.
While at the state hospital, Daniel was diagnosed with
autism by the psychiatrist. This new perspective and additional insight
provided by Daniel regarding the fire-setting behaviors prompted a different
approach to understanding him. Specifically, when asked, Daniel would say that
he would set fires because he not only liked the smell but being outside next
to a fire helped him feel calm and content. It helped him from feeling
over-stimulated. It was determined by
staff at the hospital that Daniel did not engage in this activity to be
destructive. To that end, additional evaluations were conducted by consultants.
Although there were some discrepant clinical impressions, there was
confirmation by the state hospital’s psychiatrist that since there was no
recent history of physical aggression, fire setting, or self-injurious
behavior, along with improvement in provocative language and threats to harm
self or others, Daniel was recommended for discharge to a placement in the
community with 24/7 supervision after living in the state hospital for a little
over four years.
Although Daniel was recommended for discharge, it was difficult to find a place for him due to his fire-setting reputation, despite evaluations that provided information for service planning for his transition into the community. Fortunately, the state hospital social worker assisted Daniel to apply for a Medicaid waiver and after navigating all the red tape, enrollment proceeded and a team was built starting with a supports coordination agency that was not just willing but experienced in supporting people with autism. A supports coordinator (SC) assists with linking individuals to needed services to address their diagnostic and independent living needs. In this case, a residential living situation was needed so Daniel could be discharged from the hospital. Daniel’s SC visited with him in the hospital and participated in further discharge planning to get an understanding of Daniel’s needs to be successful in the community. Although the SC found that there were providers who were either not receptive or who did not have a home available with 24-hour support, the SC was able to find a provider who was willing to support Daniel. Despite having a preference to live in a county closer to where his parents lived, Daniel and his family agreed to try out a new home that was in another county once the options were shared and discussed as a team. After visiting the available apartment, Daniel became excited about living in his own apartment, and he was anxious to meet his new housemates and explore the local community.
Growing Toward Independence
Although Daniel was recommended for discharge, it was difficult to find a place for him due to his fire-setting reputation, despite evaluations that provided information for service planning for his transition into the community. Fortunately, the state hospital social worker assisted Daniel to apply for a Medicaid waiver and after navigating all the red tape, enrollment proceeded and a team was built starting with a supports coordination agency that was not just willing but experienced in supporting people with autism. A supports coordinator (SC) assists with linking individuals to needed services to address their diagnostic and independent living needs. In this case, a residential living situation was needed so Daniel could be discharged from the hospital. Daniel’s SC visited with him in the hospital and participated in further discharge planning to get an understanding of Daniel’s needs to be successful in the community. Although the SC found that there were providers who were either not receptive or who did not have a home available with 24-hour support, the SC was able to find a provider who was willing to support Daniel. Despite having a preference to live in a county closer to where his parents lived, Daniel and his family agreed to try out a new home that was in another county once the options were shared and discussed as a team. After visiting the available apartment, Daniel became excited about living in his own apartment, and he was anxious to meet his new housemates and explore the local community.
After intake and assessments, Daniel and his team determined that community support and behavioral support services would be an effective complement to the residential 1:1 supervision as the community team learned more about Daniel’s strengths and needs. Community Support provides assistance with finding social activities in the community and supporting the individual during these activities. Behavior Support consists of assisting the individual with managing negative behaviors and practicing positive coping skills for difficulty situations. Fortunately, Daniel was also assigned a mental health Blended Case Manager, who was able to link Daniel to mental health services and provide more frequent support than the SC. Daniel quickly developed a positive relationship with his staff. Daniel has reported that he most enjoys getting out in the community and doing the things that he likes to do like attending Gay Pride events, attending dances, and going out shopping and to lunch with peers. He likes to tell jokes and make his peers and staff members laugh. Daniel was also interested in applying for jobs so he could earn his own money and exploring volunteering or working at a plant nursery or outdoor garden as he enjoys nature and being outside.
With the support of his team, Daniel learned how to manage
his own groceries and cook small meals for himself. He learned to keep his room
clean and perform laundry duties. Daniel takes his medication daily with the
assistance of staff. He has started to learn about the medications he is
prescribed and the intended results. He has recently started to learn how to
use Uber and the bus system in the area to assist him with transportation
needs. He has plans to visit a friend a few hours away and will need
transportation. He does not feel comfortable getting his driver’s license at
this time due to feeling overwhelmed about driving.
Challenges
Despite a generally positive transition, supporting Daniel has been a work in progress with this team. Daniel had to adjust to living with three other housemates in a two-bedroom apartment. His first housemate moved out due to his own personal behavioral issues, and there are often changes with who lives in the apartment depending on individual needs. Some of these housemates are at a higher level of care than Daniel, so he often does not feel a connection with them. He would rather find a community of LGBT friends he finds relatable. With the help of staff, he has been able to learn to communicate with housemates when he needs his own space instead of becoming angry and verbally “lashing out.” When Daniel gets frustrated, he finds it helpful to go for a walk with staff or go out in the community to a Wawa to keep himself calm. He did not have the ability to engage in these calming strategies while he was in the state hospital. He has come up with a list of coping skills and calming activities that he can use to manage his anxiety and/or frustration. He keeps this list on the wall next to the TV in the living room.
