Positive Approaches Journal, Volume 9, Issue 2
| Site: | My ODP |
| Course: | My ODP |
| Book: | Positive Approaches Journal, Volume 9, Issue 2 |
| Printed by: | |
| Date: | Monday, July 27, 2026, 8:06 PM |
Positive Approaches Journal | 5-6

Volume 9 ► Issue 2 ► 2020
Introduction
Communication can be defined as the successful exchange of a message between two or more people. But isn’t communication so much more than this shared message? It’s how we develop relationships and build trust, and how we advocate for ourselves; it’s our connection to others. Communication is a huge part of our everyday life. Although communicating may sound like a simple concept, communication, especially effective communication, is quite complex. It entails many aspects of a multifaceted process that is embedded in everything we do as individuals and is part of a social structure. To complicate it even more, each person communicates differently. Yet we know everyone communicates and despite how they communicate, they want and need their message to be received.
For instance, as an individual with Autism Spectrum Disorder (ASD), I tend to think of things quite literally. When my roommate asked if there were dishes in the sink, I looked and saw a spoon and a pot. To me, at that moment, that did not register as ‘dishes’ – it registered as a spoon and a pot. I think and process information literally. My roommate, who is not on the spectrum, thought she was being clear when she asked her question. However, when she came down the next day and saw the spoon and pot in the sink, she was not happy. Despite both of us having strong verbal communication skills, there was still a breakdown in communication.
Everyone communicates and has something to say, in one way or another, it is just a matter of how we learn to ‘listen’ to one another. At a foundational level, four aspects are needed for communication: a way to communicate, a reason to communicate, a topic to communicate about, and a communication partner to share the message through a common modality (Willis, 2020). In this issue, authors will touch on some of the many aspects of communication and provide some guidance on how to be both a better sender and receiver of communication.
— ODP’s Special Populations Unit and Hope Pesner
Positive Approaches Journal | 7-13
Data Discoveries
The goal of Data Discoveries is to present useful data using new methods and platforms that can be customized. For optimal viewing and engagement, use the full screen function at the bottom of this section.
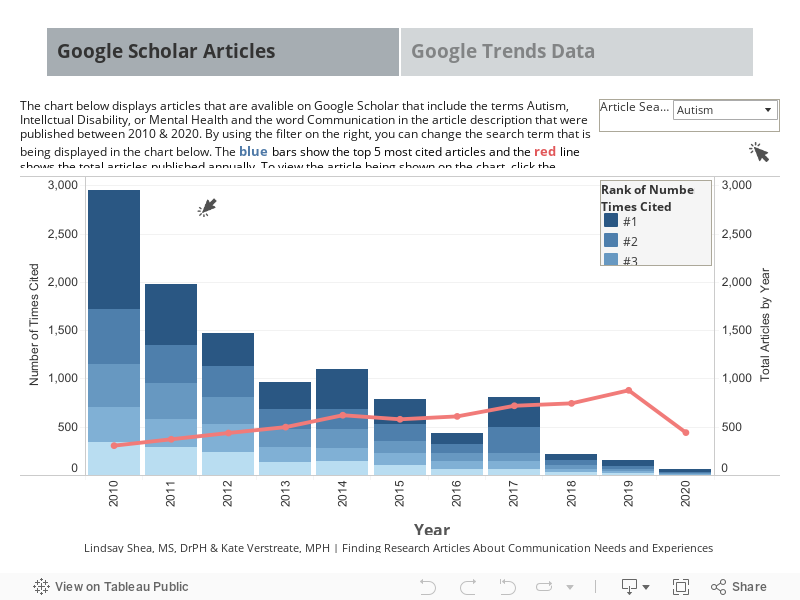
Finding Research Articles About Communication Needs and Experiences.
Data is an important tool used in research studies, generally. Specific to this journal issue, data can be useful to understand communication issues and identify new solutions and supports for communication. Research studies are usually published in peer-reviewed journals that may require a fee to view the full text of research articles. New tools, like Google Scholar, link to full text versions of research articles that are free and let you easily search options to find articles that are interesting or useful and accessible to you. One important way to determine how valuable a research article has been to increasing the understanding of communication needs and experiences is how often it has been cited. Research articles are cited, or used as references, when they contribute new information that has not been described previously or use innovative methods to understand an issue like communication. This issue's Data Discoveries is a Tableau dashboard displaying research articles about communication that have been cited frequently and links to Google Trends to see news and other new information about communication from across Google searches.
Research articles that you access through Google Scholar usually have corresponding author. You can email a corresponding author, or any author on a research article, if you have questions about the research. It also might be helpful to Bookmark Google Scholar or Google Trends in your Internet browser so you can use them easily in the future. The ASERT Collaborative has several resources about communication, including a description of the spectrum of communication, information about how communication works both ways, and a guide to wearing a mask and navigating communication during COVID-19. The US Department of Labor Office of Disability Employment Policy also has resources about communicating with and about people with disabilities.
Black | 9-17
Volume 9 ► Issue 2 ► 2020
Meet Alex Black: A Supported Life Well Lived
Molly Black
This article was revised from an original post at: https://nfadb.org/page-18334/
My son, Alex, was born in 1991. He loved music, swimming, hanging out with his family—especially his sisters—reading books, and looking at photos. He also enjoyed spending time alone in his man cave.
Alex was an individual with complex support and healthcare needs due to the etiology of Cornelia de Lange Syndrome. Cornelia de Lange syndrome is a genetic disorder. People with this syndrome experience a range of physical, cognitive, and medical challenges ranging from mild to severe. The syndrome has a widely varied phenotype, meaning people with the syndrome have varied features and challenges (www.cdlsusa.org1). Alex required one-on-one support to complete tasks associated with work, recreation, hygiene, socialization, and safety. Meeting his needs and interests, and our family vision for his adult life, required a great deal of planning. Support as a young adult also required funding. We were fortunate that he had partial Medicaid waiver funding throughout his high school years and full funding through developmental disabilities systems at age 21, in addition to Supplemental Security Income (SSI).
Once Alex exited the school system, his entitlement to services and supports went away. This is the case for many students with disabilities because adult services are based on eligibility and availability of services. Pennsylvania, where we live, has a long waiting list for adult services. They are not easily obtained without advocacy and emergency level of need for individuals with intellectual and developmental disabilities. To be completely honest and frank—without funding, his transition would not have been as successful as it was and would not have met all his needs and interests.
Natural supports for complex individuals are not always easy to find or have available at all times, even though we may desire and plan to use them. Often, those with high healthcare needs and lower communication skills only have paid support, especially as family and friends age. An individual with deaf-blindness and additional needs might require funding for transportation, interpreter services, or home and community habilitation support to complete daily activities, including but not limited to work, medical appointments, and social needs. Throughout Alex’s childhood and adolescence, we often asked ourselves, “If he didn’t have a disability, where would he be learning, playing, socializing, and possibly working?” We used that to guide our decisions for, and with him. Throughout his high school years, we used many person-centered tools such as person-centered planning, Planning Alternative Tomorrows with Hope (PATH), and several vocational assessments, including the process of Discovery. Discovery is a person- centered planning process that involves getting to know a person before supporting them in developing a plan for employment. 2 Discovery allowed us to see his strengths and abilities and envision ways he could contribute to his community through work. As parents, we think we know so much about our children, but we learned many new things about Alex through this process.
Planning took A LOT of effort on our part and a great commitment from our school district. Alex’s school funded vocational assessments and the process of Discovery leading to the development of a vocational profile. We formed a team around Alex and allowed him and his interests to be the focus. We created an individualized program for him, and it happened in the community.
Adult agencies were also included in planning for Alex’s future, including Developmental Disabilities, Vocational Rehabilitation, and the Bureau of Blindness and Visual Services. Unfortunately, this was before WIOA—the Workforce Innovation and Opportunity Act. Vocational Rehabilitation did not deem Alex able to benefit from their services and closed his case.
It was important to have a plan in place long before high school ended. Early planning was the key. In Pennsylvania, transition planning begins at age 14. Alex’s planning included exploring vocational pursuits at school and in the community, developing volunteer opportunities, expanding recreational activities, and making community connections. The goal was to have a plan for what his day would look like after he exited high school. Waiting to plan until age 19, 20, or 21 is far too late.
Alex was included in general education classes and his curriculum included a focus on life and vocational skills to prepare him for post-school success. An extra year of high school, after he walked at commencement, involved spending half of each day at school and half in the community securing vocational opportunities. It was important to us that these be individualized for Alex, rather than part of group experiences.
At school, Alex had a paraprofessional in the role of the intervener. She also became an employee of the agency that administered his waiver and we were able to use habilitation aid funding to cover community support even though it was during school hours. I would be remiss if I did not give this individual the credit she was due. She transitioned with Alex and became a hybrid of habilitation aide, intervener, support service provider, interpreter, facilitator, and transporter; depending on what was required at any given moment. Most of all she was trained, and she respected our family values.
Alex communicated with signs, gestures, and Augmentative and Alternative Communication (AAC), but was non-verbal. His vision and hearing loss affected his ability to function. He was fortunate to have mobility, but his stamina and attention were short
lived. He had the ability to use his small hands, but his fine motor skills were limited. While his unique and creative life accomplishments may seem elusive for someone with his limitations, they were doable with planning and supports. He had interactive
days full of interesting things to do and a reason to leave his house and his family each day.
Alex had numerous vocational experiences that helped him learn valuable skills and have rich, meaningful interactions in the community.
- He folded towels (with help) in his consumer science class, not because he liked folding towels, but because it was a good life skill and other students were doing it too. We took that to his local YMCA in the community, where he had support folding towels as a work experience. After finishing his tasks, and with his own membership, he would swim and use the hot tub. One day, our family went to a local restaurant where the host greeted and interacted with Alex. He told us he had shared time in the hot tub with Alex at the YMCA. Unknown to us, Alex had made a friend outside of our family and school social circle through this experience.
- His vocational experiences were mostly volunteer, with the hope of working toward paid employment. Would that have ever happened? We will never know, but I’d like to think it could have. For example, when Alex was in high school, he used a rolling cart to deliver supplies and other items to teachers and the front office. We generalized this activity to a local nursing home where; with one-on-one support; he delivered magazines and mail on a similar rolling cart and collected trash from the residents’ rooms. He was truly included in the nursing home’s volunteer program and invited to their appreciation luncheons. They depended on him to show up and complete his work. We were informed that if he was able to work more hours, he could become a paid employee.
- He was a business owner. He received his first vending machine as a donation, and we invested in a second one. He shopped for products, stocked the machine with hand-under-hand support from his intervener, and did the banking. He enjoyed operating the coin-counting machine. This created opportunities to communicate with people at our church where the vending machine was located, as well as the bank personnel who looked forward to seeing him. We were proud of his ability to donate the money he earned to his church, just like other members of the parish.
- He baked dog treats for a local groomer, which included shopping for ingredients, baking, and packaging them. The owner provided natural supports to accommodate the work environment to meet Alex’s physical needs. Interactions with the owner, customers, and dogs provided a great benefit to Alex.
- He picked up shredded paper from a workshop and delivered it to a local farmer for animal bedding. The farmer appreciated these deliveries and took Alex for rides around the farm on his four-wheeler to visit the animals.
- He volunteered at the local public library, straightening bookshelves and pushing chairs back under tables. He got to know people in the community and to look at books, which was one of his favorite pastimes.
Alex lived a rich, meaningful life for 22 years. He was a contributing member of his church and his community, a business owner, and a cherished family member. At the time of his death, he was about to embark on the next step of his adult journey, moving out of his family home to live with a roommate. There is perpetual sadness around our loss, but gratitude for the love, joy, and unique experiences Alex brought to our family.
It is a complicated life our children and young adults with deaf-blindness lead. The world is changing, as many individuals, parents, and advocates no longer consider day programs, sheltered workshops, or remaining at home as the only post-school options. Just
like the push to include students with disabilities with their non-disabled peers in general education classrooms, we are seeing the same push to the community for adults.
My advice to other parents is to start planning early. Be an active part of your child’s Individualized Education Program (IEP) team. Connect with all potential funding and service providers as early as you can. Set high expectations for your child’s
life and don’t be dissuaded by others who do not share your expectations.
References
- Cornelia de Lange Syndrome Foundation, Inc. www.cdlsusa.org. Accessed July 2020.
- Condon E, Callahan M. Individualized career planning for students with significant support needs utilizing the discovery and vocational profile process, cross-agency collaborative funding and social security work incentives. Journal of Vocational Rehabilitation. 2008; 28: 85–96.
Biography Molly
Black is the parent of three adult children, one of whom lived for 22 years
with deaf-blindness due to the etiology of Cornelia de Lange Syndrome. She
currently serves on the Board of Directors of the Pennsylvania Partnership for
the Deafblind (PPDB), a non-profit, family support group. She is a past Board
Secretary of The Parent Education Advocacy and Leadership Center (PEAL), the
Commonwealth’s Parent Training and Information Center. She has coordinated and
facilitated several study groups of parents and professionals around topics
concerning Deaf-Blindness. Molly has led and participated in leadership,
advocacy, family engagement and transition training activities of the Project.
