Positive Approaches Journal, Volume 10, Issue 1
| Site: | My ODP |
| Course: | My ODP |
| Book: | Positive Approaches Journal, Volume 10, Issue 1 |
| Printed by: | |
| Date: | Sunday, August 9, 2026, 12:53 AM |
Positive Approaches Journal | 5

Volume 10 ► Issue 1 ► May 2021
Sexuality and Social Connectedness Part 2
Introduction
Human sexuality has long been studied and will continue to be explored for years to come. Throughout my career several things have remained constant: individuals, no matter their age (beyond adolescence), gender, race, sexual orientation, mental health status, or presence of intellectual or developmental disability all want to feel safe and develop loving relationships. The desire for intimacy is not limited to a certain fraction of the human race; we do well to remember that. Relationships are an enduring part of who we are, and they tend to connect us. The COVID-19 pandemic has stressed many of those relationships and we have had to be innovative to maintain a sense of connectiveness. Let’s continue to work on getting to know each other and developing lasting relationships. We can all use the connection!
Kate Griffin, an English author, once said:
It seems to me that the greatest triumph of any human rights movement, be it fighting for racial, religious, sexual or gender equality – is to achieve that moment where eyes are opened so wide that a sort of blindness sets in. I don’t care if
someone is black, white, gay, or straight. I don’t care if a woman has children or no – I just want to know who they are. […] At the end of the day, gender differences seem to me to be just a tiny, tiny drop in the great expanse of things
that make people unique. Unique, not ‘different’, not ‘other’ merely another piece of that great teaming mass that makes up the wonderfully rich, thrillingly varied definition of ‘humanity.'
—Dale K. Adair, MD, FAPA, Chief Psychiatric Officer, Office of the Medical Director
Department of Human Services, Office of Mental Health and Substance Abuse Services (OMHSAS)
Positive Approaches Journal | 6-7
Volume 10 ► Issue 1 ► May 2021
Data Discoveries
The goal of Data Discoveries is to present useful data using new methods and platforms that can be customized.
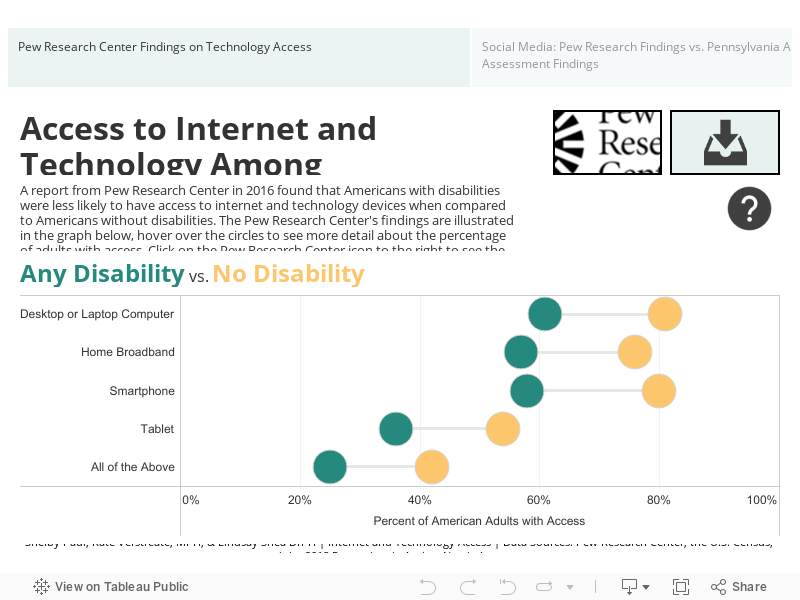
Access to Internet and Technology Among Adults with Disabilities
Access to the internet, technology devices, and social media has become a part of most of our lives, especially in the era of COVID-19 related lockdown orders. Whether we are searching the web for news or chatting with friends on Facebook, technology plays a large role in keeping us connected. This dashboard is powered by data from the Pew Research Center, Pennsylvania Autism Needs Assessment, and U.S. Census data aimed at evaluating how Americans with disabilities are accessing technology and using the internet to stay engaged in their communities and connected to others.
To navigate the dashboard below, use the buttons along the top to browse through the topics. On tabs that include filters (located just above the chart on the left-hand side), select a value to filter the data by (i.e. race, age group, gender) and the charts below will be filtered to that specific group. To see the exact values displayed in the graphs, hover over the marks on the graph and a tooltip will appear to show these values. If you would like to download the data dashboard, click the download icon in the top right corner of the dashboard. To access the websites used in developing the data dashboards, click on their respective icons located in the upper right-hand corner of the dashboard.
Having Trouble Getting Online?
Public libraries are a great way to access computers and other technology devices as well as broadband internet. To find a Pennsylvania Public Library near you, visit Public Libraries (pa.gov) and search for your county. Access to free Wifi can also be helpful if you do not have access in your own home, to find accessible hot spots near you visit Free WiFi Hotspots in United States | WiFi Map and search for your city. For more ways to get involved in the online community, visit ASD Next to browse virtual social events, get connected on social media, and access resources. As always, when we are using the internet it is important to keep ourselves and our information safe. Visit ASERT: Cyber Safety Tips and Tools to learn more about how to keep your personal information safe when browsing the internet and using social media sites.
Boyd | 8-14
Volume 10 ► Issue 1 ► May 2021
Embracing Inclusion: Prioritizing Lesbian/Gay/Bisexual/Transgender/Queer (or Questioning)/Intersex/Asexual/+ (LGBTQIA+) Inclusion for People with Intellectual and Developmental Disabilities
Parris Boyd
Abstract
This article explores the importance of LGBTQIA+ inclusion for people with intellectual and developmental disabilities. People at this intersection face unique barriers such as choosing between expressing their gender and/or sexual identity and losing life-sustaining supports. After identifying some of these barriers, the article gives readers ways to be inclusive when working with LGBTQIA+ people with disabilities.