One of the areas of independent living that Daniel struggles with the most is budgeting and money management. He enjoys spending money and online shopping, where he will often splurge on unnecessary items that he will buy impulsively. This then leads to a lack of money for groceries and other spending money. When he was in the state hospital, his income was limited and all of his needs were provided for, so he did not have as much freedom to buy the things he wanted. Now that things are different, Daniel has to understand how managing money and controlling spending is an important part of learning to live independently. His team works with him daily on this goal and has created a worksheet for him so he can write down his needs and wants with the amount of money he has. This helps him see how much money he can spend. Daniel believes that he can live with a friend who may have his own place and that he will not have to pay rent. He does not want to think about potential utility bills, food costs, tuition for school, and transportation needs. He is very adamant that he can live on his own, yet shuts down when financial issues are brought up.
Another area that is a struggle for Daniel is navigating intimate relationships. Daniel wants to be in a romantic relationship and to get married. He seems to want this to happen very quickly, without taking the steps to get to know someone. Daniel meets people and explores relationships by connecting with others on Facebook and in the apartment complex where he lives. He dated a male who lives in another group home in the complex, although they have since decided to remain friends. He also interacts with peers during community outings. Daniel’s team supports his desire to find intimacy and encourages him to meet people and explore relationships slowly, so he can be successful. This is often a difficult concept for Daniel, and causes much anxiety for him, as he had a fiancé when he was at the state hospital, and he states that he wants to be able to meet his own sexual needs. Daniel talks about being undecided and conflicted between wanting a serious relationship and wanted to explore new ones. When Daniel was in the hospital, he often got caught up in romantic relationships with other men. He is now learning to understand the difference between sexual intimacy and emotional intimacy with partners. His behavioral specialist is open to discussing his sexuality and talks with him about how sex can be different from other types of intimacy.
Keys to Success
Daniel has been successful in many ways over the last two years. He secured a job at Burger King and successfully worked there for approximately six months with the assistance of a job coach. He decided to leave because he wanted to pursue his passion of obtaining a criminal justice degree. Daniel applied and was accepted at a local community college. This was a big victory for Daniel, as he never graduated high school. With the help of disability services at the college, he will be able to take remedial classes, and is planning to take classes in Criminal Justice. However, he has since decided to delay community college and focus on independent living skills and relationship building with his new boyfriend, Doug. Daniel is still learning to process concerns before making impulsive decisions. He feels that working a few days at an outdoor nursery may be more suited to him at this time than a fast food restaurant. He is working on having a more positive relationship with family members and being able to express his sexuality in positive ways. Daniel has agreed to start participating in more social groups and community activities. There continues to be team collaboration (team meetings, conference calls) to address any issues or concerns that arise.
Daniel has had many obstacles along his path to independence but has been able to continue to thrive with the assistance of his team, including his family. Daniel is fortunate enough to have a multi-disciplinary team with great diversity: providers with experience in supporting people with autism and individuals from the mental health system to provide support from that perspective. Daniel’s team consists of two Behavioral Specialists, various Residential and Community Support staff members, a job coach as needed, a mental health blended case manager, a house manager for his apartment, a psychiatrist and medical doctor, and a supports coordinator. His behavior specialists work with him on how to manage his anxiety, frustration, and anger. They understand when Daniel becomes upset and potentially verbally aggressive. They never hold this against him and always follow up with him to ensure he knows they continue to support him. Residential staff is available in the home, so Daniel is supervised at all times, but he is able to go for walks on his own and can be alone in his room. His community support staff help him participate in community and social activities and often joke with him when he is feeling down. Staff assist with transportation when Daniel wants to visit his parents. Daniel’s clinical coordinator through his residential placement remains in contact with his supports coordinator to ensure all hours in his Individual Support Plan are authorized as needed. His clinical coordinator is notified anytime Daniel has a concern or question and always has her “door open.” Daniel’s house manager assists with managing any apartment or housemate related issues. Daniel’s Blended Case Manager helps him locate resources as needed, such as a rep payee (someone to manage his SSI payments), Office of Vocational Rehabilitation (OVR) services, or applying for jobs or colleges. He also assists with any mental health resources as needed. Daniel sees his psychiatrist quarterly to discuss any medication-related concerns.
Daniel also has a special mentor named Lisa who was previously his house manager at his residence. She continues to be an important part of his team even though she has different administrative duties now. She is always there to lend a hand or an ear to Daniel when he calls or needs something. Lisa is very invested in Daniel’s care and wants him to be successful.
Overall, Daniel’s quality of life has improved greatly since being discharged from the state hospital in 2017. He has stated that he is grateful to be out of the hospital and living as independently, as possible. He enjoys going places with staff and learning how to do things on his own. He continues to learn new ways of navigating relationships and social opportunities. He is hopeful that he can live on his own someday, with the continued support of his team, as needed. Having this strong team has improved Daniel’s chances for success even when he, himself, is doubtful of that success.