She continues to be passionate and motivated to support families who live the
daily struggle and joys of raising a child with Deaf-Blindness. She is
assisting to spearhead a national effort to support families adjusting to the
loss of a child. Molly resides with her husband in Irwin, a suburb of
Pittsburgh, PA and has been a Family Engagement Consultant with the
Pennsylvania Deaf-Blind Project since 1998.
Contact
Molly Black
Pennsylvania Deaf-Blind Project
7322 Sierra Drive, Irwin, PA 15642
412-719-9370
Gentile | 18-26
Volume 9 ► Issue 2 ► 2020
Behavior Change in Individuals with Intellectual/Developmental Disability
Julie P. Gentile, M.D.
Introduction
Individuals with intellectual disabilities (IDD) often have limited expressive language skills and may communicate critical information to those around them through their behavior. Intellectual disability is characterized by limitations in both intellectual function and adaptive behavior, which may include practical and social skills. A comprehensive assessment should be performed to determine the etiology of the disability and the appropriate services to support the individual.1 As Sigmund Freud stated, “All behavior is purposeful.” It is the job of clinicians, caregivers and family members to determine the etiology of behavior. A change in behavior may indicate a medical condition, a psychiatric illness, medication intolerance, or a host of other issues. It is the critical detective work that we perform that will reveal the etiology of behavior change. Behavior is not a problem; it is a form of communication. Literature shows that behavior change in ID often indicates medical or mental health conditions; it is vital that we facilitate timely identification of accurate diagnoses and treatment for same.2 Despite advances in preventive and medical care, age at death remains lower and mortality rates higher for persons with ID.1 Older adults with IDD carry a higher mortality risk relative to the general population, mainly attributable to respiratory, central nervous, and circulatory systems.
Assessment: The Biopsychosocial-Developmental Model
The biopsychosocial model is useful when attempting to determine the etiology of behavior change in a person with IDD.1 It is important to gather information from the individual, family, caregivers, clinical records, and collaborating agencies. The assessment can evolve over time and incorporates supporting, predisposing, perpetuating, and protective factors related to the disorder. In the assessment of behavior change in an individual with IDD, it is important to provide an environment most likely to de-escalate the situation. Use a calm, soothing tone, express concern, offer food or drink, allow trusted persons to be present when able, remove potentially dangerous objects and distract with positive activities. Avoid overcrowding individuals or exposing them to loud noises, addressing only the caregiver, concealing hands in pockets, using intimidating direct eye contact or a confrontational stance, and unnecessarily invading personal space. It is important to talk both directly to the individual and to obtain collateral information from others present.3 Care in the approach to the situation can help the provider obtain accurate and complete information for the assessment.
Biological Component
The biological aspects of the assessment will include information such as demographics, medical history, genetics, family history, medication trials, and substance use.4 Especially important is a medication timeline and a medication history that includes medications the individual was taking at a time when he or she was doing well. Ask questions about when the individual was most recently doing well and collect as many details of that point of reference. We must know what the highest level of functioning is and how to achieve that in the present. The timeline of medication trials is important, as individuals with IDD are more susceptible to medication side effects. It is also important to remember that externalized behavior may be a way for an individual to communicate about a current medical illness, so documentation by caretaking staff can be helpful to determine an underlying biological cause of the aggressive behavior.5
Psychological Component
Family history of violence, whether potentially genetically influenced or a learned behavior, is a predisposing factor, as individuals who experience violence regularly at a young age are more likely to be aggressive. Psychological data obtained should also include trauma history, information regarding developmental years, losses and significant transitions, environmental changes, past counseling relationships, and an individual’s coping skills.
Social Component
Social outlets are important for persons with IDD, and it is imperative they feel safe in their environments. Data should be gathered about residential placements, social activities, hobbies and interests, spirituality, spending money, exercise and activity, and feelings of safety.
Developmental Component
Individuals with IDD will usually present within the context of the developmental stage in which they live.1,6 IDD is categorized as profound/severe, moderate, or mild, which is often an indicator of the level of dependency needs and expressive language capability of the individual. Generally, individuals with mild cognitive deficits live in the community in supported residential situations and participate in life-long supported employment or programming. Persons in the moderate category will most often need varying levels of support from their families or community agencies. Because their expressive language skills are typically more limited, they are at higher risk for inability to communicate subjective complaints using speech about mental health and medical illnesses.1 Individuals with severe/profound IDD are more likely to have very high levels of dependence on external supports and to have associated medical conditions, with most individuals requiring assistance for all aspects of life. Significant medical complications, such as seizure disorders, swallowing difficulties, speech impairments, and reduced life expectancies are more common for persons in the profound impairment category.
Obtaining the history
- Always start evaluation with the individual—even if it is as simple as having them express how they feel in the moment. The evaluation should start and end with the individual
- Be mindful of the communication barriers faced by individuals with IDD and that responses may take longer to formulate than individuals who are neurotypical. Patience is key
- Use simple vocabulary and avoid complex sentence structures
- Start with very concrete concepts like food or other basic needs and workshop/daytime habilitation activities and build from there
- Sequencing chronological events is often a struggle for the individual but asking for caregivers to help frame reported events can be helpful
- Limitations of attention, physical impairments including bowel/bladder incontinence to even pain may limit an extensive interview
- “Problem behaviors” may in fact be a medical condition that needs to be addressed such as high blood sugar leading to frequent urination, which can be interpreted as the individual “attention-seeking” as opposed to a physical need5,6
Conclusion
Individuals with IDD are at a significantly higher risk of having comorbid medical, genetic, and psychiatric conditions that in turn place them at greater risk for medical conditions involving every organ system. Individuals with IDD are less likely to be afforded access to traditional preventative guidelines and treatment methods. The barriers to treatment must be overcome. It is well documented that neurotypical individuals with severe and chronic psychiatric illnesses have greatly reduced life expectancy. Since many individuals with communication deficits exhibit behavioral changes or acute psychiatric symptoms when experiencing medical conditions, the mental health clinician often plays a vital role in facilitating access to appropriate care.
Clinical Pearls for Navigating Medical Evaluation |
|---|
|
Consider having individuals weighed at home in a more familiar environment. The individuals who are unstable when standing or have comorbid physical disabilities may require a larger scale with more support. |
|
‘White coat hypertension’ might be more prevalent in people with IDD. Portable electronic blood pressure may work well. Home monitors can measure the blood pressure in a relaxed familiar environment. |
|
Blood draws may be best performed in familiar environments. For cholesterol and glucose testing it is sometimes acceptable to use finger stick measurements. Studies have shown that finger stick measurement is acceptable for screening purposes especially in low to moderate risk individuals younger than 65 years. |
|
Screen for cerumen as the first step in hearing screening. Individuals can then have a basic hearing test either in a primary care office or with an audiologist as needed. |
|
Sedation or anesthesia may be required for routine procedures like dental work, endoscopic procedures or minor surgery. |
|
Menstrual related psychopathology: consult the OBGYN to discuss regulation of menstrual periods. Have a lower tolerance to use of NSAIDs for menstrual related changes. |
|
If individuals have any chronic pain condition, rule out exacerbation at the onset of any problem behavior as well as PCP exam and lab work up. |
Clinical Pearls for Navigating Medical Evaluation |
|
|---|---|
|
Diabetes Mellitus |
Sensory Deficits |
|
- Scr - Consult nutrition for poor feeding skills, FTT, obesity, growth retardation, metabolic disorders |
- Screen for subclinical hearing impairment or undetected cochlear pathology |
|
Pulmonary |
Gastrointestinal |
|
- Risk factors: drooling, feeding problems, GERD, aspiration, spasticity, scoliosis - Vaccinate for H. influenza & S. pneumonia |
- Risk factors: cerebral palsy, IQ < 35, scoliosis, anticonvulsants, BZD, non-ambulatory |
|
Menstruation |
Cancer |
|
- Be aware of mood/behavior changes + abnormal bleeding - Transdermal patch > OCP, Depo shot > IUD - Side effects of anticonvulsants & antipsychotics can affect cycling and nutrition - NSAID = pain, self-mutilation, aggression (caution for GI upset) - SSRI = severe mood/physical symptoms in PMS/PMDD |
|
 - Assess hearing q5yr after age 45 (q3yr for DS)
- Assess hearing q5yr after age 45 (q3yr for DS) - Be careful of high risk of recurrent respiratory problems due to muscular weakness, ineffective cough, decreased airway clearance, inadequate lung capacity
- Be careful of high risk of recurrent respiratory problems due to muscular weakness, ineffective cough, decreased airway clearance, inadequate lung capacity  - Be watchful for GERD, constipation (med side effect), fecal impaction, aspiration, malnutrition, pica, colonic volvulus & pseudo-obstruction (acute abdomen), reflux esophagitis (GIB)
- Be watchful for GERD, constipation (med side effect), fecal impaction, aspiration, malnutrition, pica, colonic volvulus & pseudo-obstruction (acute abdomen), reflux esophagitis (GIB) - Encourage regular GYN visits
- Encourage regular GYN visits - Colon CA screening (early detection is difficult due to constipation)
- Colon CA screening (early detection is difficult due to constipation) - Prostate CA screening (same as general population)
- Prostate CA screening (same as general population) - Cervical CA screening (based on sexual and FHx)
- Cervical CA screening (based on sexual and FHx)
Common Presentation of Behavior Change and Possible Etiologies |
|---|
|
Fist jammed in mouth: consider gastroesophageal reflux disease, eruption of teeth, asthma, rumination, nausea, anxiety, painful hands, and gout. |
|
Biting side of hand: consider sinus problems, Eustachian tubes/other ear problems, eruption of third molars, dental problems, pain or paresthesia of the hands. |
|
Biting objects with front teeth: sinus problems [also the most common reason for thumb sucking and bruxism], Eustachian tube or ear problems, finger pain or paresthesia, and gout. |
|
Intense rocking: visceral pain, headache, depression, anxiety, or medication side effects. |
|
Refuses to sit evenly, or at all: hip pain, genital or rectal discomfort, clue to ongoing or past abuse. |
|
Unpleasurable masturbation: prostatitis, urinary tract or genital infection, rectal injury or infection, parasitic infection, syphilis or other ‘old’ conditions, repetition phenomenon [past abuse], or never learned pleasurable masturbation. |
|
Waving head side to side: attempt to supplement visual field, vertigo, or hypervigilance. |
|
Walking on toes: arthritis in the hips, ankles, or knees, sensory integration issues or tight heel cords. |
|
Won't sit: akathisia, anxiety, depression, back pain or other pain, sleep deprivation. |
|
Whipping head forward: Atlantoaxial subluxation [found in 14% of individuals with Down syndrome and others with joint laxity], dental problems, or headaches. |
|
Sudden sitting down or ‘sit down strikes’: cardiac problems, syncope, orthostasis, medication side effects, vertigo, otitis, Atlantoaxial subluxation, seizures, or panic. |
|
Waving fingers in front of eyes: migraine, corneal scarring, cataracts, seizures, glaucoma, or medication side effects i.e. diplopia. |
|
Head banging: depression, headache, dental problems, seizures, otitis, mastoiditis, sinusitis, tinea capitis. |
References
- Gentile JP and Monro M. Medical assessment. Psychiatry of Intellectual Disability: A Practical Manual. Gentile JP, Gillig PM, eds. Chichester, UK: Wiley and Sons, 2012. 26-50/51(abstract page).
- McCarthy J and O’Hara J. Ill-health and intellectual disabilities. Current Opinion Psychiatry. Sep 2011; 24(5):382-6. doi: 10.1097/YCO.0b013e3283476b21.
- McDermott S, Moran R, Platt T and Dasari S. Variation in health conditions among groups of adults with disabilities in primary care. Jrl of Community Health, Vol. 31, No. 3, June 2006. Pages 147-159.
- Ryan R. Intensive conference on dual diagnosis. The Community Circle, Denver, CO. CME Event July 2003.
- Sullivan WF, Heng J, Cameron D, et al. Consensus guidelines for primary health care of adults with developmental disabilities. Canadian Family Physician 2006;52: 1410-1418.
- van Timmeren EA, van der Putten AA, van Schrojenstein Lantman-de Valk HM, van der Schans CP, Waninge A. Prevalence of reported physical health problems in people with severe and profound intellectual and motor disabilities: A cross-sectional study of medical records and care plans. J Intellect Disabil Res. 2016 Nov;60(11):1109-1118. doi: 10.1111/jir.12298. Epub 2016 May 20.
- Wilkinson JE, Culpepper L, Cerreto M. Screening tests for adults with intellectual disabilities. Jrl Am Board Fam Med 2007; 20:399-407.
Biography Julie P. Gentile (jen-TILL-ee), M.D. is
Professor and Chair at Wright State University Department of Psychiatry and is
the Project Director for both Ohio’s Coordinating Center of Excellence in
Mental Illness/Intellectual Disability and Ohio’s Telepsychiatry Project for
Intellectual Disability. Dr. Gentile is a Distinguished Fellow of the American
Psychiatric Association and has evaluated more than 4,500 individuals with IDD.