You may have looked at the title of this article and wondered, “Where did the Q, I, A, and + come from?” What has traditionally been known as the “LGBT” community has been growing in recent years due to the understanding of what the LGBTQIA+ community means. Largely, this community has defined itself by being outside of the heterosexual lens. As more identities figure out that they are outside of that lens, they have advocated to become a part of the acronym. This has left us with the acronym LGBTQIA+ which usually translates to:
- Lesbian
- Gay
- Bisexual
- Transgender
- Queer/Questioning
- Intersex
- Asexual
- + The many sexualities that are not included in the acronym
In discussing inclusion, it’s important we are aware that people with developmental disabilities can be any, and multiple, identities within the LGBTQIA+ spectrum. For instance, a transgender woman with an intellectual disability can be a lesbian. It is especially important for those who work with people with support needs to be inclusive because supporters can often be barriers to identity in ways able-bodied people do not experience. I came across this a lot in my work in gender-affirming care (gender-related healthcare for transgender patients). When conducting intake assessments for patients who had a developmental disability, the process was often different than intake assessments with folks who had fewer formal supports. A person with few formal supports often experiences barriers like losing employment, familial estrangement, and other life-shifting consequences. These are often difficult barriers to overcome but worth it for the people who came to my office. When someone with an intellectual or developmental disability would speak with me, they would not only mention the same barriers, but they would also have additional barriers related to their supporters. These supporters can often be in control of transportation, communication, and other vital resources that people without these needs don’t have to consider. One client of mine who managed to defeat many obstacles to meet with me was still rejected when the doctor said they were not equipped to handle someone with an intellectual disability. Another client’s family said they would disown her if she even went to an appointment to talk about her gender dysphoria. Roadblocks to expression are not limited to transgender people with disabilities, many identities within the LGBTQIA+ spectrum are controlled by those around them.
In a study on resilience of LGBTQIA+ people with disabilities1, a participant detailed an experience where her parents found out that she was in a same-sex relationship and threatened to stop providing care if the relationship didn’t end. The “care” her parents were providing was life-sustaining, which forced the participant to choose between a fulfilling relationship and physical safety. This is one of countless examples of how people with higher support needs have to navigate more significant barriers. A more common example that I have been met with is supporters questioning the identity of the LQBTQIA+ person with a disability. When supporters question people about their identities, they are doing several things that they may not be aware of. For starters, they are making themselves the experts of that person’s experience. Asking people to prove their identities with questions like “Are you sure you’re a lesbian?” or “How do you know you are transgender?” instantly place the person as the student, and the asker as the expert. The truth is, by the time people express their gender or sexual identities to others, they have usually gone through a lot of internal turmoil beforehand. They likely know far more than their supporters realize. Further, these questions other the individual by treating their identity as something they have to prove to the asker. Being inclusive means that a person’s gender and/or sexual identity shouldn’t matter. The concern of the supporter should be focused on how to support them.
Supports are where LGBTQIA+ inclusion becomes most important for the well-being of a LQGBTQIA+ person with a disability- no matter the role. The Trevor Project National Survey on LGBTQ Youth Mental Health 2020 found that 29% of LGBTQ youth experienced
homelessness, were kicked out of their homes, or ran away2. This statistic shows how many LGBTQIA+ youth are facing unsupportive homes and families. This is exacerbated when it comes to LGBTQIA+ individuals who have disabilities because
running away or being kicked out could be impossible due to not physically being able to leave, having medication that is not otherwise accessible, or even death due to their reliance on supports. This leaves LGBTQIA+ individuals with disabilities
in a position where they have to choose whether to be themselves or their mental, and sometimes physical health. The word “choose” is not exactly fitting when it comes to the positions LGBTQIA+ people with disabilities are faced with around unsupportive
people. This “choice” is often between expressing gender identity, which has been noted by the CDC to lead to better health outcomes or facing hostility and even physical violence for being open about one’s sexuality and/or gender identity3.
People within the LGBTQIA+ community are very attuned to who is and is not homophobic but even still, there are risks to coming out to a person who has the best intentions. In short, there are many reasons why people may not come out and those
reasons are only amplified when individuals have higher support needs.
Another barrier that comes with being disabled and in the LGBTQIA+ community is that they are sometimes faced with even more marginalization. LGBTQIA+ people with disabilities have to deal with homophobia and/or transphobia in the disability community and ableism in the LGBTQIA+ community. This is an oversimplification as you can also face ableism within the disability community and homophobia and transphobia in the LGBTQIA+ community. To live at the intersection of these identities has been documented by many people with lived experience to be even more severe (see Hayden Kristal’s TEDX “The Importance of Intersectional Accessibility in Activism4”). This creates few, or no, places of safety for LGBTQIA+ individuals with disabilities and may force them to navigate each identity while trying to find community. This is exactly why the interactions with the people closest to them are so important. Having to navigate multiple marginalized identities to find a place of belonging takes a large toll on one’s mental health5 There are concrete ways supporters can be inclusive and therefore lifting the burden of feeling outcasted:
- When someone tells you they are gay, transgender, asexual, etc. you should believe them. Questioning how they came to know this is simply not important. A more appropriate question is, “How can I support you?”
- If someone says that they are transgender, it is important to recognize that gender is more than genitals. People express their gender in many ways that don’t include a doctor (i.e. nail polish, haircuts, clothing, etc.).
- There isn’t an IQ test related to being gay, straight, transgender, etc. People of all backgrounds and disabilities can be within the LGBTQIA+ spectrum- even if they do not have the words for it.