Lupey, Moran, Leamer | 14-21
Volume 8 ► Issue 2 ► 2019
More Than a Village
Ian Lupey, Heather Moran, and David Leamer
Abstract
A case-study is presented of an individual who lives successfully within numerous community-based social networks, resides in own apartment, independently navigates transportation, works full-time, and enjoys a robust variety of individualized hobbies
and interests. Yet, six years ago, access to these community supports led to an increase in challenging behaviors and more limitations to community integration. An analysis is made to the successful aspects of treatment which is hypothesized
to include: person-centered programming, attention to underlying function of behavior, maximizing natural supports, and ongoing focus on objective measurement of progress.
Success never read the textbook. As professionals in our field, we continue to read and research the latest strategies built on pre-existing data. Those textbooks and peer-reviewed journals outline successful strategies through supporting data and reflect current approaches within the field. Although sometimes under-estimated within the field, the role of natural supports can often be the most integral part of one’s success. A strategy at home may be the only strategy necessary for an adult with Autism Spectrum Disorder (ASD) if implemented by the individual’s parents, but what about a boss at work or the waitress at a favorite diner? This article highlights how one individual’s path to success was influenced by a community of supporters, including individuals who were not part of the immediate treatment team. As numerous researchers have noticed, “One of the most provocative avenues is extending beyond individuals with disabilities and the services system, to understand and impacting larger community itself, this is an exciting frontier” (Novak et al, 2013).
Challenges within the Education System
Leo sought to be like any other person chasing the American dream: working to support himself, living on his own, maintaining a social life, and staying true to his own hobbies and interests. Leo had been diagnosed with Autism at an early age and his parents did not always know what supports were available. During his primary school years, Leo made progress academically, but behavioral challenges became more disruptive. Behaviors of concern included retracing his steps, spending excessive amounts of time washing his hands, over-eating, and other disruptive behaviors that drew attention from peers and the school staff. Even though it may or may not have been the original function of these behaviors, Leo received attention and it strengthened those “problem behaviors.”
After graduating high school, Leo enrolled in higher education. He attempted to complete a bachelor’s degree and found support along the way from various faculty and staff at the university he attended. While in two separate post-secondary educational settings, and with numerous natural and college-based supports, Leo found it impossible to maintain academic and social success. He was frequently distracted and disorganized, misunderstood socially by peer groups, and increasingly feeling a personal sense of anxiety and displeasure with remaining in that setting. His parents did notice; however, he was well liked by some of his peer group, had a very positive influence on many of those around him/roommates and had unwavering support and understanding from many faculty members. Following two unsuccessful attempts as a full-time student, Leo returned home and began employment in his local area in the restaurant and landscape industry.
Life after School
Running low on ideas and still hoping for a life outside of the nest, Leo’s parents helped him to find placement in a residential setting where he could receive support while gaining independence. As a result, Leo began living with several individuals who also presented with a variety of behavioral and other challenges. During this time, Leo began working at a local dining establishment. The team quickly learned this was not an appropriate placement due Leo’s overeating behavior with access to unhealthy foods. Leo was able to secure a position in a different department within the same organization. With these large steps towards independence, Leo and his parents sought out more services: integration, employment, and behavioral supports.
While living with individuals in the residential setting, a new behavior developed as a coping skill: elopement. With the behaviors of his roommates causing him anxiety, Leo developed this behavior to avoid them. Leo would often leave the home without telling anyone and staff was often unable to locate him. This became problematic and resulted in a team unable to provide services. Together, Leo’s team decided that living in this type of residential setting was detrimental to his goals and they began working to find different residential options. A Section 8 apartment with significant rent reduction became available and Leo was determined to give it a try. When Leo moved into his own apartment, the pressure was on for the treatment team.
Individualized Planning
In this new and independent setting, Leo’s team focused their approach on individualized planning, more specifically those supports Leo had naturally acquired: college faculty members, bosses at work, band members, etc. Given Leo’s ability to pair
with these individuals and prior learning history, his team gained insight into how to teach skills across settings. The community members that Leo learned from became “influencers,” both as a result of their leadership roles and personal interest
in Leo’s success. These important individuals were impacted positively by the opportunity to support Leo and play an integral role in his success.
The next step was identifying and addressing the functions of his behaviors. Leo’s team identified two functions that were maintaining the problem behaviors: sensory and attention. It became clear that the initiation of the behaviors was to satisfy a sensory need; however, as a natural consequence, Leo was also obtaining social attention. The team had to carefully select which strategies would be effective to increase appropriate behaviors without reinforcing the problem behaviors that were maintained by attention. Analysis to the function of behavior can be a bit more challenging when working with adults in the community yet remains an imperative step to determining the most effective strategies to implement. “Specifically, practitioners must continue to expand and develop effective functional assessment models to specifically address the unique needs of adult populations and service settings.” (Manente et al, 2010)
Identifying Effective Strategies
Finding effective strategies began with improving motivation. “A meaningful life requires reinforcement that is overarching, intrinsic, and positive.” (Villatte et al, 2016). Lucky for Leo’s team, the most effective reinforcer was always clear: social interaction. Many of Leo’s hobbies of playing instruments, singing, and bowling included a social aspect. Leo’s team, now having grown to include the influencers, used social interaction to not only motivate Leo but to reinforce him for success.