She has been awarded over $8,000,000 in grant funding to support her dual
diagnosis projects and is the recipient of the American Psychiatric Association’s
Menolascino National Award for Excellence in Psychiatric Services for
Developmental Disabilities. Contact Information Julie P. Gentile MD, DFAPA Professor and Chair Wright State University Boonshoft School of Medicine Department of Psychiatry 2555 University Blvd. Suite 100 Campus South Dayton, OH 45435 937-775-7792
Kline | 28-40
Volume 9 ► Issue 2 ► 2020
Communication: Understanding the Basics, Levels, and Strategies
Erin Kline, M.Ed.
Abstract
Communication is necessary for language to occur. This article will discuss considerations that are foundational in eliciting communication. Building on these concepts, the seven levels of communication, based on an assessment tool used to determine why and how a child/individual is expressively using behaviors or other means to communicate (called the Communication Matrix), will be explained. The levels acknowledge behaviors as: rudimentary, reflexive, advanced, formalized and the many stages in between. Lastly, detailed strategies will be offered to further support and promote growth in each of the seven areas.
Communication and language; people often think they are one and the same. Yet that is not entirely true. One can communicate without the use of language; however, one cannot use language without communication. This article will provide clarification between the two and will focus on communication, specifically for individuals who might not yet be using formalized language. Many people place the emphasis on individuals using language, wanting to know if they are talking or signing yet, without realizing the many foundational skills that must be developed and set in place before language is established.
Communication is defined as the exchange of a message between two or more people.1 There are four key elements that are needed for communication to happen. First, a sender is needed. This is the person who is communicating/expressing the message. Second, a receiver is needed. This is the person who the message is going to. Third, a shared topic is what the two people are communicating about. When trying to motivate communication, one of the driving forces is preferential topics. Everyone communicates about things that are important and of interest to them. Consider this: if someone is passionate about sports and that is where a bulk of their time and energy lies, when somebody approaches them wanting to talk about the prime minister of France, they might not be very inclined to engage in the discussion. However, if that same person wanted to talk about the game winning shot of last night’s championship basketball game, they would naturally be more eager and excited for that conversation. Being aware of what the person wants to give their attention to is essential. Try to avoid broad activities or objects; dig deep and get specific. Notice what they enjoy looking at, listening to, touching, smelling, and tasting/eating. Notice their preferences in toys/objects, textures, people, environments, positions/equipment, movement, vibration, etc. In order to develop and have a repertoire of likes and dislikes, there must be varied experiences, time, and repetition. Reflect on the person’s exposure and experiences in relation to objects, toys, activities, foods, people, and places. Have there been multiple exposures that will enable them to actively decide whether they liked or disliked the experience?
While this may sound basic, there are many factors to consider for an individual who may have limited access to people, places, experiences, materials, and/or objects. The following questions must be considered: What and how many experiences has the individual had? Have they had the opportunity and time to form trusting relationships and attachments with others? Does the individual feel safe and secure enough to communicate? Have they been in an environment with people that are responsive to their vocalizations, movements, and behaviors? Does the individual understand that their behavior(s) can impact those around them? At the very core of communication is cause and effect; the individual does something and someone responds. When developing communication, individuals need to be in an environment where any movements, vocalizations, or facial expressions the individual exhibits are acknowledged, and responded too. Through these consistent responses, individuals learn that their behaviors affect the people around them and, in turn, their needs are met.
When looking at why, there are a plethora of reasons that individuals communicate. The following list is not exhaustive, but includes expressing comfort or discomfort, requesting something, making choices, refusing something, requesting help or attention, showing affection, greeting others, sharing, and asking questions.2
The last of the four elements needed for communication is a mode or a means of expression. There are numerous modes that individuals can use to communicate, a few of which include facial expressions, body movements, signs, words, pictures, objects, augmentative and alternative communication (AAC) devices, and braille. When thinking about the mode or what the communication exchange looks like, it is important to first determine how the individual is communicating and what means are accessible, meaningful, and functional to them. Communication can be described as either pre-symbolic or symbolic.
Pre-Symbolic Communication
Pre-symbolic communication is when the individual engages in behaviors that are either reflexive or purposeful. Reflexive, or pre-intentional behaviors, express the state of the individual (e.g., if they are in pain, wet, or hungry) and typically develop between birth-3 months of age.2 This may look like a change in posture (e.g., stiffen, relax), facial expressions (e.g., grimace, smile), vocalizations (e.g., cry, fuss, scream, coo, squeal), or body movements (e.g., head movements, turn away, lean in, kick legs, extend arms). Purposeful behaviors (similar to those listed above) are intentional, but not intentionally communicative and typically emerge between 3-8 months of age.2 This means that the individual is using these behaviors to affect the other’s behavior, however, with both reflexive and intentional behaviors, it is the other person who is inferring the meaning of the individual’s behavior. An example of an intentional behavior would be when a mother rocking her child stops. The child vocalizes when the rocking movement stops. The child vocalized, which was an intentional behavior, but didn’t turn toward, touch, or look at the adult. It is the adult who interprets the vocalization to mean the child wants more rocking.
Now that the individual has developed consistent behaviors that are intentional, the next step is when communication emerges, either unconventionally or conventionally. The main component that moves an individual’s purposeful behaviors into communication is the emergence of dual orientation. To recap, communication occurs when the individual sends a message about something to someone else; there is a sender, a receiver, a shared topic, and a means of expressing. Dual orientation is when the individual understands that they must communicate a message about something to someone; it is two-fold. An example of this would be when the individual is swinging on a swing. When the movement of the swing stops, to request more they might kick their legs, arch their body back, vocalize, or smile. In addition to these intentional behaviors, the communicator must provide wait time for the individual to involve a communication partner. The individual might move their arm to touch the person pushing them or turn toward where the person is to look at them. Proximity is important. The communication partner should be right next to the individual, talking and touching her/him throughout the interaction, so they are aware someone is there, available to communicate. The communication partner should also be close enough to the individual so that they can easily reach, touch, or turn toward them. Motivating activities/toys are also crucial when encouraging communication. When dual orientation occurs, it is no longer the other person who is guessing or interpreting what the individual’s behaviors mean; the individual is now communicating.
Unconventional communication, defined as “gestures used with the intent of affecting the caregiver’s behavior,” typically emerges between 8-12 months of age.2 With unconventional communication, one typically needs to know the individual or have spent time with them to know what their body movements/gestures mean. Conventional communication, common gestures that most people would be able to understand and interpret (e.g., shakes head “no” or nods head “yes,” points at someone or something, waves or raises hand, etc.), “used with the intent of affecting the caregiver’s behavior,” develops between 12-18 months of age.2
Symbolic Communication
Now that the individual understands the importance of communicating a message to another person, at the symbolic level the communicator begins using symbols (either concrete or abstract). They are generally used one at a time, not yet in combination with more than one symbol. At this point, the individual learns the concept of one-to-one correspondence; the understanding that a symbol is a representation of a specific referent (e.g., a photograph of a green spoon is a concrete representation of the actual green spoon the individual uses during breakfast). Concrete symbols, generally understood between 12-24 months, refer to symbols that “bear a clear perceptual relationship to the referent; they physically resemble the referent in appearance, sound, touch, or motion2” (e.g., a real life photograph, an object symbol, pantomiming the action, or mimicking the sound of the object). Abstract symbols, typically understood between 18-24 months of age, “bear a purely arbitrary relationship to their referents; they are not perceptually similar to them2” (e.g., a braille or written word, a manual sign, a spoken word, or an abstract 3D or 2D symbol, such as a texture, object, picture, or drawing).
Once the individual has these foundational skills (attachment/relationship with others, repertoire of preferences, intentional behaviors, a responsive communication partner, dual orientation, and one-to-one correspondence), the groundwork has been laid for language to occur. This is when the individual combines two or more symbols, according to grammatical rules or syntax, and generally happens around 24 months or age.2
Building on the various levels of communication, moving from reflexive and intentional behaviors, to the emergence of communication (whether unconventional or conventional), to then communicating using symbols (whether concrete or abstract), takes time and practice. When determining if the individual is ready for the next level, the communication partner must assess the ability to generalize, that is, making sure the individual’s responses are consistent across a variety of people, locations, and activities. To help facilitate the development and mastery of these levels, below are intervention strategies that may be beneficial for eliciting communication.
Strategies for Communication Development
Reflexive or pre-intentional behaviors
- Use a variety of active learning materials and preferred objects/textures/activities to encourage purposeful movements and active exploration
- Set up an environment that the individual has access to and is responsive to their movements, behaviors, and vocalizations
- A person familiar with the individual’s vocalizations, facial expressions or body movements immediately acknowledges and provides language in response to the child
- Ex. The child moves their right arm, the communication partner might say, “Oh, I see you moving your arm.” Reaching out to touch the child’s right arm, the communication partner can say, “Are you trying to find your blanket? Here it is!”
- A responsive environment means setting up objects that respond to the child’s purposeful movements
- The individual is positioned next to dangling wind chimes or hanging beads/bells. Even the smallest of movements will generate a response; the sound of the chimes or beads/bells
- Keep a consistent and predictable routine and implement touch/sound/visual cues, so the individual can anticipate what will be happening throughout their day
Purposeful or intentional behaviors
- When the individual makes any purposeful movements, vocalizations, or facial expressions; immediately acknowledge what they did, and respond with what they may be trying to communicate
- The child is playing on the swings on the playground. When the movement stops, and they begin pushing their head/trunk back, the adult might say, “Oh, I see you pushing back, you want more swinging?” and immediately start pushing the swing again
- Give the individual the opportunity to communicate with others. Have “touch conversations” with them about things that are motivating/interesting to them. Notice what they are paying attention to, exploring, or playing with and use mutual tactile attention to let them know that their interest is shared by touching the side of their hand, as well as the item they are interacting with. Follow their lead by imitating their movements and/or playing alongside them. This communicates, "I see you playing with _____ and I’m interested in the same thing you are. Can I play too?" Provide the language for what they are doing, seeing, touching, experiencing, etc.
- Provide opportunities for the individual to engage with activities and manipulatives that encourage turn-taking with another person (joint attention and parallel play). When the individual is interested in an object/activity that a peer is involved in and they approach the peer, model how to engage in back and forth interactions. Also, provide the language for “my turn,” “your turn,” and “wait.”
Unconventional communication
- When the individual communicates using unconventional methods, honor and respond to their behaviors and then model more conventional gestures
- Use hand-under-hand signing and shape the child’s hands into the appropriate handshape for the sign3
- Set up activities that encourage dual orientation. During a preferred activity/object, pause or stop it and provide wait time for the individual to communicate a message to a communication partner
- During activities, proximity will be important; the communication partner should be next to the person, talking and maintaining physical contact with them throughout the interaction, so they are aware someone is there
Offer wait time
- When the individual vocalizes or makes body movements to show that they no longer want an item, encourage them to communicate this message to a communication partner (e.g., by pushing the object away and then looking at the person, etc.)
- Give the individual the option to make choices between preferred activities/items and non-preferred activities/items. Make sure the individual is aware of and looks at/touches both choices being presented and does not just choose the first item they see. Wait for the individual to reach for or sustain gaze with what they want. Then give them the object they picked and pair it with a concrete or abstract representation of it (e.g., photograph of what the object is or the sign or word for it)
- With choice-making, when requesting more of, or when requesting a new activity/object, in addition to the individual looking at or reaching toward the item or photo that they want, we still want them to communicate that message to a communication partner. They can involve a communication partner by reaching to touch, turning toward, or looking at the person, or by handing them the object or photo
Conventional communication
- To encourage the individual to request a new object, set up a box with a few of their preferred objects (so they can see it, but just out of reach). This allows the opportunity to communicate that they want something new/different
- To encourage the individual to request a new activity, begin pairing a meaningful object (preferably one that is used with that activity) and a photo at the beginning of the activity; this symbol will come to be a representation of that specific activity. In turn, they can touch, look at, or reach for the object or photo and then involve the communication partner
- Encourage the individual to request the attention of a communication partner. Begin by positioning within close proximity (next to, touching whenever possible) to the individual and then distancing; encouraging them to seek out the communication partner. Situations may need to be sabotaged to encourage the individual to request attention (e.g., the - activity/object doesn’t begin until they request a communication partner’s attention)
- If the individual throws an object, provide the language for what their behaviors are communicating. Model head shaking for “no” and say, “No, you don’t want the _____? Okay, we can be done.” Encourage the individual to hand the unwanted object to the communication partner (to communicate that they don’t want it) or sign/say “all done,” “no,” or “don’t want.”