- Be careful with your words. Though you may think there isn’t anyone who is LGBTQIA+ around you, you never know, so it’s best to avoid derogatory comments about any identity.
- Be open to making mistakes- we all make them. If you say the wrong thing, just apologize and take it as a lesson. It’s important to remember that just because you apologize doesn’t mean they owe you forgiveness.
If we truly want an inclusive world, we have to give all people the space to be themselves (within the parameters of legality and not harming others). For too long, the answer to embracing LGBTQIA+ people with disabilities has been met with fear of teasing. This puts the onus on the individual rather than addressing the actual perpetrator of the harm- the bully, especially considering that bullying is usually not restricted to one facet of a victim’s identity. Being inclusive isn’t hard but it does require explicit effort. The effort is worth it and will pay off for people who have had their identities pushed aside for far too long.
References
1. Hunter T, Dispenza F, Huffstead M, Suttles M, Bradley Z. Queering disability: Exploring the resilience of sexual and gender minority persons living with disabilities. Rehabilitation Counseling Bulletin. 2020;64(1): 31-41. doi:10.1177/0034355219895813.
2. The Trevor project national survey 2020.” The Trevor Project website. Accessed April 25, 2021. www.thetrevorproject.org/survey-2020/?section=Suicide-Mental-Health.
3. Mental health for gay and bisexual men. Centers for Disease Control website. Published February 29, 2016. Accessed April 25, 2021. www.cdc.gov/msmhealth/mental-health.htm.
4. Kristal H. The importance of intersectional accessibility in activism. YouTube. Published June 2, 2016, Accessed April 25, 2021. www.youtube.com/watch?v=W0I9kXwxIu0
5. Conover KJ, Israel T. Microaggressions and social support among sexual minorities with physical disabilities. Rehabilitation Psych. 2019; 64(2): 167-178. doi:10.1037/rep0000250
Biography
Mr. Boyd (he/him) is a project coordinator at the Institute on Disabilities where he principally works on projects related to criminal justice and sexuality. He earned his Master’s in Social Work at Temple University. Mr. Boyd has previously worked in gender-affirming care at a medical practice and in transition for refugee populations.
Contact information
Parris Boyd
Institute on Disabilities, College of Education and Human Development at Temple University
Brown | 15-22
Volume 10 ► Issue 1 ► May 2021
Responding to the Victimization of Individuals
with Intellectual Disabilities and Autism
Sierra Brown, PhD
Abstract
People with disabilities are at risk for sexual victimization at a much higher rate than their peers. Current estimates may be underestimated due to challenges in communication and disclosing abuse. Improving sexual education and knowledge for people with disabilities can improve outcomes and reduce the risk of victimization. However, many individuals do not receive adequate sexual education. This article reviews how Autism Services, Education, Resources, and Training (ASERT) Collaborative is responding to this issue and raising awareness to decrease victimization.
Introduction
Healthy relationships and sexuality are important parts of a fulfilling, everyday life, and a right for all people with developmental disabilities. However, many people with developmental disabilities do not have the same access as others to education and knowledge essential to developing and maintaining healthy relationships – including education regarding sexual health and sexuality.1,2 People with developmental disabilities are at a disadvantage as research suggests that people with Intellectual Disabilities and Autism (ID/A) have lower levels of perceived and actual knowledge of sexuality.3 Additionally, poor sexual knowledge may increase the risk of sexual victimization. 2 Recent findings suggest that people with intellectual disability are sexually assaulted seven times more than people without disabilities. This striking statistic highlights the need and urgency to develop risk reduction strategies and improve the sexual education for people with developmental disabilities.
Sexual Education and Developmental Disabilities
Sexual education is essential to the development of healthy relationships and reducing risk of victimization. However, sexual education is not universally provided to children, adolescents, and adults who have developmental disabilities. A common belief was that people with disabilities did not desire sexual relationships, were asexual, or could not manage these types of relationships. Decades worth of research and advocacy have documented improved attitudes of families, caregivers, and professionals regarding the sexuality and sexual education of individuals with disabilities.4,5 Despite the paradigm shift, the availability to receive this type of education remains limited for individuals with disabilities for many reasons. Though attitudes have generally improved overall, the sexual development of individuals with disabilities is still often ignored. 5 Information about sexual health may be intentionally or unintentionally withheld from people with disabilities during critical moments of adolescence and adulthood for fear that the information will increase inappropriate sexual behavior, fear of victimization, the belief that the person would not have the ability or desire for a sexual relationship, or due to concerns regarding consent and their decision making ability regarding sexual activity. Students with disabilities are at times excluded from sex education at school or may not receive adequate education that is taught to their developmental level.6 If topics related to health and development are covered, information about more nuanced topics such as dating, marriage, and sexuality are typically not adequately covered.7 By the time a person reaches adulthood, there are very limited resources and opportunities for direct education. When sex education is provided it is often not tailored to the individual’s needs and is offered traditional views of sexuality from a heteronormative framework.8 Many individuals with disabilities are then left to get their relationship and sexual knowledge from unreliable sources, such as the internet, TV shows, movies, and pornography.1 These methods may perpetuate misconceptions about sexuality and do not provide adequate information about what it takes to have a healthy sexuality. Oftentimes, the responsibility of sexual education falls on parents and caregivers who may have a high degree of discomfort or uncertainty about the appropriateness of broaching topics issues related sexual health, relationships, and sexuality.4,8-11
Direct instruction of sexual education is also necessary to give people the tools necessary to recognize and prevent abuse or exploitation. Increase risk of sexual victimization is influenced by many factors including learned compliant behaviors, increased reliance on others for assistance in personal care, communication challenges, lack of awareness that certain behaviors are considered sexual abuse or exploitation, or a desire to be socially accepted. Education can be used to teach personal safety skills to recognize and disclose sexual abuse. Education can also be a powerful tool to empower people with disabilities to exercise greater autonomy over their body, life, and choices.