Beyond motivation, the team relied primarily on the prompting hierarchy. When learning a new skill, Leo’s team would use most-to-least prompting to ensure Leo was learning the skill without any errors. Most-to-least prompting would start with
a team member modeling or demonstrating the skill/behavior. Then, the team would use verbal prompts (“Do this first” or “What do you do next?”) and continue to fade to only gestural prompts (the team would point to a task to be done).
Once Leo demonstrated the skill independently, the team would move to least-to-most intrusive (e.g. starting with a gestural prompt and moving up to modeling). This style of prompting allowed Leo many opportunities for independent success.
Maximizing Natural Supports Through Community Integration
If a problem behavior was observed, reinforcement was withheld until the appropriate behavior was displayed; this is part of a more comprehensive instructional strategy known as differential reinforcement. In the case of repetitive/restrictive behaviors (i.e. retracing steps, washing hands, etc.), reinforcement was withheld until the behavior lessened. This style of reinforcement was very effective in strengthening the appropriate behaviors and decreasing the problem behaviors. Once the most effective strategies were identified, Leo’s team implemented them in all settings so the influencers could learn the strategies as intended.
With help from Leo’s team, each influencer learned how strategies were implemented and the rationale. The influencers were quickly reinforced by Leo’s appropriate response to the strategies. For example, when the choir director learned the prompting hierarchy, he did not have to stop a song to prompt Leo; he simply needed to give a gesture. When Leo’s boss learned to acknowledge only the appropriate or alternative behaviors, he noted that Leo was more aligned to the regulations in the work setting. Without exception, each community influencer was easy to approach and very willing to be flexible and make accommodations with relatively little effort. It was important to have Leo's support and participation with each individual and he was a key component to explaining how he needed added support. It is important to identify some relatively minor adaptations prior and go into the meeting with a specific request in mind and indicating that it might only be for limited time-duration.
The team taught Leo new skills including cooking and cleaning through social motivation while he lived independently in his new apartment. The team would remind Leo of the social significance of the skill. For example, to help motivate Leo to keep
his home clean his team would remind him if a girlfriend were to visit, she may not enjoy seeing his apartment with dirty dishes in the sink. Leo continued to engage in repetitive behaviors so his team would remind him it would be rude to keep
his friends waiting. At work, Leo learned new aspects of the job and was able to work with different people in different departments of the facility.
Once these skills were learned and he was fluent, Leo’s team facilitated the social interactions that were highly motivating. The team helped Leo invite peers to his place to watch a movie or play a game and would go as far as offering to drive individuals
to and from his place. Leo was then able to make the connection between having a clean apartment and his peers having a good time. When Leo demonstrated success regulating behaviors in the community, he was naturally reinforced by additional
time he could spend with his friends.
Leo now has a reinforcer day built into his schedule. These reinforcer days include Leo heading into the community to meet up with friends or making new ones at a local coffee shop, bowling alley, or band practice. While at these places and interacting with the community, Leo is able to practice skills with careful supervision from his team and those influencers. Practicing skills across the many settings with many different community members helps Leo strengthen those skills.
Measuring Success
Leo learned many new skills and is still living on his own to this day. However, many of the problem behaviors Leo demonstrated in high school are still present; so how can success be measured? From the beginning, the team, including those influencers, collected data to track Leo’s progress. The frequency data suggested that Leo is retracing fewer steps. The duration data showed staff that Leo was spending less time washing his hands. Leo’s team also took into account that some skills (appropriately portioning out meals) did not occur at a consistent rate, so the measurement had to reflect successes out of opportunities. Based on the results of all the data collected, the team is able to determine that the behaviors are becoming less socially significant.
Leo identifies success as living independently, supporting himself financially, and staying true to his hobbies. Leo has a village of family and support workers who help him every day, but it was outside that village, in those influencers, where
Leo found the most success. Those natural supports continue to be present in every aspect of Leo’s environment and strategies are implemented consistently in all settings. Achieving success will vary with each individual. Success was knocking
on Leo's door and he answered it. Leo's success was achieved through proper motivation and a team including his village and beyond.
References
- Novak, A.A., et al, Social Inclusion and Community Participation of Individuals with Intellectual/Developmental Disabilities. Journal of Intellectual and Developmental Disabilities 2013;51(5)360-375
- Manente, C.J., et al. Effective Behavioral Interventions for Adults on Autism Spectrum: Best Practices in Functional Assessment and Treatment Development. The Behavior Analyst Today, 2010;11(1) 36-43
- Villatte, J.L., et al. Acceptance and Commitment Therapy Modules: Differential Impact on Treatment Processes and Outcomes. Behaviour Research and Therapy. 2016; 77, 52-61
Neuville | 22-28
Volume 8 ► Issue 2 ► 2019
The Gift that Keeps on Giving: Social Role Valorization as a Framework for Designing Good Supports
Elizabeth P. Neuville
Abstract
Despite many years of operating community-based programs with the intention to assist people with disability to have full, rich meaningful lives, some of the biggest hoped-far gains, such as an end to degradation, isolation, and rejection, and a full
welcome to people with disability to share everyday lives with other citizens, have eluded us. This paper outlines the basics of Social Role Valorization as a well-seasoned framework and offers encouragement to adopt and adapt its principles to help
services better deliver on their promises to the people they serve. In summary, positive behavior support is an evolving practice that integrates person-centered values with behaviorally based scientific practices and other theoretical orientations
to address the comprehensive needs of individuals with developmental disabilities. At the heart of positive behavior support is the person we are seeking to support. Our allegiance is to that person, requiring us to be person-centered while drawing
from the most effective approaches science and our collective professional wisdom has to offer.