- Pair cleaning up and putting the object back in its original location with the word and sign for “all done/finished.” Do this by saying, “all done with the _____,” as well as signing “all done/finished” with the individual’s hands (hand-under-hand)
- Provide opportunities within the individual’s normal routines to greet people and have others greet them at arrival and departure. Model waving hello and goodbye
Concrete/Abstract symbols
- Use concrete symbols in a calendar system to prepare the individual for transitions and refer to the symbols throughout their day3
- Give the individual the option to make choices between objects/activities while pairing the corresponding photo, object symbol, word, or sign with the object/activity prior to interacting with it (reinforcing the concept of one-to-one correspondence using concrete and abstract symbols). When the individual chooses the object or photo symbol of the object/activity that they want, encourage them to hand the symbol to the communication partner, as if communicating, “This is the activity I want to do.” In time, see if the individual can confirm the choice they made (with the object) with the corresponding photo, sign, or word
- When the individual becomes disengaged or it is obvious that they no longer want an item, encourage them to communicate this message to a communication partner, using concrete or abstract symbols. An example of this would be the individual taking the object or photo symbol of the toy or activity they are finished with and placing it in the finished box. Continue to model the signs and words for “all done” and “don’t want” and provide wait time for the individual to express this
- Create a list for “first words/signs/symbols” to share with all team members and ask for their input as well3
Language
- Plan activities that provide opportunities to practice combinations of 2-3 symbols with a variety of people in different environments (if needed, model first)3
- Teach specific grammar, syntax, and other rules of language3
- Provide access to individuals who are fluent in the individual’s specific language mode, including peers, across all environments3
Language is a form of communication, but communication does not necessarily require language. By reviewing the developmental tiers of communication, there are multiple skills that can be built upon in between purposeful movements, understanding communication, and using formalized language. Engaging in activities or with objects and people that are motivating to the individual, sets the stage for communication to be fun and rewarding for all involved.
References
- Stremel, K. Communication interactions: it takes two. DB-LINK. 2004;1.
- Rowland, C. Communication matrix: a communication skill assessment. Portland, OR: Design to Learn; 2004.
- New York Deaf-Blind Collaborative (NYDBC). Communication for learners who are deaf-blind and/or have multiple disabilities; 2016.
Biography
Upon graduating with her bachelor’s degree in Deaf Studies, Erin Kline started her career working with adults who are Deaf-Blind, at the American Association of the Deaf-Blind. This ignited her passion for working with individuals with a dual sensory loss, leading her to pursue her master’s degree in Deaf Education, with an emphasis in Early Intervention with Infants who are Deaf-Blind. She has been working for Delaware’s Statewide Deaf-Blind Program for over 12 years, providing consultation, training and direct services to infants and children who are deaf-blind with multiple disabilities, their families and their Individualized Family Service Plans/Individualized Educational Program teams. She has presented on a variety of topics, including: Cortical Visual Impairment, CHARGE Syndrome, Communication Development and Active Learning. She is also a board member with the National Intervener and Advocate Association.
Contact Information
Erin Kline, M. Ed.
Delaware Statewide Programs for the Deaf, Hard of Hearing & Deaf-Blind
(240) 217-4863
Milcic | 41-53
Volume 9 ► Issue 2 ► 2020
Language Deprivation and Its Implications
Lori R. Milcic, MAP, CI, CT, QMHI
Abstract
When it comes to communication, there are many underlying elements that impact effectiveness. Influences that are often considered are medical conditions, developmental disabilities, or mental health diagnoses, but rarely do we hear about the impact of language deprivation. The need for direct access to language is essential. This article will define language deprivation, its surprising reverberating impacts on daily functioning, and how our responses can support a positive outcome for individuals’ futures.
When it comes to communication, there are many underlying elements that impact effectiveness. Influences that are often considered are medical conditions, developmental disabilities, or mental health diagnoses, but rarely do we hear about the impact of language deprivation. Perhaps this is because language deprivation is considered to be rare, which would be true when describing the typical, modern, hearing population1. However, language deprivation during a child’s developmental years is rampant within the deaf population,1-4 and continues into the adult experiences of individuals with developmental or intellectual disabilities.5-7 The need for direct access to language is essential. This article will define language deprivation, its surprising reverberating impacts on daily functioning, and how our responses can support a positive outcome for individuals’ futures.
Language deprivation occurs when a child does not receive enough linguistic exposure between birth to about five years old to support the development of a fluent, native language. For a hearing person, extreme cases of this have been documented to occur only about once a century.1 This is because it is very difficult to deprive a child of language completely when they are able to passively hear ambient sound all around them from parents, peers, neighbors, crowds, media, and the like. We take in sound and language all the time, without even trying. To deprive someone of that would require intentionality. However, for someone with a hearing loss, the opposite is true. A deaf person passively takes in no language unless someone intentionally exposes them to it in ways they can access, such as through the use of a visual, signed language or with electronic devices like hearing aids paired with active training in speech and listening.1-4,8
Without this intentional linguistic exposure during those key developmental years, a person is at risk of Language Deprivation Syndrome, which is not restricted only to language difficulties but indicates further social and cognitive impairments. In fact, Language Deprivation Syndrome is functionally similar to intellectual disability.3 More information on this syndrome will be defined throughout this article. First, it is important to understand what language deprivation looks like.
Language deprivation can occur in different populations to varying degrees. Imagine the typical communication experience. Conversation is naturally reciprocal; one person speaks, another responds, the first speaks again, and so on. This interaction brings connection and satisfaction. Humans learn from each other, experience each other’s perspectives, share joy and sadness, and more. But what happens if an individual has an intellectual or developmental disability, autism, or any myriad of things that affect the ability to communicate? If a person speaks and no one responds, what happens? The speaker might try a second time, or even a third, but eventually will give up because that reward of pleasure and connection is not achieved. Over time, this pattern is repeated and can lead to a type of language deprivation outside of early developmental periods where exposure to language eventually diminishes.9-12 For children, there may be many structures in place to mitigate this and provide language immersion, regardless of their response. Students are typically in school for several hours per day, exposed to language being used around them, and often experiencing direct support and intensive interventions provided by experts in special education, speech and language pathology, and more. But we know that social opportunities, peer relationships, and community interaction can be limited for children with intellectual or developmental disabilities.9-10 Furthermore, it’s not uncommon for adults to constrain the ways they communicate with this population, limiting their exposure to complex concepts or broader vocabulary.9-11 Therefore, children with intellectual or developmental disabilities may not have a fully immersive language experience commensurate with their typically developing peers. For individuals who have hearing loss and a co-occurring intellectual or developmental disability, the adverse impacts are compounded.13
Unfortunately, there is very minimal research on language deprivation in the adult years; however, there is some evidence of its devastating effects. These impacts can include, but are not limited to, progressive isolation, withdrawal, and decompensation of mental health conditions.10,14-15 Once transitioned into adulthood, many, if not all, of the interventions available during childhood are discontinued, either due to unavailability or the individual’s apparent choice. Consider the previous example of interacting with a non-responsive communication partner. During the developmental years, professionals and lay people tend to have more patience and often feel empowered to do more for a child, directing them to engage in activities they may not seem interested in or providing them with opportunities they did not independently request. The same situation with an adult might evoke a different response. For example, someone might determine that a non-responsive adult does not want to communicate, prefers to be alone, or feels annoyed by repeated prompts to engage. With adults, people feel less empowered to provide experiences that are not explicitly requested by the individual. Additionally, for those adults who require specialized communication modalities (such as the use of assistive technology or American Sign Language), there are often fewer professionals available with the expertise to provide immersive language experiences. Any of these circumstances can lead to an experience of language deprivation in adulthood, leading to waning language skills, progressive isolation, behavioral challenges, and cognitive decompensation.
How serious can these language deficits be? For those who experience language deprivation during those key early years of development, the impacts can be serious enough to lead to a diagnosis of Language Deprivation Syndrome (LDS). While this terminology is relatively new, the data behind it are not. As early as the 1960s, clinicians have been documenting certain observations of functional deficits in people with hearing loss who were not adequately exposed to language during childhood.1,16 A constellation of symptoms was noted in this population, including difficulty sequencing events (describing what came first, second, third, etc.), understanding the concept of time, struggles with cause and effect, lack of Theory of Mind and empathy, and aggressive behavior directed toward self and others.1,3,17 There is also a deficit seen in world knowledge or “common sense”, what is often clinically termed Fund of Information. Dr. Sanjay Gulati1 noted that people with even mild language deprivation can exhibit these symptoms, however, it appears that the severity of the symptoms have a positive correlation to the severity of the deprivation. For adults, the “use it or lose it” principle applies. Individuals who once had access to language and communication and are later deprived of those interactions begin to lose their fluency and can experience impacts across categories of functioning, as well, including cognitive, social, and behavioral/mental health.11,14-15
For children with hearing loss, support systems continue to advocate for outdated intervention approaches while the research grows in opposition. The medical perspective typically encourages fixing the hearing loss with procedures like cochlear implantation.16,18 In parallel, the educational system in our country has leaned toward teaching spoken and aural language for decades.2,4 However, research shows cochlear implant (CI) success rates as low as 30% with spoken language fluency2,18 and negative impacts for these children in social gains, as well.2,4,16,18 There simply is insufficient research available to justify the oral/aural approach as the top choice of physicians and educators across the country. However, there is a great deal of data available that supports development of any fluent, native language (especially sign language) for positive achievement in all areas of development for this population.1-4,8,14,16,18-19 In other words, immersion in a visually accessible language, like sign language, would be a better foundation for further learning and development, or to gain back language that has been lost due to deprivation occurring in adulthood. In fact, there is some promising empirical research on this, as well, including Functional magnetic resonance imaging (fMRI) studies that show positive brain changes for teenagers with severe language deprivation experiences after living in an immersive language environment, a place where they had access to sign language all day, every day.20
One excellent example of a person dealing with Language Deprivation Syndrome is the story of Sonya (pseudonym). She was a profoundly deaf child who had no access to language from birth to age ten. No one knows whether she was born deaf or lost her hearing due to an illness later in childhood. However, during her developmental years, she could not hear well enough to make out the sounds of English and was not provided access to American Sign Language. Therefore, she learned to use behaviors to communicate, albeit ineffectively. By age ten, her behaviors had become aggressive and dangerous to both herself and others. Her large physical size, together with her aggressive behaviors, led to feelings of fear in others and an inability to keep her safe. At this time, she was placed in a behavioral health program that specialized in supporting children with hearing loss. This was an immersive American Sign Language (ASL) program, meaning that all students and staff used ASL to communicate. Over time, Sonya began to learn this language and after a while, she began to use that language to connect with other people and to make her feelings and needs known. Her aggressive behaviors eventually ceased altogether and today, she is thriving as an adult with many friends, a job, and her own apartment. However, because she had no access to language for the first ten years of her life, she still struggles linguistically. She is unable to “time stamp” events that occurred before she learned ASL. When she describes experiences in her youth, she cannot tell you when or where they happened, nor can she answer direct questions about those experiences. She doesn’t know the names of people or places that appear in these stories and often tells memories out of order. She also cannot tell you how many total years she remained in the behavioral health program. Sonya struggles, even to this day, with language dysfluency. While she uses ASL very well today, there are still grammatical elements missing from her expressive language that can leave communication partners guessing at who did what to whom, or where an event occurred, or whether she is telling a story about her past or talking about a dream for her future. She continues to struggle with abstract concepts and common world knowledge.
Max’s story reveals another side of the coin. He was born with hearing loss and an intellectual disability and attended deaf-focused education programs throughout his schooling years. He was moderately fluent in ASL as a child and enjoyed relationships with peers and caring adults at school. His family, who loved him very much, did not use ASL at home. When Max (pseudonym) became an adult, he transitioned into a residential program for people with intellectual disabilities in his home area, which was rural and had few resources for people who use sign language. His support staff were very caring, but they only knew about ten words in sign language. Max was unable to be understood in his native language, ASL, and received communication through a few signed words, gestures, and pictures. Max learned to accommodate this change and began using gestures and pictures expressively, as well. Over the years, support staff came and went and eventually everyone thought this was how it had always been for Max. Then one day, many years later, Max met someone who used ASL with him. His face lit up with joy and he was able to communicate in his native language again. The support staff were amazed. No one knew that he had been fluent in ASL or that he was a social person. It was widely believed that he preferred to be alone and did not wish to communicate much, other than to request items he wanted by pointing or gesturing. Max knew he wanted to live in an environment where people used ASL. Unfortunately, by this time, Max had forgotten a great deal of sign language. He could not remember basic vocabulary and did not use complete, grammatical sentences. It was hard for him to make his desires clear to others. He struggled with many of the same language issues Sonya did, even though he had known ASL in the past. At his advanced age, he never did regain his ASL fluency back completely, but moving into an accessible environment allowed Max to thrive in community and with connection.
So why is an understanding of language deprivation and its impacts important? First, it is essential to recognize that language deprivation has far reaching implications on an individual’s functioning. It’s not just that a person may not know the vocabulary
to discuss a topic, but that multiple areas of social and cognitive functioning can be impacted. Second, remediation requires intensive language immersion. This approach has the added benefit of not only improving language fluency but impacting social
and cognitive gaps in a way that reverberates into all areas of everyday life. Furthermore, when someone has experienced language deprivation, whether in childhood or adulthood, we cannot accurately diagnose their needs in other domains until we address
the communication gap. It is impossible to recognize where support needs lie unless the impacts of language deprivation can be identified for each individual. Once communication needs are met, the veil is lifted and the need for other interventions
becomes clearer. Support services will continue to encounter frustrations if they put the cart before the horse.