Best Practices in Sexual Education
When it comes to sexual education, a comprehensive range of topics should be covered to address all aspects of healthy relationships and sexuality– from personal hygiene, information about puberty, understanding anatomical information, and topics regarding sex.
Sexual education should be tailored to the person’s specific needs, with special consideration for the developmental level, communication skills, and age. Teaching sexual education should follow the best practices of education for individuals with disabilities including repetition, the use of visuals, concrete language, video modeling, and social scripts. Therefore, sex education cannot be a one-time occurrence that happens in high school. Sex education should be started from an early age and should continue through adulthood, focusing on age-relevant issues. The goals of the education should not only be aimed at risk reduction and prevention of inappropriate sexual behaviors. However, it is equally important to equip people with skills to develop meaningful relationships and sexuality and also provide them information to be able to distinguish between risky and safe behaviors.
The adequacy of sexual education may also be related to conflicts with existing policies, regulations, and laws aimed at protecting vulnerable populations. For example, results of one study showed professionals identified several topics related to sexual health that were not allowed to be taught in their organization. 12 It is a challenge to balance existing policies and procedures with the needs of individuals who benefit from direct sexual education. In Pennsylvania, this was addressed by the Sexual Health, Personal Relationships, and Sexuality Guidelines put forth by the Office of Developmental Programs (ODP)13 which state, providers are encouraged to “have a policy on sexuality that is consistent with the values of Everyday Lives…” and to “provide accessible and appropriate education, information, and resources that address sexual health, personal relationships, and sexuality needs.”
Autism Services, Education, Resources, and Training’s (ASERT) Response in Pennsylvania
In 2018, the National Public Radio (NPR) released a series called “Abused and Betrayed” investigated unpublished findings from the US Department of Justice documenting how people with intellectual disabilities were disproportionally impacted by sexual abuse. 14 Statistics provided by the Department of Justice revealed that people with disabilities were sexually assaulted seven times more than people without disabilities indicating people with disabilities. 14 The series prompted swift action from advocates and organizations to help meet the needs of individuals with disabilities to reduce the risk of victimization and to increase competency in healthy relationships.
ASERT is a state-wide initiative in Pennsylvania funded by ODP aimed at supporting individuals with autism, their families, caregivers, and professionals through providing resources, education, and training. Following the reporting by NPR, the response from ASERT began with a partnership with experts in the field to address the risk of sexual victimization for people with autism spectrum disorders (ASD). The first initiative by ASERT was in collaboration with researchers at the National Crime Victims Research and Treatment Center (NCVC) at the Medical University of South Carolina called the “Be Safe” campaign. The goal of the Be Safe resource collection was to disseminate pertinent, scientific, and developmentally relevant information to the community about prevention and intervention strategies for people with ASD. These resources were created in part to address the needs of parents, caregivers, and professionals but also aimed to empower self-advocates by providing information about healthy relationships and sexuality.
The resources developed for the Be Safe campaign were created with best practices of information dissemination in mind. To target a large variety of stakeholders, learning styles, and information preferences, ASERT adapted resources on topics related to sexual health and reducing risk in a variety of formats including resource pages, social stories, visuals, and videos. eLearning modules were also developed to provide families/caregivers, professionals, and self-advocates more in-depth information about the prevention and intervention for sexual victimization. Furthermore, to provide the community easier access to these resources these resources were then published online at ASERT’s website, www.PAAutism.org/BeSafe.
ASERT continues to develop projects with a focus on reducing risk of sexual victimization through collaboration with two organizations that support individuals with developmental disabilities in Pennsylvania: Healthcare Quality Units (HCQUs) and Temple University Institute on Disabilities as part of the Information Sharing and Advisory Committee (ISAC) sub-committee on sexual abuse prevention. The aim of this collaboration was to develop resources to increase capacity and knowledge for service providers on topics healthy relationships and risk reduction in line with ODP’s Sexual Health, Personal Relationships, and Sexuality Guidelines.
Conclusions
Healthy relationships and sexuality is a right of all people. Though a great deal of progress has been recognizing sexual health as an important aspect of an everyday life, more action is needed to develop ways to deliver sexual education and reduce the risk of victimization. Recognition of the risk factors and signs of sexual victimization, improved access to education for individuals with disabilities, and focus on best practices can help to further reduce this risk of sexual victimization for people with disabilities.
References
1. Mehzabin P, Stokes MA. Self-assessed sexuality in young adults with High-Functioning Autism. Res Autism Spectr Disord. 2011;5(1):614-621.
2. Solomon D, Pantalone DW, Faja S. Autism and adult sex education: A literature review using the information-motivation-behavioral skills framework. Sex Disabil. 2019;37(3):339-351.
3. Brown-Lavoie SM, Viecili MA, Weiss JA. Sexual knowledge and victimization in adults with autism spectrum disorders. J Autism Dev Disord. 2014;44(9):2185-2196.
4. Tamas D, Brkic Jovanovic N, Rajic M, Bugarski Ignjatovic V, Peric Prkosovacki B. Professionals, parents and the general public: Attitudes towards the sexuality of persons with intellectual disability. Sex Disabil. 2019;37(2):245-258.
5. Ballan MS. Parental perspectives of communication about sexuality in families of children with autism spectrum disorders. J Autism Dev Disord. 2012;42(5):676-684.
6. Barnard-Brak L, Schmidt M, Chesnut S, Wei T, Richman D. Predictors of access to sex education for children with intellectual disabilities in public schools. Intellect Dev Disabil. 2014;52(2):85-97.