Background
In nearly five decades since Dr. Wolf Wolfensberger published The Principle of Normalization, a transformative idea set which sparked the community movement, at least for people with developmental disability, in North America, parts of Europe, and Australasia. At the time, the brutal conditions in the large-scale institutions, such as euphemistically named state schools, state centers, and state hospitals were revealed for all to see, thanks to intrepid change agents like Burton Blatt, Bill Baldini, and many others who captured and described the conditions. Images of the realities of the institution came into our living rooms and forced us to see “man’s inhumanity to man.”1 Although it was obvious that what was happening in those places of despair was, quite simply, wrong, it was hard to discern what should be for people. In other words, what would be right? Normalization provided the first clear guidance on this, and across the western world, it was seen as the spark that was needed to fuel the creation of a community system. The key idea, simple yet elegant, was that people who are marginalized and devalued should have life conditions that are at least as good as those of typical citizens. There was great hope that what would be created for people with disability – typical residences, valued work options, full integration, and full lives - would stand in sharp contrast to years of segregation, mistreatment and neglect.
However, as the community system was constructed across the United States, it became clear to those developing and using Normalization that deep social devaluation, oppression and segregation was continuing in more subtle and hard-to-see ways, even in more typical settings like group homes and supported living models. The institutions were improved, no doubt, and yet the essence of segregated institutions – places of purposeless life-wasting- held on, and the institutions, in their appearance, became much more palatable to everyday people. One might say that we put curtains on the institutions, and it became harder to recognize the nature of the beast. In many ways, the hoped-for changes towards a community system of support had eluded us. For these and other reasons, in the 1980s, Normalization was re-conceptualized into Social Role Valorization (SRV), a more deeply nuanced set of ideas which was built on top of Normalization, with many powerful components.2
A Refresher on Social Role Valorization
Social Role Valorization (SRV) is based on a framework of understanding how people come to be at the bottom of the social ladder, and what really works in people’s lives to lift them out of this social devaluation. The central strategy is to assist people who have had very negative societal roles – such as burden, eternal child, menace, sick, ‘better off dead’, human service client, object of ridicule to name a few – instead be assisted to move toward valued roles, like citizen, taxpayer, neighbor, big brother, student, employee, homeowner, amateur artist, club member. These valued roles carry great weight for all people, as they are the means through which all people gain access to really important things like acceptance, belonging, a good reputation, a strong self-image, opportunities, and a full, rich life.3 Services which support and assist people to have valued social roles as a focus point seem to be the ones which provide the greatest well-being to the people they serve.
Unfortunately, most services, in these enlightened days, seem to focus on activities in and of themselves, rather than crafting a vision of valued roles for each person they support, individually, then moving towards that vision by enabling activities which are directly related to the development of valued roles. SRV offers a fundamentally different understanding. Competency development is one way to build towards valued roles – for example, assisting someone to be in the role of fisherman or woman involves learning at least some of the skills needed to fish, but also involves helping someone to have the image of the role – by having the equipment, the license displayed, the right clothing, and many subtle and obvious cues, not to mention all of the people that a fisherman or woman would typically interact with. Much more remains to be said about valued roles, their benefits, and how to support people with disability to grow into them successfully, but a deeper study of SRV can be pursued elsewhere. In science, SRV would be said to be an elegant theory, meaning that it is a simple concept from which many, many corollaries and aspects can be drawn. Indeed, SRV is not a method, there is no checklist, no workbook, and no ‘package.’
An organization does not “do” SRV – but if used as a foundation, it seems that whatever methods an organization uses can be done better, deeper, more fully, and with more positive benefit if laid on a strong foundation of SRV, provided the method has
relevance and potency in and of itself, and does not cause harm to people.4 For example, it seems that the practices of positive approaches, or person-centered planning, or applied behavioral analysis, or any other number of practices
can be done with more depth, sensitivity, equity, responsibility, and success if the practitioner understands what SRV has to teach us. Understanding the important SRV frameworks such as the existential wound of segregation and rejection, the power
of the physical environment in shaping behavior, the importance of valued societal participation, allow practitioners deep insight into the most powerful determinants of how people come to experience belonging and acceptance. For instance, inclusive
education will be, quite simply, more inclusive and successful with an understanding of the power of imitation and modeling and role expectancies offered by SRV theory. Helping people have freely-given relationships, much talked about in our field,
actually has a fighting chance if SRV is understood and used.5 SRV often appears to help practitioners, families, advocates, and everyday citizens see more keenly the experiences that people with disability have borne, identify more closely
with such people, and work more fruitfully towards better futures.
A Gem of a Concept
One practical, powerful, and useful concept developed and described in SRV is the concept of the Culturally Valued Analogue (CVA), which is defined as a societal practice that is used with frequency, with which most people would be familiar, and most people would think well of.6,7 This simply means that, whenever a strategy is required to support a person, a first and foremost question should be asked, “What happens for typical people with a valued status?” If this question is asked and answered, the next question can be, “Can we start with that?”