The biggest takeaway here, is to start with effective communication. Children and adults both need access to a mode of communication that provides them with the highest possibility of fluency, whether that is a spoken language, a signed language, or even an alternative or augmentative communication mode. The mode may differ based on the individual, but the need for intense immersion across all settings remains a common thread. The good news is that with an immersive communication environment, great strides can be made across multiple domains and positive changes can occur in people’s lives, no matter their age.
References
1. Gulati S. Language deprivation syndrome. In: Glickman NS, Hall WC. Language Deprivation and Deaf Mental Health. New York, NY: Routledge; 2019: 24-53.
2. Hall ML, Hall WC, Caselli NK. Deaf children need language, not (just) speech. First Language. 2019;39(4):367-395. doi:10.1177/0142723719834102.
3. Hall WC, Levin LL, Anderson ML. Language deprivation syndrome: a possible neurodevelopmental disorder with sociocultural origins. Social Psychiatry and Psychiatric Epidemiology. 2017;52(6):761-776. doi:10.1007/s00127-017-1351-7.
4. Hall WC. What you don’t know can hurt you: the risk of language deprivation by impairing sign language development in deaf children. Maternal and Child Health Journal. 2017;21(5):961-965. doi:10.1007/s10995-017-2287-y.
5. Johnson H, Douglas J, Bigby C, Iacono T. Social interaction with adults with severe intellectual disability: having fun and hanging out. Journal of Applied Research in Intellectual Disabilities. 2012;25(4):329-341. doi:10.1111/j.1468-3148.2011.00669.x.
6. Walton KM, Ingersoll BR. Improving social skills in adolescents and adults with autism and severe to profound intellectual disability: a review of the literature. Journal of Autism and Developmental Disorders. 2012;43(3):594-615. doi:10.1007/s10803-012-1601-1.
7. Wilson NJ, Jaques H, Johnson A, Brotherton ML. From social exclusion to supported inclusion: adults with intellectual disability discuss their lived experiences of a structured social group. Journal of Applied Research in Intellectual Disabilities. 2016;30(5):847-858. doi:10.1111/jar.12275.
8. Scott JA, Dostal HM. Language development and deaf/hard of hearing children. Education Sciences. 2019;9(2):135. doi:10.3390/educsci9020135.
9. Forrester-Jones R, Carpenter J, Coolen-Schrijner P, et al. The social networks of people with intellectual disability living in the community 12 years after resettlement from long-stay hospitals. Journal of Applied Research in Intellectual Disabilities. 2006;19(4):285-295. doi:10.1111/j.1468-3148.2006.00263.x.
10. Gilmore L, Cuskelly M. Vulnerability to loneliness in people with intellectual disability: an explanatory model. Journal of Policy and Practice in Intellectual Disabilities. 2014;11(3):192-199. doi:10.1111/jppi.12089.
11. Kenneally SM, Bruck GE, Frank EM, Nalty L. Language intervention after thirty years of isolation: a case study of a feral child. Education and Training in Mental Retardation and Developmental Disabilities. 1998;33(1):13-23.
12. Ramirez NF, Leonard MK, Davenport TS, Torres C, Halgren E, Mayberry RI. Neural language processing in adolescent first-language learners: longitudinal case studies in American sign language. Cerebral Cortex. 2014;26(3):1015-1026. doi:10.1093/cercor/bhu273.
13. Bruce SM, Borders C. Communication and language in learners who are deaf and hard of hearing with disabilities: theories, research, and practice. American Annals of the Deaf. 2015;160(4):368-384. doi:10.1353/aad.2015.0035.
14. Marrone N, Ingram M, Bischoff K, Burgen E, Carvajal SC, Bell ML. Self-reported hearing difficulty and its association with general, cognitive, and psychosocial health in the state of Arizona, 2015. BMC Public Health. 2019;19(1):875. doi:10.1186/s12889-019-7175-5.
15. Xin Ye, Dawei Zhu, Siyuan Chen, Ping He. The association of hearing impairment and its severity with physical and mental health among Chinese middle-aged and older adults. Health and Quality of Life Outcomes. 2020;18(1):1-8. doi:10.1186/s12955-020-01417-w.
16. Humphries T, Kushalnagar P, Mathur G, et al. Avoiding linguistic neglect of deaf children. Social Service Review. 2016;90(4):589-619. doi:10.1086/689543.
17. Peterson CC, Siegal M. Deafness, conversation and theory of mind. Journal of Child Psychology and Psychiatry. 1995;36(3):459-474. doi:10.1111/j.1469-7610.1995.tb01303.x.
18. Humphries T, Kushalnagar P, Mathur G, et al. Cochlear implants and the right to language: ethical considerations, the ideal situation, and practical measures toward reaching the ideal. Cochlear Implant Research Updates. 2012. doi:10.5772/35558.
19. Murray JJ, Hall WC, Snoddon K. Education and health of children with hearing loss: the necessity of signed languages. Bulletin of the World Health Organization. 2019;97(10):711-716. doi:10.2471/blt.19.229427.
20. Mayberry RI, Kluender R. Rethinking the critical period for language: New insights into an old question from American Sign Language. Bilingualism: Language and Cognition. 2017;21(5):886-905. doi:10.1017/s1366728917000724.
Biography
Ms. Milcic has spent decades studying language deprivation, both formally and informally, and is currently pursuing her doctoral degree in developmental psychology with a research emphasis on Language Deprivation Syndrome. She is fluent in American Sign Language, holds the rare Qualified Mental Health Interpreter specialty certificate, and currently serves as the Deaf Services Coordinator for the Pennsylvania Department of Human Services.
Contact Information
Lori R. Milcic, MAP, CI, CT, QMHI
PA Office of Developmental Programs, Special Populations Unit
301 Fifth Ave, Piatt Place, Suite 490, Pittsburgh, PA 15222-1210
412-252-2315
Millar | 54-68
Volume 9 ► Issue 2 ► 2020
Recognizing Limited English Proficiency within the Disability Community
Amy Mathewson Millar
Abstract
Individuals with limited English proficiencies (LEP) face significant barriers within the disability community, concerning equal recognition of needs and access to services and support at alarming rates, in contrast to English proficient individuals. The current areas of need to remedy this long-standing gap, that violates the Americans with Disabilities Act, are found in building trust, improving access to professionally trained interpreters/translators, and addressing systemic bias to prompt micro-progressions towards universal change, ensuring that all limited English proficient individuals with disabilities have equal access to services and supports in their everyday lives.
The Problem
Individuals with limited English proficiency (LEP) face significant barriers and are often forgotten within the disability community as it relates to gaining equal recognition of needs, access to services, resources, and support at far greater instances than those that are English-speaking. A Philadelphia Latnix Advocate and primary caregiver to children with disabilities, “M”, shared one of her own horrifying experiences when she was at her child’s medical appointment:
The staff had left her door open and she was able to hear the conversation in the next room. A woman was there for her child and had brought a family member to interpret for her. M was not trying to listen but realized right away what the doctor was saying was not what the interpreter was relaying. The child was in dire need of hospitalization for a serious medical need and they should, under no circumstances, go home. The family member incorrectly translated that it was serious, but she didn’t know all the words he was saying and thought she heard they could go home. M alerted staff who didn’t have any available professional interpreters, so they brought M into the family’s room where it was learned that the family member had LEP herself and lacked the understanding to properly interpret, even though she was only trying to help.
This situation could have resulted in serious complications or death for the child due to the mere lack of a professional and well-trained interpreter, not to mention that this instance was a violation of the Americans with Disabilities Act (ADA) and
the Health Insurance Portability and Accountability Act of 1996 (HIPAA). This scenario happens more often within the disability and global community than anyone would care to admit, which could be remedied by recognizing the needs of those with LEP
and improving access to professionally trained communication specialists, translators, and interpreters. According to the United States Department of Health and Human Services, “If English is not your primary language and you have difficulty communicating
effectively in English, you may need an interpreter or document translation in
order to have meaningful access to programs funded by the Department of Health
and Human Services (HHS). Title VI of the Civil Rights Act of 1964 requires recipients of Federal
financial assistance to take reasonable steps to make their programs, services,
and activities accessible by eligible persons with limited English proficiency. 1”
The Americans with Disabilities Act (ADA) did propel advocacy efforts for individuals with disabilities and their families. Maureen Devaney and Audrey (Dee) Coccia were two leading forces at that time and went on to create Vision for Equality (VFE), a grassroots 501(c)(3), in 1996 to address the growing needs of families of individuals with disabilities who often are caregivers for their loved ones. VFE has long differentiated itself from other advocacy organizations with its unique “for families, by families'' approach. VFE’s staff and volunteers consist of people with disabilities, including those with LEP, and family caregivers providing a fidelity that system-based approaches lack. VFE has worked tirelessly as a unique organization dedicated to people with intellectual disabilities and autism in Philadelphia and throughout the state of Pennsylvania. Each year, VFE provides training to teach thousands of people with intellectual disabilities and autism and their families about services, supports, current laws, and best practices so that they can become their own advocates and, in turn, assist others.
It was clear to VFE over the years that for families with LEP, more needed to be done, even now as the 30th anniversary of the ADA was celebrated in July of 2020. Navigating the disability system is challenging and daunting for all families. Yet, little is done to bridge the gap for those that wait for services, especially for those with LEP.
VFE has always supported the advancement of assistive technology for communication for all people; however, in 2004, VFE began their outreach to the families that shared an intersectionality of disability and LEP within the Latino community. Latino Services of Vision for Equality, Inc. advances information, advocacy, training, and resources to ensure that the Hispanic community has the knowledge and tools needed to make well-informed choices to improve their quality of life across Pennsylvania.2 While VFE has been a leader in providing accurate and valuable information to individuals with disabilities and their families for many years, Latino Services works to provide the same access to training and technical assistance for the Spanish-speaking community. This work has enabled many families with LEP to enhance their abilities and close the cultural gap so that they have a better opportunity to connect with needed programs, services, and providers.
Vision for Equality’s co-executives have worked to create systemic and generic social change for all individuals and their families within the disability community, to have the support they needed at the time that they needed them to flourish in their lives. Some of their first experiences reaching families with LEP came from the closure of a Philadelphia Latino-focused provider in the early 2000s, leaving a number of people being cared for in group home settings where both the individual and their family had LEP with no real support or options. It was challenging to interface, support, and understand the unique needs of the individuals and families. VFE had previously formed the Philadelphia Parent Support Groups through their partnership with Philadelphia County’s office of Intellectual disAbility Services. As caregivers themselves, they were moved by the level of need these families had, which led to the creation of the Latino Parent Group. Their approaches naturally brought families to VFE’s doorstep that were desperate and facing lack of access to state systems, policy makers, and supports due to LEP. It became clear that there was a need to have a dedicated department to serve the Latino Community and their work continues today. Dee Coccia, at nearly every meeting she attends for decades, asks the same question, “What are we doing to reach those with LEP and cultural barriers?” Often there is silence or the standard response, “If we get a request for materials or an interpreter in another language, we will honor it.” Which begs to question: how would one make that request if that organization, system, or agency’s website, materials, and offices are geared to or produced solely in English?
“My experience as a Latino parent of children with ID is that when a professional wrongly assumes that I have the knowledge and awareness of language and terminology used in the ID system, especially the acronyms. I don’t expect all resources to be translated, but with today’s technology at least have it on the organization’s website. Professional translators, with no ties to the family or the organization, are needed so that they can remain neutral at meetings (schools, hospitals, etc.). I feel uncomfortable bringing a friend or family member or having someone else from the organization translate; a third-party translator would be more professional. I like to keep family business private and there were a few events when the person translating needed more help than me because they lacked the professional training in translation or the disability community.”
A pivotal moment in this movement came when a member of Vision’s Latino Services Department approached the then Deputy Secretary of the Office of Developmental Programs at a largely attended statewide meeting. She handed the Deputy Secretary a document and she asked, in front of all attendees, that he read it and use it in the meeting. He replied, “I cannot read this, it is all in Spanish.” She explained, “Exactly. This is how I feel when you present the meeting materials to me.” This brought recognition to the critical need to do more and made way for the Latino Services and family group to be recognized and supported by policy makers both in solidarity and fiscally. It has been more than a decade since that meeting, and while there have been many strides to date, many statewide materials, websites, and offices are still solely geared exclusively to those with English proficiency, discriminating against those with LEP.
Current Areas of Need
Working around this topic of recognizing those with LEP, several individuals were asked to share their personal and professional experiences in a virtual round table discussion in June of 2020. When addressing how to improve the reach, recognition, and support of those with LEP, there were three clear themes from their perspective: trust, lack of access to professional and knowledgeable translators and interpreters, and systemic bias. It was clear that there was a vast need for more micro-progressive movement by all members of the disability community, from self-advocates to top policy makers, to address these needs and move toward a more equitable disability community for all people that have intersectionality with LEP and disability. This is not limited to the Latino, HOH, Deaf, or Blind communities but includes all communities with LEP.