7. Holmes LG, Himle MB, Sewell KK, Carbone PS, Strassberg DS, Murphy NA. Addressing sexuality in youth with autism spectrum disorders: Current pediatric practices and barriers. J Dev Behav Pediatr. 2014;35(3):172-178.
8. Barnett JP, Maticka-Tyndale E. Qualitative exploration of sexual experiences among adults on the autism spectrum: Implications for sex education. Perspect Sex Reprod Health. 2015;47(4):171-179.
9. Holmes LG, Strassberg DS, Himle MB. Family sexuality communication for adolescent girls on the autism spectrum. J Autism Dev Disord. 2019;49(6):2403-2416.
10. Nichols S, Blakeley-Smith A. “I’m not sure we’re ready for this …”: Working with families toward facilitating healthy sexuality for individuals with autism spectrum disorders. Soc Work Ment Health. 2009;8(1):72-91.
11. Hartmann K, Urbano MR, Raffaele CT, Qualls LR, Williams TV, Warren C, Kreiser NL, Elkins DE, Deutsch SI. Sexuality in the autism spectrum study (SASS): Reports from young adults and parents. J Autism Dev Disord. 2019;49(9):3638-3655.
12. Curtiss SL, Ebata AT. Building capacity to deliver sex education to individuals with autism. Sex Disabil. 2016;34(1):27-47.
13. Bulletin 00-18-01 attachment 1: Sexual health, personal relationships, and sexuality guidelines. Rehabilitation & Community Providers Association website. https://www.paproviders.org/wp-content/uploads/2018/04/00-18-01-Attachment-1-Sexual-Health-Personal-Relationships-and-Sexuali....pdf. Published 2018. Accessed April 16, 2021.
14. Shapiro J. Abused and Betrayed Series. NPR website. https://www.npr.org/series/575502633/abused-and-betrayed. Published January 8, 2018. Accessed April 16, 2021.
Biography
Sierra Brown is a licensed and board-certified psychologist. Dr. Brown is currently an Assistant Professor within the Department of Psychiatry, Division of Autism Services. In the Division of Autism Services, she is actively involved in research and community outreach projects through the Autism Services, Education, Resources, and Training (ASERT).
Contact Information
Sierra Brown
Assistant Professor, Department of Psychiatry, Division of Autism Services
Phone: 717-531-8338
Frantz | 23-34
Volume 10 ► Issue 1 ► May 2021
Detangling Sexuality Information: Misinformation, Confusion or Hope
Beverly L Frantz
Abstract
Sex is a difficult subject for parents, teachers, and other professionals to discuss. Sexuality conversations tend to be brief, biased based, and infrequent. Without ongoing comprehensive sexuality education, a gap between intelligence, curiosity, social messaging, and personal experiences can have significant consequences.
This paper explores how the lack of comprehensive sexuality education with an increase in the number of sexual messages from the internet and other social media platforms together with sexual behavior rules that people are required to follow in group homes or other residential settings provide confusion for people with intellectual and developmental disabilities. The confusion looks very different for an adult and is a slippery slope from non-contact sexual behavior to sexual offending behavior.
Sexuality is an integral part of who we are. It is a basic and natural human drive. It is more than just “doing it” or “having sex.” It is a constant companion throughout life. The World Health Organization (WHO) defines “sexuality” as a “central aspect of being human which encompasses sex, gender identities and roles, sexual orientation, eroticism, pleasure, intimacy and reproduction.1”
If sexuality is such an integral part of our lives, why do we have such a difficult time talking about it? Especially, with people with intellectual and developmental disabilities (IDD)? Over their lifespan, a person with IDD may need additional support to explore and understand sexuality. They want a romantic relationship. However, their parents, residential staff, or other professionals may discourage the relationship for fear they may engage in sexual intercourse.
Sources of Conflicting Sexual Messages
Remember when you were a child, how did you learn about sex? What formal or informal messages did you receive about sex? How many boyfriends or girlfriends did you have in grade school? Did the person you thought of as your boyfriend or girlfriend know? How long did the relationship last? A day, two days, a week? What about in high school? Post high school? Sexuality is not static. It is fluid. We perceive it differently as we age and experience its various forms. For example, sexuality in its broadest terms includes holding hands, kissing, snuggling, doing things together, the examples are endless.
People, including people with IDD, receive numerous sexuality messages over their lifespan. Age, culture, family beliefs, geography, education, religion/faith all contribute to the types of sex messages a person receives. People, including parents, caregivers, teachers, professionals, direct support professionals, siblings, and friends each provide different messages. The media including print, television, movies, internet, and other social platforms also supply different messages and frequently contradict each other. These contradictory messages become a tangled web of words. A web from which it is difficult to discern accurate information from misinformation and sensational information.
Regardless of any sexuality question or issue, clear and concise statements are easier to understand. People with IDD infrequently receive clear and concise statements; unless, it is to re-direct or reprimand their behavior. Everyone should have the opportunity to receive clear, accurate, and non-judgmental information about sexuality.
The Role of Parents/Care Providers in Sex Education
Parents and care providers play a significant role in their child’s sexual education and behaviors. Curiosity about sex is natural, regardless of a person’s age. If accurate sexuality education is not provided, children will learn about it from other sources. The sexuality information a child, adolescent, or adult receives from outside of the family may be misleading and inaccurate. Parents must be sensitive to what information their child, regardless of the age of the child, is seeking. Sources may present information as accurate, misleading, romanticized or a combination.
The following example illustrates how easily, from a generational perspective, it is to misunderstand sexual words and concepts.