A simple illustrative example is learning to ride a horse. When this seems like something someone served might be interested in, service workers often leap to offering therapeutic riding activities designed for groups of people with disability. They exist everywhere these days and are often free. However, SRV theory teaches to first ask the question about how horseback riding, or the role of horseback rider (to put it in role terms) happens for typical people. Well, there are many ways that typical people might do this, or enter this role – take riding lessons, find a friend who has a horse, take a guided trail ride, purchase a horse, lease a horse, join a program at a local riding stable- you will notice that none of these include getting horseback riding therapy. Yes, a person might need support and adaptations to ride a horse, and these can be provided while not straying too far from the natural pathways. And yet, it is much easier to pursue segregated, medicalized horseback riding, despite the fact that it relegates horseback riding, an enjoyable sport that is done for its own sake, as a means to fix or treat people. In fact, that is a good way to think about the CVA – it is exploring the natural pathways that already exist in society.
Program vs Home
For those who design and operate residential services, the CVA offers exceptional guidance in creating environments that are truly home. And that is a helpful thing to remember – the CVA for a residential program is, in fact, home. Home is an incredibly
powerful driver of the quality and richness of life for most valued citizens, and that, in fact, many people exert a great deal of effort in creating for themselves. For many people with a disability, the loss of home has been one of innumerable losses,
particularly for people who have been institutionalized, or who have been in the revolving door of mental health programs, where people cycle in and out of many different residential services, single-room occupancies, living on the streets, prison,
and hospitals.
If planners and workers simply spend time discussing and laying out the qualities and characteristics of a valued home, one that most people would aspire to, yearn for and pursue, that is an excellent and worthy way to put the CVA to use as the basic
foundation of what the service is providing. Adaptations can be made from there. These adaptations need to be made to account for individual needs, and this is a part of making the service relevant and tailored to each person who lives in the home.
However, violations of the CVA should be monitored carefully, as service quality degradation can easily happen when the CVA is not guarded.
For example, practices which are put in place to protect the well-being of a person, such as locked areas, alarms, video monitoring, may be extended for years well past their purported need. Or the home may become full of indicators that this is a program,
such as the open presence of files, instructive signs, medical devices, notebooks, staff offices, workplace notifications, and many more. It is always an excellent idea to walk through residential homes from outside to inside looking for any and all
indicators that, in fact, this is a human service program rather than a home. Then, one can try to minimize these features. My colleague Darcy Elks has referred to these ‘service land’ feature as the “fingerprints of the organization,” and they are
best avoided. Use of the CVA calls into question many current practices popular in many human services, which clearly violate cultural norms, and should cause us to take up “studying the ordinary,” as my colleague Tom Doody says, as a good way
to rethink some of these practices.
SRV remains, after over 40 years of experience in use here and there across the world, a powerful way to understand the experience of living with a devalued status within society and offers a rich collection of strategies which make good sense to help
uplift people towards better lives. It is helpful in designing and structuring human services, as well as individually supporting people to live lives embedded in the best of community. Although Social Role Valorization concepts are not always easy
to implement, it seems there are no shortcuts to building community around people and using what we know about how society behaves to benefit those who may need it most. Social Role Valorization, over the years, continues to provide such valuable
guidance to those trying to do best by the people they serve, and truly functions as a gift that keeps giving.
References
-
Burns, Robert. The poetical works of Robert Burns. JB Lippincott & Company, 1868.
-
Wolfensberger,W. Social role valorization: A proposed new term for the principle of normalization. Intellectual and developmental disabilities. 2011; 49.6: 435-440.
-
Osburn, J. An overview of social role valorization theory. The SRV Journal. 2006 1.1: 4-13.
-
O'Brien, J. Celebrating the genius of Wolf Wolfensberger. Research and Practice for Persons with Severe Disabilities.2011; 36.1-2: 76-79.
-
Lemay, R. Social role valorization insights into the social integration conundrum. Mental Retardation. 2006; 44.1: 1-12.
-
Wolfensberger, W. & Thomas, S. PASSING: A tool for analyzing service quality according to Social Role Valorization criteria. Ratings manual. (3rd rev.ed.). Syracuse, NY: Syracuse University Training Institute for Human Service Planning, Leadership & Change Agentry.
-
Barken, Emma. "Almost, but not quite there: Failing to fully develop culturally valued analogues." The SRV Journal. 2010; 5.1: 14-20.
Salzer | 29-35
Volume 8 ► Issue 2 ► 2019
Community Inclusion as a Human Right and Medical Necessity
Mark Salzer
Abstract
For individuals with behavioral, intellectual, and developmental disabilities, community inclusion refers to the extent to which individuals who experience disabilities have the opportunity to fully participate in their community and welcomed, embraced, and valued for the unique contributions they can make to society. Community inclusion is recognized as a human right and a medical necessity in terms of the extent to which it can leads to enhancements in physical, cognitive, and mental health and wellness. This article makes the case for the importance of community inclusion and introduces the key conceptual, theoretical, and evidence-based fundamentals for promoting it.