Trust
The Merriam-Webster dictionary defines trust as, “assured reliance on the character, ability, strength, or truth of someone or something or one in which confidence is placed, or dependence on something future or contingent: hope.3” For those with LEP, trust is and always will be at the forefront. They must fully trust the person interpreting and the accuracy of translations. They must also trust the agency, county, or organization to provide what was promised. Often agencies wonder why participation from LEP families is low for their events; lack of trust is often the issue. It must be earned and built. It is also why “For Families, By Families” and “Nothing About Me, Without Me” approaches are best in reaching disparate groups of people, including those with LEP.
VFE built that trust among the Latino community over time by employing and empowering family members that were caregivers with LEP who faced barriers themselves and who were eager to assist others within their community while actively listening to families’ needs. They were authentically supported with training and education. They recognized the need for more simultaneous interpretations, as often LEP individuals are asked to attend events in a separate room or location all together, highlighting that they did not have equal access.
State policy makers wanted to hear from the Latino community and a large event was to be held with interpreters through VFE, but policy makers would have required the gathering of the names and contact information for all those in attendance, in order to allow the event to take place. VFE advocated that these families, many of whom were undocumented or facing immigration challenges, would not attend if required to sign-in or provide their information as required by the state, and they won. The event was held in Philadelphia and drew a crowd of over 1,000 people, all eager to learn how to navigate the disability system and find support for their loved ones with disabilities. It was the first large, inclusive gathering of Spanish-speaking families in the state around disability services. Had it not been for VFE’s advocacy, a sign-in sheet would have prevented this valuable event.
Trust must first be built in order to reach those with LEP. Respecting culture is also important; often we expect others to fit into our culture rather than taking the time to understand their unique needs. This takes time, effort, and utilizing representatives that embody and identify with that culture. The need for diverse approaches and efforts for individual and family groups must be rooted in the trust built between systems-related organizations and those they wish to support by utilizing the individuals with LEP as leaders for all efforts.
Access to professional interpreters and translators
Many of the examples shared from the round table focused on the need for true access to professional, well-versed translators and interpreters that also have experience and understand the disability community including medical terminology, understanding of services and procedures, and access to resources for effective interpretation and translation. As of June 2020, there are currently a staggering 7,099 spoken languages in the world; in the United States, there are 347 spoken languages.4 The barriers in locating a trained professional are compounded by costs, scheduling constraints, and an underutilization of available technology. Often, the provision of mandated auxiliary aids under the ADA is not provided by organizations, even when requested, due to lack of known professionals with the appropriate knowledge base coupled with the fiscal impact. Furthermore, there is deep-rooted bias that this need is unnecessary, excessive, and burdensome when, in fact, it is an inherent right under the ADA. Many LEP families are either left out or rely on neighbors, family members, or friends to act as their interpreter. Yet this requires them to have those relationships in the first place, as well as the needed trust. When accessing needed disability services, medical care, and supports; not having a professional interpreter or translation can also violate HIPAA and put the individual at risk.
As mentioned, M, is a Latinx family caregiver, translator, and interpreter. To her, the biggest problem, fueled by a lack of professional interpreters and translators, is the isolation experienced by those with LEP. In seeking assistance, often individuals or families don’t understand what the professional entity is trying to communicate, contributing to a lot of misunderstanding, isolation, and frustration. They must often rely on friends or family members as interpreters and, in doing so, lose some of the information because the person who is interpreting or translating does not understand a term or acronym. In addition, many agencies do not have the necessary information in varied languages, further isolating individuals and families with LEP. From her experience, many individuals use Google to translate documents which, while helpful, is not always accurate or understandable.
Many times, the information is not family-friendly, with too many confusing terms. Even if the translation is done at a professional level, if the individual or family has limited understanding of disability-related terms, it too can be lost in translation. Terms and acronyms can be complex and difficult to translate. M herself works with a diverse team when doing translations, several of whom speak a varied dialect of Spanish, and will often consult with outside resources to ensure that the translation is done properly. This lengthier process ensures that the translation is at a superior level and accessible for individuals who may also have communication or intellectual disabilities in addition to LEP.
In languages that have various dialects, there are many homonyms that are written and spoken the same but have different meanings. For example, in Spanish, “mañana” can mean both tomorrow and morning. In Korean, 배 [be](bae) can mean ship, stomach, or pear. 5 If an organization utilizes a word incorrectly, this could create confusion. Agencies that want to address the needs of LEP communities must have information in diverse languages that are also easy to understand. Additionally, agencies must work toward having a more diverse staff that understand unique cultural needs, so they can build relationships and capacity, and ensure access to professional interpreters and translators.
Timely access to information is critical for all people, but especially for those with LEP and disabilities. The COVID-19 pandemic demonstrated the lack of timely translated materials, professional medically versed interpreters, and diverse delivery of information, putting lives at risk. The need for translations should not solely be produced upon request, especially in a crisis, but rather equal access to information for all people must always be a shared responsibility.
Systemic Bias
My belief is that bias is innately rooted in preconceived notions that have no factual foundation and are formed by a lack of ability to adjust one’s “cultural lens” through which they view a person, scenario or concept. Bias has impacted the disability community long before the ADA, and long after as well. There is a systemic learned, ableist bias for those with disabilities. Those with LEP do not suffer simply because of their LEP; they suffer because of systemic bias that creates barriers based on the idea that bridging the gap to meet their need is too complex, would require substantial strain, and would force organizations to address learned ableism and bias.
“B”, a well-respected Latino advisor based in Harrisburg, Pennsylvania shared that while she does have knowledge of system-based terminology and has English proficiencies today, her accent creates stigma and barriers that come from a place of bias that she must not understand English, or lacks intelligence or expertise. She recalled a time in her career where she was promoted but her coworker did not celebrate with her. Rather, the co-worker expressed, “There is no way I am working under a dumb Mexican. She can’t even speak English!” Her accent brought out deep-rooted bias that ignored her training, skill, knowledge, and experience. In comparison, “N”, a Philadelphia-based professional in the disability community, has no noticeable accent from her country of origin, yet has experienced similar bias in reverse. She is too “Americanized” to be someone that understands the needs of her cultural community, even though she has deep connections to her culture, has faced her own barriers, and is still going through a lengthy immigration process herself. Hard of hearing and Deaf individuals can also experience this interchangeable bias. Additionally, when interpreters are assumed only needed and provided for the formal part of a meeting, not before or after when many attendees network and converse, it leaves those with LEP out of conversation and connections.
Bias can impact all areas of life including access to care. B shared an experience when her daughter, who has intellectual and medical disabilities, was bitten in the face by a dog and sought care at her local hospital. They placed her in a hallway and told her they had to wait for the interpreter, while she held her bleeding child in her arms for hours. The staff treated her as though she was a burden, solely because of her LEP at the time. She pleaded for help, but no one understood, and her daughter waited needlessly for care. A security guard offered her a handkerchief for her daughter’s injury, the only care this hospital provided. She finally called a hospital much further away. When they arrived, the second hospital was ready to treat the child without barriers, with interpreters and staff that were sensitive to the language and cultural needs of the family. “Hospital shopping,” a term indicating the need to shop around to find competent, proper care that is not clouded in stigma, bias, or lack of capacity to treat the unique needs of those with disabilities and LEP, is a term very familiar in the disability community, especially among those with LEP. This is particularly problematic in rural areas where there may only be one provider or hospital.
From an advocates’ perspective, it was clear that systemic bias raised its head front and center during the COVID-19 pandemic for those with LEP significantly beginning with lack of equal and timely access to information. Care was rationed for those disabilities. Language barriers and the lack of understanding that a support person is not a “visitor” for an individual with a disability or LEP, but rather an essential, life-sustaining, mandated, auxiliary support resulted in traumatic experiences and life-threatening conditions. Rationing of care and denial of support persons endangered lives even at world renowned facilities. These barriers, rooted in bias, violate the individual’s right under the ADA and must be remedied as we look for sustainable long-term solutions.
Conclusion
Recognizing the needs of those with LEP within the disability community requires trust, access to professionally trained translators and interpreters, and addressing systemic bias at all levels including material production, technology utilization, service
delivery, and training for individuals, families, and professionals. While this is a large and critical problem, the solution does not have to be a singular, massive change. Rather, it can be found within micro-progressive movement at all levels.
If, at each interface, local providers, counties, community partners, policy makers, and legislators make conscious efforts to create trust, build access to professional, accurate interpretation and translation while addressing systemic bias, the
needs of those with LEP will be recognized and met. Rather than seeing LEP as the barrier, antiquated barriers must be removed. By doing this, the needs of those with LEP will finally be recognized and it will lead to authentically upholding
the ADA and diversity within the disability community for all individuals and families.
Reference
1. Health and Human Services. Limited English Proficiency (LEP). December 19, 2019. https://www.hhs.gov/civil-rights/for-individuals/special-topics/limited-english-proficiency/index.html. Accessed June 30, 2020.
2. Vision for Equality. Latino Services. https://www.visionforequality.org/programs/#prg5. Accessed June 30, 2020.
3. Trust. Merriam-Webster. June 20, 2020. https://www.merriam-webster.com/dictionary/trust. Accessed June 30, 2020.
4. Michaels S. How Many Languages Are There in the World? June 3, 2019. https://www.worldatlas.com/articles/how-many-languages-are-there-in-the-world.html.
Accessed June 30, 2020.
5. Choi M. Same Words with Different Meaning in Korean. October 16, 2018. https://medium.com/story-of-eggbun-education/same-words-with-different-meaning-in-korean-1-fe0be46ed3c3.
Accessed June 30, 2020
Biography
Amy Mathewson Millar is a well-respected Disability Self-Advocate, primary caregiver to three children with medical needs and disabilities, and in addition to her role at Vision for Equality, is a member of the Pennsylvania Developmental Disabilities Council. She is a nationally and statewide recognized keynote speaker, facilitator, and trainer on a variety of platforms around disability and supporting families since 2010. Addressing stigma and honoring intersectionality within the lived disability experience are the focal points of her personal and professional work and advocacy.
Organization: Vision for Equality
Vision for Equality (VFE) is a grassroots 501(c)(3) non-profit organization founded almost 25 years ago to address the growing needs of families of individuals with disabilities who often are the primary caregivers for their loved ones. VFE has long differentiated itself from other advocacy organizations with its unique, “For Families, by Families” approach that systematic approaches lack. VFE has worked tirelessly as a unique organization dedicated to people with Intellectual Disabilities and Autism in Philadelphia and throughout the state of Pennsylvania.
Contact Information
718 Arch Street, 6N Philadelphia, PA 19106
267-773-5287
Northridge, Edwards | 69-85
Volume 9 ► Issue 2 ► 2020
Communication Assessments for Individuals Who are Deaf/Hard of Hearing and Have Other Disabilities
Jesse Northridge, LCSW
Erin Edwards, BCBA
Abstract
Communication assessments are potentially useful tools for capturing the strengths and needs of individuals who are deaf and have other disabilities. This paper offers insight into strategies for conducting an assessment, an overview of common jargon, the benefits of including formal and informal assessment data and considerations of cultural competence.
Introduction
Individuals with an intellectual disability (ID) or other developmental disability (DD) often present with communication challenges requiring assessment and treatment. Within the diagnosis and treatment of communication challenges, individuals have various strengths and needs. Some may be able to speak fluently with a large vocabulary, but struggle with receptive understanding; others may understand spoken word well, but struggle with effective expressive communication. Some people may be adept at reading social, non-verbal communication and others may miss these cues. These are just a few examples of the complexity in communication among individuals with ID/DD. Communication assessment becomes even more challenging among individuals with additional disabilities, such as sensory impairments (deaf/hard of hearing, deafblindness) as many of the assessment tools are not validated across populations.
Individuals who are deaf and have other disabilities (DWD) such as ID/DD are at a higher risk for mental health, physical health, and cognitive challenges.1,2 According to data from the Gallaudet Research Institute, approximately 39% of individuals who are deaf or hard of hearing also have an additional disability.3 Completion of a communication assessment and targeted treatment to strengthen communication, is one strategy for developing individualized intervention plans among persons who are DWD.
This article will review basic concepts and strategies for conducting a communication assessment among individuals who are DWD. The first section addresses components to include within the assessment while the second section reviews some of the common terminology used within the literature.
Beginning an Assessment
When completing a communication assessment, it is important to consider how and by whom it will be used.1,4 Assessments can be utilized by teachers to improve instruction techniques. They can be utilized by behavioral health clinicians for the purposes of improving functional independence and psychological wellbeing. They can also be utilized by healthcare providers to improve an individual’s physical health and ability to self-advocate. Families may also utilize the assessment to help secure additional services or benefits, such as through Medical Assistance or the Social Security Administration. The purpose of the communication assessment should be focused on helping the intended audience understand the strengths and needs of the individual within specific contexts.
Neild and Fitzpatrick noted there are factors which may influence an individual’s communication. Among them, the authors identified “(a) degree of hearing loss, (b) primary language used at home, (c) age of on-set, (d) presence of other disabilities, (e) race, (f) gender and (g) socioeconomic status.”5) Given the complexity of assessing individuals who are DWD, it is recommended that assessments and recommendations include collaboration with multiple disciplines. 1,6,7 For example, an individual with physical limitations may struggle if recommended for learning sign language to communicate. Similarly, an individual with visual impairments may not be able to notice visual cues unless presented within their field of vision. The assessment team may include psychotherapists, speech and language therapists, occupational therapists, physical therapists, and physicians. Each of these disciplines can help to gather information regarding the individual’s abilities and needs. They may also be able to offer suggestions for ways of supporting the individual being assessed, such as ways to adapt/modify existing assessment instruments.