After getting off the school bus and walking into his house a third-grade student asked his mother, “Did you and dad have oral sex this morning?” Surprised by the question and not knowing exactly how to respond, she told her son to ask his father when he came home from work. When dad came home, she told him what their son had asked. In a few years the father had planned to have the “sex talk.” But his son asked a question and he would answer it now. His son was playing a video game when dad approached him to talk. His son was focused on his game and showed no interest in what his father was trying to talk to him about.
Mom and dad heard “oral sex” from an adult perspective and were prepared to answer the question from that perspective. That is, the mechanics of oral sex. What the child was actually asking was whether his parents kissed each other that morning. How could oral sex be mistaken for kissing? Simply. A few days before the child asked, “the question,” he had a dental check-up; and, the importance of oral hygiene was discussed. The following day his buddy at school shared a secret with him. His buddy said that during recess and behind the school dumpster, he was going to have sex with his girlfriend. From a child’s perspective, kissing was synonymous with sex.
The boy was asking his mother about kissing, not oral sex. He put one (visit to dentist/oral hygiene) and one (his friend’s plan to kiss his girlfriend) together and got three (the oral sex question). Younger children are interested in body parts, pregnancy, and babies, rather than the mechanics of sex. Providing accurate, non-judgmental information to a child about their bodies, boundaries, and sexuality reduces the chance of misinformation and improves their ability to make safe and informed decisions. Accurate information acts as a safe passage to adolescence and adulthood.
Parents are their child’s first sex educator. They play a significant role in the sexual development and behavior of their child. Talking about sex, regardless of the child’s age, can be uncomfortable. At what age should parents start discussing sex with a child? How to start the conversation? What should be included in the conversation? The “sex” conversation is not a one-time conversation. It is a continuous conversation delivered in a non-judgmental, age appropriate, positive manner. There is no single, right way to talk to your child about sex. In fact, talking to your child about sex might be the easiest conversation since sex refers to the biological characteristics that define humans as male or female. Discussing the broader topics of sexual health, sexuality, and sexual rights are more challenging. Chronological and development ages and life experiences are important factors in considering when, how, and what topics to begin with.
Healthy Sexuality
The Pan American Health Organization (PAHO) and the WHO convened a number of experts together to develop working definitions of key terms when discussing sexual health with respect to body integrity, sexual safety, eroticism, gender, sexual orientation, emotional attachment, and reproduction. Four key concepts were defined: sex, sexual health, sexuality, and sexual rights. “Sex” as commonly defined generally means sexual intercourse. For the purpose of this paper, the PAHO and WHO definitions will be used. That is, “sex” refers to the biological characteristics that define humans as male or female. “Sexual health” requires a positive and respectful approach to sexuality and sexual relationships, as well as the possibility of having pleasurable and safe sexual expression, free of coercion, discrimination, and violence. For “sexual health to be attained and maintained, the sexual rights of all persons must be respected, protected and fulfilled.2”
“Sexual health” needs to be understood within social, economic, and political contexts. Sexual health includes:
- Well-being, not merely the absence of disease
- Respect, safety and freedom from discrimination and violence
- The fulfillment of certain human rights
- The relevant throughout the individual’s lifespan, not only to those in the reproductive years, but also to both young and the elderly
- Diverse sexualities and forms of sexual expression
- Critically influenced by gender norms, roles, expectations, and power dynamics
“Sexualization” often called the “shadow” side of sexuality, spans behaviors that range from harmless manipulation to violent and illegal behaviors. Behaviors may include flirting, seduction, sexual harassment, sexual abuse, and rape.
The importance of providing comprehensive sexuality education in a positive, non-judgmental manner is critical to providing an opportunity for individuals with IDD to receive accurate sexuality information, ask questions, understand the rights and responsibilities of engaging in sexual activity, and to enjoy the same everyday life as those without a disability. The numerous and conflicting formal, informal, and sexually nuanced messages a person with IDD receives through their lifespan can impact how they understand the subtle differences between platonic, romantic, and intimate relationships.
Sex Education in School
A 2014 study reported that 93% of parents supported having sex education taught in middle school and 96% of parents supported having sex education taught in high school3. Comprehensive sex education is supported by numerous prestigious health and medical organizations including the American Medical Association, the American Academy of Pediatrics, and the Society for Adolescent Health and Medicine.
Schools in Pennsylvania are not required to teach sex education4, however, they are required to provide human immunodeficiency virus (HIV) education. Primary/elementary schools are allowed to omit instruction on the sexual methods of infection transmission. Sex education programs vary widely across the 500 school districts in Pennsylvania. With the exception of sexual transmitted infections (STI) and HIV prevention education, each school district is permitted to decide if it chooses to offer sex education and what topics they want included. If a student’s school does not provide comprehensive sex education, parents can advocate or insist that comprehensive sex education be included in the student’s Individualized Educational Program (IEP).5
An IEP is a program developed to ensure that a student with an identified disability, who is attending an elementary or secondary educational institution, receives specialized and related services. Some consider the IEP to be the cornerstone of a quality education for a student with a disability. School districts that do not offer comprehensive sex education curricula, unintentionally place students with disabilities at a higher risk of sexual victimization and offending behaviors. A substantial gap exists between what a child learns at home about healthy sexuality and what they learn and experience in middle and high school. How do they reconcile students touching other students – from hugs, to holding hands and kissing, to chest bumps and towel snaps in locker rooms? Especially, if they were taught to “keep your hands to yourself?” One risk reduction strategy, cited by the Center for Disease Control (CDC), is providing comprehensive sex education to reduce victimization.