This article was supported by a grant from the National Institute on Disability, Independent Living and Rehabilitation Research (NIDILRR) (90RTCP0001-01-00; Dr. Salzer, principal investigator). The contents of this article do not necessarily represent
the policy of the U.S. Department of Health and Human Services, Administration on Community Living, or NIDILRR, and endorsement by the federal government should not be assumed.
___
Community inclusion2 refers to the extent to which individuals have the opportunity to fully participate in their community like everyone else and be welcomed, embraced, and valued for their uniqueness and abilities1. Community
inclusion has been a longstanding concept for policies and service delivery in the broader disability community for more than six decades, starting with the Danish “Normalization Movement” that promoted the notion that individuals with intellectual
disabilities should be supported to the extent that they are able “to function in ways considered to be within the acceptable norms of his/her society”2. Nirje discussed normalization in terms of ensuring that people with disabilities
experience “…patterns of life and conditions of everyday living which are as close as possible to the regular circumstances and ways of life of society”3. Expanding on these ideas, Wolfensberger’s2,4 Social Role Valorization
Theory argues that promoting participation in valued social roles, such as work, school, religion, etc., reduces the risk that persons with disabilities are devalued by society.
The Americans with Disabilities Act5 was born out of these lines of thinking and established the promotion of “opportunity” for people with disabilities to live in the community in the law. International consensus on this issue was advanced
by the United Nations General Assembly that adopted the ‘Convention on the Rights of Persons with Disabilities’6, which argues that inclusion of those with disabilities is a human rights issue, and nations must “Promote full and effective
participation and inclusion in society, including…competitive employment, and participation in the economic, political, social, cultural, recreational activities of their communities.”
Community inclusion is more than a human rights issue, however. Greater inclusion leads to greater community participation, including work, education, religious and spiritual participation, engagement with family and friends, leisure and recreation, and other domains associated with a meaningful life. All of these are associated with physical, cognitive, and mental health and wellness benefits for anyone, including individuals with disabilities. It is in this sense that community inclusion, and the resulting participation, should be viewed as a medical necessity. This is consistent with the International Classification of Health, Functioning, and Disease (ICF), developed by the World Health Organization7. According to this framework, health is viewed as more than problems with “Body function and structure” (e.g., impairments or symptoms). It also includes “Activities,” the execution of specific tasks or actions, and of most relevance here, “participation,” which is defined as involvement in a life situation such as domestic life, interpersonal life, education and employment, and community, civic, and social life (e.g., religion, politics, recreation, leisure, sports, arts and culture, dating). The ICF recognizes community participation as one domain of health by itself, and something that has a positive benefit on body function and structure. Benefits associated with community participation on health, cognition, and mental health apply to everyone. Participation, for example, addresses social determinants of health8, such as poverty, social support, and educational attainment, reduces sedentary behavior, especially long, sustained periods of sitting or lying down, that have numerous negative health consequences9 and also enhances cognition. Engagement in meaningful activities is also associated with greater levels of happiness 10.
In the past, there have been doubts about the capacities of people with behavioral, intellectual, and developmental disabilities, including autism, to participate, especially for those with significant impairments, or whether participation would be
healthy. The movement away from institutional care, for example, has provided clear examples to the contrary, although doubts may remain about the extent to which participation can occur even for those in residential programs. The case for community
inclusion and participation as a medical necessity for people with mental health and other disabilities has been articulated in “Well Together,”1 where research is offered to indicate that participation is just as beneficial to the
health of people with disabilities as it is for the general population. While participation may look different for different people (e.g., different number of hours, modifications in what participation looks like, unique supports), it is clear
that inclusion and participation are accessible to all.
Fundamentals for Promoting Community Inclusion
Salzer and Baron1 describe eleven fundamentals for promoting community inclusion, supported by key conceptual, theoretical, and research evidence. While the fundamentals presented focus on people with significant behavioral disabilities, they are derived from efforts across all disabilities. They are briefly described here.
Fundamental #1 - Community participation is beneficial. Increasing efforts to promote community inclusion require an appreciation that the resulting participation has significant physical, cognitive, and mental health benefits for people with
disabilities.
Fundamental #2 - Community inclusion applies to everyone who experiences a disability. Beliefs that providers/supporters/caregivers are able to predict who is, and who is not, ready to participate, are not well supported by the research. Such
beliefs may be used to inadvertently restrict opportunities for full and meaningful participation among those who could otherwise participate to some degree and in ways that are specific to their interests and abilities.
Fundamental #3 - Community inclusion requires seeing ‘the person’, not ‘the patient’. Individuals with disabilities must be viewed as people who have hopes, dreams, desires and capabilities like everyone else that should be supported, rather
than solely as “patients” with an emphasis on deficits and impairments.
Fundamental #4 - Self-determination and dignity of risk are central to community inclusion. Self-determination refers to ‘acting as the primary causal agent in one’s life and making choices and decisions regarding one’s quality of life free
from undue external influence or interference’11. Dignity of risk is the “right to make choices that affect one’s own life even when these choices could, or do, turn out to be mistakes, allowing individuals to learn from their mistakes
along the way like everyone else”12. The decision about what areas one wants to participate in, and to what degree, is a decision best left up to the person, short of the rare circumstances when such participation might truly be dangerous
to them or others. Concerns about potential failure in participation should be weighed against the benefits of pursuing one’s own goals and learning from mistakes.