According to one article, a communication assessment should “describe the individual’s communication abilities; the skills, needs, culture, and behaviors of their communication partners; and the communications supports and demands presented by different environments.” 7 Notable in this recommendation is that not only the individual themselves should be considered, but also behaviors and preferences of the natural supports that they will be communicating with, as well as the contexts in which the individual will be expected to perform the communication skills. The U.S. Office of Special Education Programs and the Perkins School for the Blind have offered guidance on questions and information to include in an assessment. Please see the appendices for some of these examples.
Another format for communication assessments is to utilize dynamic assessments (DA). Dynamic assessment involves both assessment and intervention by placing an “emphasis on the process of learning (the how) rather than the result (the what).”8 It involves an initial assessment followed by intervention and follow-up assessments to track the most effective ways of teaching an individual new material. Mann8 argues that DA may be a more effective assessment for deaf learners, as it focuses on the individual’s current learning strategies as well as his/her responsiveness to various teaching interventions, rather than simple task performance. However, DA is intended to be an ongoing process over time and may be more appropriate in a school or day program, and not as available in a short-term, clinical setting.
Fundamentals of Communication
Before conducting a communication assessment, it is imperative to understand the jargon associated with the literature. Two of the important terms to understand are expressive and receptive communication. Expressive communication refers to an individual’s ability to send messages to another person. For example, when assessing expressive communication, a clinician may ask the individual to label/name an item, ask for a preferred item or activity or respond to a question. The individual would vocalize, sign or use other Augmentative or Alternative Communication (AAC) to communicate. Alternatively, receptive communication refers to an individual’s ability to understand what another person is communicating. In testing receptive communication, typically a clinician may ask an individual to point to a picture or object that has been named or follow a direction that is given verbally without a model or gesture accompanying it. In assessing individuals who are DWD, the incoming communication will need to be adjusted to match the individual’s strengths and experience. Signing, lip-reading, and gestures may be what the individual understands best; or pictures, symbols, braille, or text may be used for the individual to match to behaviors or responses. When conducting assessments, clinicians must understand that an individual’s abilities within each of these categories may be uneven and that the methods used for communication may be non-traditional (compared with individuals who are not DWD). Often, parental input will be needed to identify and interpret gestures and subtle signals used in the home. This input will help the clinician to understand the individual’s skill level.
Researchers and clinicians may describe communication using the seven levels of communication development.9 In Level I (preintentional behavior), individuals (typically young infants) do not communicate voluntarily. However, they are able to share messages of distress to caregivers, who then respond to the individual’s needs. Level II (intentional behavior) involves a transition to movements and gestures that are purposeful in nature (i.e. pushing away unwanted items but is not intended to directly send messages to another person. In Level III (unconventional behavior), individuals use behaviors that may be ignored at a young age (i.e. tugging on people and whining) but are not considered appropriate for older individuals. Level IV (conventional communication) uses non-verbal gestures, movements and possibly vocal intonations to communicate (i.e. waving, pointing). These behaviors are considered socially appropriate across the lifespan. Level V (concrete symbols) is often skipped by individuals without disabilities. However, it involves the use of symbolic gestures or vocalizations (i.e. mimicking the sound of something they desire). Words, both spoken and printed, begin to appear in Level VI (abstract symbols). However, language is typically limited to a singular word at a time. It is not until Level VII (language) that individuals are able to begin forming phrases. For individuals with DWD, it is possible that different types of communication fall across different levels. For example, mands (requests) may be observed at a higher level of speech development than protests (saying no). A thorough assessment may seek to identify types of communication that fall at lower levels, in order to target them to strengthen through intervention.
Furthermore, Taylor’s 10 article on assessing individuals who are DWD noted there are six parameters of communication assessments. Sensory abilities refer to an individual’s ability to process audio and visual cues. Motor abilities are a person’s abilities (and limitations) of movement when communicating. Of note, this also includes a person’s oral-motor abilities, which impact articulation of vocal speech. Paralinguistic behaviors are non-verbal cues of communication (proximity, body language, facial expressions, etc.) as well as variations in speech (volume, pace, intonation, etc.). Linguistic abilities refer to an individual’s ability to form, modify and use words. Within this domain, it may be beneficial to note morphological abilities (i.e. prefixes and suffixes), syntax (the sequence and grammar of phrases) and semantics (the intended meanings of phrases). Finally, pragmatic communication refers to how messages are used and interpreted, particularly in varying social contexts. Pragmatic communication can vary widely depending on the communication partners and the settings.11 An assessment across these parameters, with particular attention to the sensory domain (e.g., visual cues, such as orienting and attending to the communication partner), motor domain (e.g. ability for oral motor and/or fine motor for signing), and receptive and expressive paralinguistic behaviors (e.g. use of body language facial expression or touch) may provide information to help match the individual with DWD to a communication system that will best fit their personal strengths.
Formal vs. Informal Assessment
In a study from the United Kingdom, over 76% of speech and language therapists reported using both formal and informal assessments among individuals who are DWD. 12 Boesch13 noted that formal assessments may be needed for differential diagnoses or to secure government benefits. However, informal assessments are likely to provide greater (and possibly more useful) information.
As mentioned above, professionals from a variety of disciplines may utilize a communication assessment to guide and improve interventions. Regardless of an assessment’s eventual utilization, professionals in every domain regularly strive to utilize standardized instruments for their assessment protocols. Standardized instruments can help with a differential diagnosis and compare an individual to same-aged peers. However, formal assessments are rarely validated for use among individuals who are DWD.4,12
One study from the United Kingdom found that speech and language therapists most commonly chose to utilize three assessments: the Preverbal Communication Assessment, the Affective Communication Assessment and the Checklist of Communication Competence.12 However, it was also noted that speech and language therapists regularly adapt and modify assessments based on the needs and abilities of the individual.1 Making these decisions should be done with clinical justifications and with an understanding of how it may alter the results of the assessment. Any modifications to a formal assessment should be noted within the results interpretation.
Given many of the challenges associated with formal assessments, informal assessments may yield more (and higher quality) information.10,14 An informal assessment generically refers to the use of non-standardized instruments. Clinicians may choose to utilize specific portions of a formal assessment, collect data using a personalized instrument or simply record observational data. During interactions with the individual, the clinician should also strive to utilize the individual’s interests (e.g., preferred topics of conversation, preferred items) to promote engagement and gain better understanding of the individual’s abilities. Regardless of the assessment tool used, it has been recommended that assessments take place in the individual’s natural environments, with observations between the individual and their family members, peers and teachers. 7,11,14 In fact, failure to do so may yield inaccurate or incomplete data. “Asking students…to perform a skill in settings other than real life removes the contextual cues they rely on to make sense of the task. Artificial environments such as testing rooms may not give accurate information, especially when students have complex disabilities.”14 Furthermore, “it is preferable to conduct multiple observations in different settings over time, even if the observations are brief.” 1 Observing these interactions between the person being assessed and their natural supports in context can yield a wealth of information regarding subtle communications that are currently effective for the individual, as well as communications that are not. For example, in non-speaking children, it is not uncommon to observe a parent or caretaker responding to a need of the child, when to an unfamiliar observer no obvious communication from the child has taken place. In these moments it is helpful for the clinician to explore further, asking the parent or caretaker how they knew what the child needed. Oftentimes, there is a subtle look, sound, gesture, or movement that conveyed a need. Once understood, this subtle communication, understood by only one or two others, can be shaped into a communication that can be understood by a broader population of adults, peers, or caretakers.
Cultural Competence
To someone unfamiliar with deaf culture or unfamiliar with standardized testing instruments, it may be tempting to simply ask that an interpreter aid with translating assessment tools. However, it is important to note that assessments and translations are both filled with complexity.15,16 For example, an interpreter may not recognize the significance of various words and phrases and may unintentionally convey altered meanings to the individual or the clinician. Similarly, a clinician unfamiliar with deaf culture may misinterpret various nonverbal tactile and body language cues of the individual. Tactile communication, various forms of touch, and tapping behaviors may be used in deaf culture to greet others, protest, direct someone’s attention, or express emotion. Therefore, it is often recommended that assessments be conducted by someone who is both trained in the use of testing materials as well as culturally competent in deaf culture. Interpreters should be used as a last resort. 17
Conclusion
Communication assessments are both challenging and important for individuals with DWD. It can be crucial to incorporate professionals from a variety of disciplines to collaborate on the assessment. The final product should highlight the individual’s skills
and needs. A thorough assessment will incorporate a mixture of both formal and informal assessment tools, though care should be taken when adapting/modifying standardized instruments. Professionals should not only be competent with the administration
of these tools but should also be competent in understanding deaf culture. With a thorough communication assessment, professionals can deliver targeted interventions and provide higher-quality services.
Appendix A: Sample Questions from the US Office of Special Education Programs1
Expressive Communication
- How does this child make his/ her needs and wants known (body movements, gestures, facial expressions, vocalizations, words, sign language, picture symbols, object symbols, etc.)?
- Does this child’s expressive behavior appear to be intentional? Is it directed toward a goal? Does it appear that the child anticipates a response to the communication?
- How frequently does this child communicate?
- What specific messages or communicative functions does this child express (protests, requests, greetings, etc.)?
- Under what circumstances is this child most communicative (with whom? when? where?)?
- Does this child need prompting or support to communicate clearly or consistently? What type of support?
Receptive Communication
- What types of communicative behavior does this child understand (spoken words, manual signs, gestures, facial expressions, vocal intonation, picture symbols, object symbols, etc.)?
- What messages or communicative functions does this child appear to understand (directives, greetings, requests, etc.)?
- Is prompting and support needed for the child to respond to a communication?
- Who communicates effectively with this child? Are there particular activities in which the child seems most likely to respond?
Social Interaction
- Does this child enjoy interacting with adults? If yes, under what circumstances?
- Does this child enjoy interacting with peers? If yes, under what circumstances?
Hearing
- Is this child able to perceive speech, vocalizations or environmental sounds?
- Would this child benefit from hearing aids, amplification or noise reduction devices (such as an FM system)?
Vision
- Is this child able to perceive, discriminate between, and understand visually based symbols for expressive communication? If not, is a tactile expressive system indicated (e.g., object symbols, Braille)?
- Is this child able to perceive visually based symbols for receptive communication (e.g., picture symbols, sign language, print)? If not, is tactile input required (e.g., tactile signs, object symbols)?
- What accommodations are needed to help this child perceive visually based communication (positioning of child and partner, illumination, position and spacing of stimuli or symbols, size and color of symbols, etc.)?
Motor/Fine Motor Skills
- Does this child have the fine motor skills needed to use gestures or manual signs, to indicate choices or to activate expressive communication devices?
- What accommodations need to be made to allow physical access to expressive and receptive communication systems?
Preferences
- What people, things, and activities does this child prefer?
- What people, things, and activities does this child dislike?
- Is this child mostly engaged by objects or by people?
- Where and when is this child at his/her best?
- To what extent does this child tolerate direct assistance, such as hand-over-hand or hand under-hand support?
- What is this child’s primary mode of exploring new things (tactile, visual, oral)?
Temperament
- Is this child easily excited or passive and quiet?
- Does this child show sustained attention to tasks or quickly lose interest?
- Is this child calm or irritable?
- Is this child sociable or shy?
Appendix B: Sample Questions from the Perkins School for the Blind14
- How does the student demonstrate interest in and awareness of the environment?
- How does the student demonstrate recognition of familiar things in the environment?
- Is the student able to learn the names of objects in the environment?
- Is the student able to name actions in the environment?
- Does the student comment on activities that occur?
- Does the student recognize an object as a symbol of an activity?
- Does the student recognize a picture or partial object as a symbol of an activity?
- What exposure does the student have to written language (print or braille)?
- What exposure does the student have to story-time, experience books, or journal activities?
- Does the student have opportunities to write or draw in various ways?
References
- Rowland C. Assessing communication and learning in children who are deafblind or who have multiple disabilities. Design to Learn Projects, Oregon Health & Science University; 2009. https://www.designtolearn.com/uploaded/pdf/DeafBlindAssessmentGuide.pdf. Accessed June 24, 2020.
- Hogan A, Shipley M, Strazdins L, Purcell A, Baker E. Communication and behavioural disorders among children with hearing loss increases risk of mental health disorders. Aust N Z J Public Health. 2011; 35(4): 377-383.
- Gallaudet Research Institute. Regional and National Summary Report of Data from the 2009-10 Annual Survey of Deaf and Hard of Hearing Children and Youth. Washington, DC: GRI, Gallaudet University; April 2011. https://research.gallaudet.edu/Demographics/2010_National_Summary.pdf. Accessed June 24, 2020.
- Luckner JL, Bowen S. Assessment practices of professionals serving students who are deaf or hard of hearing: An initial investigation. Am Ann Deaf. 2006; 151(4): 410-417.