When organizations such as the American Medical Association, the American Academy of Pediatrics, the Society for Adolescent Health and Medicine and the CDC support comprehensive sex education in schools, the question needs to be asked – why isn’t comprehensive sex education part of every student’s IEP? Anecdotal reports suggest that sex education is frequently included in a student’s IEP only when the student exhibits challenging sexual behavior, such as masturbating (self-pleasuring) in class, sexualized behaviors and inappropriate sexual language directed toward teachers, staff, and other students.
Students graduate from high school and enter the workforce or a post-secondary educational institution. Curiosity, misinformation, and gaps in accurate information grow exponentially as the individual transitions from high school into adulthood. Once a student leaves school, the opportunity to obtain healthy and accurate sexuality information diminishes. A one-day training or conference workshop cannot replace the mixed messages the person has previously received. In fact, it may be more confusing.
How will lack of sex education, sexual misinformation, and stereotypes impact their employment or studies? How and who will help them navigate their new sexual landscape?
The Individual with Disabilities Education Improvement Act (IDEA) requires that by age 16 the IEP team must determine what instruction and educational experience will help the student prepare for transition from school to adult life. Person Centered Planning (PCP) is widely used to help an individual explore where they are now, how they would like their life to change and what is needed to bring about that change. Consider who has the authority to decide if there is a difference of opinion between what is important to the person and what is important for them. It is not the person with IDD. It is a person with authority, perceived or real, who will make the final decision. Parents, educators, clinical professionals, and others create barriers for the individual to live an everyday life. Their own fears, biases, misinformation, and desire to protect the individual may have the reverse effect. Safety and risk must be balanced. PCP is an excellent opportunity to introduce new or expanded sexual topics into the plan that will create a safe place to talk and learn about sexuality. 6
Self-Determination
Self-determination is the concept and principle that includes people choosing and setting their own goals, being involved in making life decisions, self-advocating, and working to reach their goals. The American Association on Intellectual and Developmental Disabilities (AAIDD) defines “Self-determination” for people with IDD as “having the same rights to, and responsibilities that accompany, self-determination as everyone else. They are entitled to opportunities, respectful support, and the authority to exert control in their lives, to direct their services, and to act on their own behalf. 7 ”
A review of the self-determination literature tells us there is a consensus on the definition and concept. What is omitted is the concept of sexuality. It is intertwined with the person’s future goals, their ability to take control of their life, developing healthy self-esteem, willingness to ask questions and seek answers, and solutions. As previously mentioned, sex is more than solo or partner genital behavior. Sex is only the first three letters of sexuality. It is one component of a much larger concept.
The adverse consequences for people with IDD who receive no or inaccurate sex education increase the risk of sexual victimization and sexual offending behaviors. There are few published studies on the relationship between comprehensive sex education, victimization and offending sexual behavior, and individuals with IDD.
The number of people with IDD who come into contact with law enforcement as victims, witnesses, or perpetrators is staggering. The victimization rate for people with IDD is anywhere from 4 to 10 times higher than the general population. The discrepancy between the 4 to 10 times is based on whether the data collected included people living in congregated residential settings.8 Alleged perpetrators, generally for sex-related offenses, are disproportionately represented in the criminal justice system.9
The difference between living independently, living with family, or living in a community residential setting directly impacts the type and number of sexual messages a person receives10. Studies have suggested that the turnover rate in group home settings varies between 50% and 85% per year. Sheryl A. Laron, in her book Staff Recruitment, Retention, & Training Strategies For Community Human Services Organizations, reported that 41% of direct support workers left their jobs before finishing six months on the job, and another 25% left before finishing 12 months on the job.11 The number of agency staff and other professionals involved with supporting someone living in a group home could be 50 or more a year. Each of those individuals may express their personal views about sexuality to the people they support. A 2018 study conducted with 23 Applied Behavior Analysis (ABA) providers explored staff retention. The study found that the rate of pay and hours of supervisions were correlated with decreased turnover. Hence, the decrease in staff turnover should limit the number of mixed messages, especially around sexuality.12
Because of staff turnover, it is not practical to attempt to train all staff about sexuality and how to effectively convey accurate sexuality information to people with IDD. Instead, several staff who have shown an interest in sex education, are open to receiving on-going comprehensive sex education, are non-judgmental, respectful of other’s self-identifies and willing to work with professionally trained sex educators should be designated as the agency’s “sex educator” for the residents and staff.
Conclusion
By the time an adult individual moves from their familial home to independent living, a group home, or other residential setting they should have a strong foundation in comprehensive sex education. It is essential to begin to introduce comprehensive sex education at an early age. Lack of such education can create a dangerous gap in understanding the consequences of misinterpretation of sexual nuances and misinformation.
Sex education provides an opportunity for people with IDD to enjoy the same sexual rights and responsibilities as the general population. It can also reduce the risk of sexual victimization and prevent individuals from being charged with sexual offenses.
There is a road map for providing accurate sexual information. It starts with parents and caregivers providing short, positive, age appropriate conversations about the human body, boundaries, and saying “no.” It continues in the educational system
with IEP, PCP, and Self-Determination. Each of these domains should provide an opportunity for students to receive comprehensive sex education. The road map becomes more challenging when a person transitions from high school to adulthood. How
is accurate, non-judgmental, and sex positive information provided? What are the consequences if not provided? Who monitors the information being provided? To embrace human sexuality in the lives of people with IDD the preceding questions need
to be answered. In addition, we must understand and affirm that people with IDD are sexual beings and have the same sexual rights, responsibilities, and risks that people without IDD have.
References
1. Sexual and Reproductive Health and Research including the Special Programme HRP. Geneva, Switzerland: World Health Organization; 2011. 1-4.
2. Promotion of Sexual Health Recommendations for Action. Antigua Guatemala, Guatemala: Pan American Health Organization; 2000. 3-4.