Fundamental #5 - Community inclusion embraces multiple domains of mainstream life. Housing and employment are important areas, but not the only meaningful areas in people’s lives. Efforts should be made to support participation in multiple domains
of community life.
Fundamental #6 - Community inclusion focuses on participation that occurs more like everyone else. While all participation has value, participation can be more or less like everyone else depending on where it falls on three dimensions. First, to
what extent is the participation occurring within programs or agencies (e.g., employment in sheltered workshops, movies onsite) or in the community (e.g., a competitive job, a move theater). Second, to what extent is the participation chosen by providers
(e.g., a staffperson comes up with the event, like going to an amusement park or picnic) or by the individual (e.g., person expresses desire to engage in an activity). Third, to what extent does the participation result in segregation (e.g., large
group of program participants going somewhere together or participating in an activity only with one another) or offer opportunities to interact with a wide variety of people (e.g., participation in the community with smaller groups or a natural supporter).
Fundamental #7 - Community inclusion is strengthened through emerging support technologies, the natural supports of families and friends, and the engagement of peer supports. A number of evidence-based modalities and practices currently exist that
can be used to promote a broad-range of community participation. These include practices that have emerged to support housing, employment, education, and other participation domains. Natural supports, such as family, friends, neighbors, etc., are
critically important and result in participation that is more like everyone else. Peer support is a well-established modality in the broader disability community, as seen most clearly in the independent living movement, and is becoming more established
in the behavioral, intellectual, and developmental disability communities.
Fundamental #8 - Providing support to family and other natural supports promotes community inclusion. Caregivers of individuals with disabilities participate less in the community and experience significant strain and distress. They are a critical
resource in the promotion of inclusion and participation and require support themselves to maximize their ability to support their loved one.
Fundamental #9 - Environmental barriers to community inclusion must be identified and addressed. The social model of disability13 understands disability, or lack of participation, as resulting from a poor person-environment fit, where
the uniqueness of the person are not accommodated by the environment. This results in disablement. Historic examples of barriers that have been addressed for individuals with physical and sensory disabilities include curb cuts, ramps, and braille
signage. Barriers may also include prejudice and discrimination, access to transportation and resources, and poverty, all of which need to be addressed.
Fundamental #10 - Community inclusion initiatives for individuals with disabilities maximize the use of mainstream community resources. Exclusive dependence on disability-specific resources for participation unnecessarily restricts access to the
plethora of community-based resources and activities, such as employment, education, leisure, etc. that are available to all citizens.
Fundamental #11 - Community inclusion requires establishing welcoming communities. Full inclusion requires communities that actively welcome and embrace people with uniquenesses. This requires appreciation and desire for diversity as a strength
rather than something to be feared.
Conclusion
Community inclusion and participation of individuals with disabilities is a rights issue as well as a health issue. The application of these fundamentals requires a substantial paradigm shift, and shift in practice, for some. This will be both challenging and uplifting as new examples of participation are achieved by those where it was not believed possible. While participation outcomes may differ across the range of capabilities among persons who experience behavioral, intellectual, and developmental disabilities, including autism, the focus of policymakers, providers, caregivers, and all other stakeholders should be to work to promote inclusion and participation to the maximum extent possible.
References
- Salzer MS, & Baron, R.C. Well Together – A blueprint for community inclusion: fundamental concepts, theoretical frameworks and evidence. Melbourne, Australia 2016.
-
Wolfensberger W. The principle of normalization and its implications to psychiatric services. American Journal of Psychiatry. 1970;127:291-297.
-
Nirje B. The normalization principle. In: Flynn R.J. NKE, ed. Normalization, social integration, and community services. Baltimore: University Park Press; 1980:31-50.
- Wolfensberger W. The principle of normalization in human services. Toronto: National Institute on Mental Retardation; 1972.
- Americans With Disabilities Act of 1990, Public Law No. 101-336; 42 USC 12211
- United Nations. The convention on the rights of persons with disabilities. 2006.
- World Health Organization. International Classification of Functioning, Disability and Health. Geneva 2001.
- Marmot M, Allen J, Bell R, Bloomer E, Goldblatt P. WHO European review of social determinants of health and the health divide. The Lancet. 2012;380(9846):1011-1029.
- Thorp A, Owen, N., Neuhaus, M., Dunstan, D. Sedentary Behaviors and Subsequent Health Outcomes in Adults. American Journal of Preventive Medicine. 2011;41(2).
- Dolan P, Peasgood T, White M. Do we really know what makes us happy? A review of the economic literature on the factors associated with subjective well-being. Journal of Economic Psychology. 2008;29:94-122.
- Wehmeyer ML. Self-determination as an educational outcome: Why is it important to children, youth and adults with disabilities? In: Wehmeyer DJSML, ed. Self-determination across the life span: Independence and choice for people with disabilities. Baltimore: Paul H. Brookes; 1996:15-34.
- Perske R. The dignity of risk. In: Wolfensberger W, ed. Normalization: The principle of normalization in human services Toronto: National Institute on Mental Retardation; 1972:194-200.
- Oliver M. The politics of disablement. London, UK: Basingstroke Macmillians; 1990.