- Neild R, Fitzpatrick M. Overview of assessment for deaf and hard of hearing students. Psychol Schs. 2020: 57: 331-343.
- Bradham TS, Houston, KT, Diefendorf, AO. Assessing a child with hearing loss: Past, present and future. In: Bradham TS, Houston KT. Assessing Listening and Spoken Language in Children with Hearing Loss. San Diego, CA: Plural Publishing Inc; 2015: 3-18.
- Brady NC, Bruce S, Goldman A, et al. Communication Services and Supports for Individuals with Severe Disabilities: Guidance for Assessment and Intervention. Am J Intellect Dev Disabil. 2016; 121(2): 121-138.
- Mann W. Measuring deaf learners’ language progress in school. In: Knoors H, Marschark M. Evidence-Based Practices in Deaf Education. New York, NY: Oxford Scholarship Online; 171-190. doi:10.1093/oso/9780190880545.003.0008.
- Rowland C. Using the Communication Matrix to assess expressive skills in early communicators. Commun Disord Q. 2011; 32(3): 190-201.
- Taylor C. Assessment of communication in people with learning disabilities. Advances in Mental Health and Learning Disabilities. 2008 Dec; 2(4): 15-20.
- Zaidman-Zait A. Assessment of pragmatic abilities in deaf and hard of hearing learners in relation to social skills. In: Knoors H, Marschark M. Evidence-Based Practices in Deaf Education. Oxford Scholarship Online. doi:10.1093/oso/9780190880545.003.0022.
- Chadwick D, Buell S, Goldbart J. Approaches to communication assessment with children and adults with profound intellectual and multiple disabilities. J Appl Res Intellect Disabil. 2019 Mar; 32(2): 336-358.
- Boesch M. Best practices for assessing communication skills prior to preference assessments for students with severe developmental disabilities. EBP Briefs. 2014 Sep; 9(3): 1-9.
- Belote M, Collins M, Edelman S, et al. Assessment. In: Riggio M, McLetchie B. Deafblindness: Educational Services Guidelines. Watertown, MA. Perkins School for the Blind; 2008. https://www.nationaldb.org/media/doc/DESG_Final.pdf. Accessed June 24, 2020.
- Clark T. Considerations for appropriate assessments with deaf children. Raising and Educating Deaf Children. http://www.raisingandeducatingdeafchildren.org/2015/04/01/considerations-for-appropriate-assessments-with-deaf-children/. Published April 1, 2015. Accessed June 25, 2020.
- Pizzo L, Chilvers A. Assessment and d/Deaf and hard of hearing multilingual learners: Considerations and promising practices. Am Ann Deaf. 2016 Spring; 161(1): 56-66.
- Clark TA. Assessment and development of deaf children with multiple challenges. In: Knoors H, Marschark M. Evidence-Based Practices in Deaf Education. New York, NY: Oxford Scholarship Online; 33-58. doi: 10.1093/oso/9780190880545.003.0002
Biographies
Jesse Northridge is a licensed clinical social worker for Penn State Health’s Autism Division. He also provides services to the Autism Services, Education, Resources, and Training Collaborative (ASERT), a Pennsylvania initiative funded by the Office of Developmental Programs (ODP). Jesse obtained his master’s degree in social work through Temple University in 2017. He can be reached at jnorthridge@pennstatehealth.psu.edu.
Erin Edwards is a Board-Certified Behavior Analyst (BCBA) for Penn State Health’s Autism Division. She also provides services to the Autism Services, Education, Resources, and Training Collaborative (ASERT), a Pennsylvania initiative funded by the Office of Developmental Programs (ODP). She has been a practicing BCBA since 2008, working across a variety of diagnoses, setting and ages. She can be reached at eedwards@pennstatehealth.psu.edu.
Westerfield | 86-94
Volume 9 ► Issue 2 ► 2020
Utilizing Effective Communication Across Teams to Support Successful Transition into the Community
Sarah E Westerfield, Ph.D
Introduction
It is not uncommon for individuals to have a challenging time transitioning from a Residential Treatment Facility (RTF) back into the community.1 Transitions can be difficult for many reasons including, but not limited to, change in or lack of structure, decreased supervision, and inconsistencies between environments. The following case study is one example of how the difficulties of transitions can be lessened through a well-developed transition plan, frequent collaboration, and the use of multidisciplinary teams to support an individual.
Everyday Lives: Values in Action2 is the foundation for policy and principles for individuals with disabilities in Pennsylvania. The basis of Everyday Lives lies in two statements: 1) We value what is important to people with disabilities and their families, who are striving for an everyday life, and 2) People with disabilities have a right to an everyday life that is no different than that of all other citizens. As challenges arise in various situations, how do we consistently ensure quality of life for individuals no matter the diagnosis and/or behavioral concerns? Individuals with dual diagnoses and/or behavior concerns can present unique challenges and may require additional support to maintain an Everyday Life. This case study will relay the chapter in the story of Joseph (pseudonym) who is Deaf and diagnosed with autism spectrum disorder (ASD).
Research estimates that as many as 3.5% of individuals diagnosed with autism spectrum disorder (ASD) are also Deaf or hard of hearing (DHH)3 This combination of diagnoses presents unique challenges, including finding providers who are prepared to support individuals with multiple disabilities. While there is almost no systematic research on the adaptation of evidence-based practices for individuals with ASD who also have hearing loss4 we can utilize best practices for behavior intervention and collaboration across teams to create the likelihood for success. Joseph’s story illustrates a successful transition into the community after an initial failed attempt and documents the imperative need for communication and collaboration across multi-disciplinary teams.
As a teenager, Joseph’s behaviors reached a point where it was difficult for the family to care for him in the home. In order to receive specialized care to address his needs, he entered a (RTF) that supported individuals with ASD who were also Deaf or hard of hearing (DHH). An RTF provides a highly structured, therapeutic environment, where intensive treatment plans can be implemented based on an individual’s needs. Joseph lived in the RTF for several years with great overall success. As Joseph neared adulthood, plans were made for him to transition to residential habilitation in the community.
Joseph transitioned into a single-person residential home that was run by a provider who specialized in working with Deaf individuals. He lived in this home for a short amount of time before he transferred to a new home with the same provider due to destructive behaviors and noise complaints by neighbors. The new home was larger and was also occupied by another individual who was also receiving services. Over the nine months stay with this provider, Joseph had eight psychiatric/behavioral hospitalizations and numerous trips to the emergency room. He engaged in aggressive, destructive, and self-injurious behaviors, and frequently called 911 to return to the hospital where Joseph reported he “felt safe”. It was often thought that Joseph felt more comfortable in a hospital setting due to the rules and structure that were put in place, like what he was used to from his prior RTF setting. Throughout this time the provider consulted with an independent behavior specialist on the case and multiple attempts were made to implement behavior change procedures. As behavior events continued to escalate, three separate events ended in criminal charges being filed.
Eventually the provider began to feel that they were unable to continue to safely support Joseph. When being admitted to the psychiatric hospital for the eighth time, a 45-day written notice was sent to the Office of Developmental Programs (ODP), informing of the decision to terminate their contract with Joseph. At this same time, the physician at the psychiatric facility prepared to discharge Joseph. However, the provider was unwilling to take him back due to past events, as well as staff feeling unsafe working with him. The Administrative Entity (AE) and the Supports Coordinator (SC) for Joseph’s case began contacting multiple providers in search of a team that could support Deaf individuals who also have complex behavioral needs. In addition, ODP was contacted for additional support in finding a placement for Joseph.
The SC and AE for the county contacted approximately 40 different providers during this time and all declined being able to support Joseph, many citing their inability to meet the needs of someone who is Deaf with intense behavioral needs. Without a provider to discharge to, the hospital administration filed a 406 petition for involuntary placement to a state center, a state-run intermediate care facility for individuals with intellectual disabilities (ICF/ID). Even though the physician agreed that Joseph could and should be supported in the community, the petition was filed because he could no longer qualify for acute care in a psychiatric facility.
Simultaneously, ODP assembled a multidisciplinary team to divert his entry to a state facility and find him a placement where he could experience success in the community. The team included an ODP Clinical Director, ODP Deaf Services Coordinator, the SC, the AE, Joseph’s psychiatrist, the hospital physician, the hospital behavioral team, Joseph’s current behavior specialist, the old provider, and, eventually, the new provider. Members of the team talked daily and met weekly developing Joseph’s profile for potential providers to ensure that all communication and behavioral needs could be addressed. The team noted the importance of three factors that were imperative for Joseph to be successful in a new residential placement, 1) access to effective communication, 2) a solid behavior plan, and 3) a structured daily plan.
Joseph’s ability to communicate effectively with those around him was essential. In addition to his need for fluent American Sign Language (ASL), the team became aware that Joseph had damaged his hearing aid and cochlear implant during a behavioral episode following his initial transition to the community. Not only did this affect his daily communication with others, this left him without the ability to communicate with his family via phone. The provider reported these devices had not been fixed for two reasons: 1) There had not been time due to his continual hospital admissions, and 2) it was thought that if the devices were repaired, Joseph would break them again. To the team, this explanation was unacceptable, and it was felt his lack of access to these devices was a contributor to current behavioral issues. Immediate advocacy for communication access began, including collaborating with a specialist for full repairs to Joseph’s assistive technology (hearing aid and cochlear implant). An individualized communication profile was developed for Joseph through the ODP Special Populations Unit, while previous technical assistance increased capacity for the new provider to support Deaf individuals in their homes.
Next a solid behavior plan was created, which was key for successful support of an individual with behavior concerns. The team identified all variables that could affect behavior and success for Joseph. This included the gathering of detailed information from past medical records including genetic consultation, as well as collaboration with the previous, successful residential placement. Joseph’s behavior specialist worked with the team and the new provider to review past information and was readily available and on call to answer questions and/or address issues or concerns. The behavior specialist trained all staff on the specifics of the updated plan and the provider worked hand in hand with the behavior specialist to implement the plan with fidelity. Data was consistently tracked and analyzed allowing the new team to determine if the current plan was working, or to adjust as necessary.
Finally, the team felt Joseph was asking for structure like what he had and known in the RTF setting. He was asking in a way that others were not hearing or understanding, as he often stated he wanted to be in the hospital where it felt safe. In order to provide this, the team felt it was important to go “back to the basics” of routine and structure, that are foundational when supporting an individual on the autism spectrum. This meant continuing to provide Joseph with autonomy and the ability to make life choices, while helping him to integrate structure into his day. This was accomplished through creating routines for daily activities (eg, meals, sleep), establishing rules and expectations across settings, and utilizing visual schedules.
Although Joseph had an initial struggle in his first community home, it was shown that he could be successful with multidisciplinary collaboration and the creation of an individualized transition and behavior plan. While his transition to this new placement was not without challenges, there has been overall success, including no hospitalizations or calls to 911. With collaboration and team-work Joseph is now starting to experience an everyday life in his community. Certainly, providers cannot be expected to have expertise in every specialized area, but it is possible to locate specialists and build a team to successfully support an individual. This case is an excellent example that through team collaboration and dedication, an individual who was once considered unsuccessful in the community can experience success with the right supports in place.
There are three key lessons to be learned from Joseph’s transition. First, providers must recognize the importance of communication access for individuals with disabilities. True access to communication includes access to assistive technology. Removing or limiting access to assistive technology should never be a consideration, especially given it is essential to quality of life. Doing so removes the individual’s agency and ability to communicate. Second, when behavioral issues are present it is imperative that a research-based behavior support plan is created and implemented with fidelity. Critical components of implementing a behavior plan include staff training, daily data collection to inform decision making, and ongoing team member discussions. Lastly, collaboration across teams is essential. Establishing and maintaining clear communication within the multidisciplinary team developed for Joseph ensured he had a successful transition. Joseph’s story is evidence of the true benefits of collaboration for supporting an individual with disabilities.
References
- Nickerson A, Colby SA, Brooks JL, Rickert JM, & Salamone FJ Transitioning youth from residential treatment to the community: A preliminary investigation. Child Youth Care Forum. 2007; 36: 73-86.
- Beer AN, McBoyle M, Kakande E, Dar Santos RC, & Koszak FK. Autism and peripheral hearing loss: A systematic review. Int. J. Pediatr. Otorhinolaryngol. 2014; 78(1): 96-101.
- Everyday Lives: Values in Action. Pennsylvania Department of Human Services, Office of Developmental Programs. 2016.
- Hansen S & Scott J. A systematic review of the autism research with children who are deaf or hard of hearing. Communication Disorders Quarterly. 2018; 39(2): 330-334.
Biography
Sarah Westerfield started with the Division of Program Administration in January of 2020 as the Western Regional Clinical Director. She received her Ph.D. from the University of Pittsburgh and her research focuses on family-professional partnerships as well as transition to adulthood for individuals with autism. Sarah has over 15-years of experience working with individuals with disabilities and their families. Formerly she has worked in early intervention through college transition, and as a special education teacher and supervisor.
Contact Information
Sarah E. Westerfield, Ph.D.
PA Department of Human Services
Office of Developmental Programs
Western Regional Office
Suite 490 Piatt Place, 301 Fifth Avenue
Pittsburgh, PA
(412)-880-0973