3. What’s the State of Sex Education in the U.S.? http://www.plannedparenthood.org/learn/for-educators/whats-state-sex-education-us Published 2021. Accessed March 18, 2012
4. Schools in Pennsylvania are not required to teach sex education (Pennsylvania Consolidated Statutes Title 22§4.29 http://www.pacodeand bulletin.gov/Display/pacode?).
5. IDEA & IEPs. National Parent Center on Transition and Employment. https://www.pacer.org/transition/learning-centered/planning/idea-ieps.asp. Assessed March 22, 2021.
6. Pennsylvania State Dept. of Welfare. (1993). Finding a Way toward Everyday Lives: The Contribution of Person-Centered Planning (H133B80048). Harrisburg, Pennsylvania: Office of Developmental Disabilities.
7. Self-determination. Joint Position Statement of the AAIDD & The Arc. AAIDD Website. https://www.aaidd.org/news-policy/policy/position-statements/self-determination. Published February 14, 2018. Accessed March 24, 2021
8. Sobsey, D. Violence and Abuse in the Lives of People with Disabilities: The End of Silence Acceptance. Baltimore, MD: Paul H Brookes; 1994, 64-75.
9. Bronson J, Maruschak LM, Berzofsky M. Disabilities Among Prison and Jail Inmates, 2011-12. Washington DC: US Department of Justice; 2015.
10. May DC; Kundert DK. Are Special Educators Prepared to Meet the Sex Education Needs of Their Students? A Progress Report. J. Spec. Educ., 1996-01 Vol 29(4) 433-444.
11. Larson SA, Hewitt, AS. Staff Recruitment, Retention, & Training Strategies for Community Human Services Organizations. Baltimore, MD: Paul H Brookes; 2005.
12. Thornton, C.R. (2018) Direct Support Staff Retention and Turnover in the Field of Applied Behavior Analysis: A National Survey (Unpublished thesis). Temple University, Philadelphia, Pa
Biographies:
Dr. Frantz directs the Institute on Disabilities at Temple University’s criminal justice and sexuality initiatives, including curriculum development, training, and technical assistance at local, state, and national levels. Her area on concentration is the intersection of disabilities, healthy sexuality, sexual violence, and the criminal justice system. She has produced numerous training videos for first responders, family members, victims, and disability service professionals. She authored personal safety curricula, peer reviewed journal articles, book chapters, DVD, and tip sheets. Dr. Frantz was the subject matter consultant for ESPN-60 program on the sexual abuse of athletes with intellectual disabilities. She is a guest faculty member for Aequitas: The National Prosecutors’ Resource on Violence Against Women, and adjunct assistant professor at Temple University. Dr. Frantz earned Master of Science degrees from Villanova University and the London School of Economics and a Doctorate degree from Widener University with a focus in Human Sexuality.
Contact Information
Beverly L Frantz
Project Director, Criminal Justice and Healthy Sexuality Initiatives
Institute on Disabilities, Temple University
215-204-5078
Hipple,Tennille, & Bohrman | 35-44
Volume 10 ► Issue 1 ► May 2021
Approaching Sexuality
in Service Spaces: An Invitation to Deeper Inquiry
Erin Hipple, Julie Tennille, and Casey Bohrman
Abstract
This article is focused on the complexities of human sexuality and gender identity and couched in vulnerability, inviting readers to reflection. Three academics, one of which continues in practice, present their musings, missteps, and a brief case presentation with a client from a subset of Bondage Discipline Dominance and Submission (BDSM). We conclude with provocative questions for reflection and suggestions for future action and consideration.
___
This article is a love letter to our past, present, and future clients, to our communities of helping professionals, to one another, and to ourselves. It blends musings born of lived experience and remembered missteps, and provides a brief case study presentation to consider, from the perspective of three academics who are eager to see a more robust integration of addressing sexuality and gender in treatment spaces. We reject the notion that behavioral health providers (social workers, psychologists, medical professionals, and the like) can ever assert “expertise” on a topic so complex. We created this writing to offer reflection on our vulnerabilities as clinicians, educators, and humans. We invite you to be vulnerable as well, insofar as it feels resonant to do so.
As a result of the lack of comprehensive sexual literacy at all levels of education, behavioral health providers and clients alike might struggle to bring up issues of sex. Regardless of their level of comfort with sexuality, these providers may find themselves as a first point of contact for clients arriving for other concerns irrespective of or secondary to their sexuality. A lack of understanding of sexuality concepts may make even unrelated therapeutic work more difficult. Also, depending on a variety of factors including location and socioeconomic class, clients may not have the option of a referral to someone who specializes in sexuality issues, which makes basic skills related to conversing about sexuality even more necessary among providers.
We must enter into these conversations willing to make mistakes. For example, five years ago, the second and third authors were invited to deliver a training on Motivational Interviewing (MI) for persons identifying as transactivists tasked with reaching into their community to encourage the use of Pre-exposure Prophylaxis (PrEP) for prevention of HIV infection. We identified as trainers and scholars who thought a lot about heteronormativity, one of us identifying as a member of the Lesbian Gay Bisexual Transexual Questioning+ (LGBTQ+) community. We still made mistakes. The most harmful of which was misgendering individuals identifying as non-binary, accidentally using the wrong pronouns at different points throughout the 2-day training. We learned the importance of humbly apologizing, moving forward, and making concerted efforts to get pronouns correct in the future.
Brief Case Study Presentation
Early in the first author’s career, I worked with an individual whom I will call Kai. When they first came for an intake, they were struggling with relationship issues with their partner related to an infidelity that had occurred. As Kai and I explored their experiences of distrust related to the infidelity, they began talking about some of the dynamics of their relationship. Based on what they shared with me, it sounded as if their partner, a cisgender man who worked in a corporate job, was very controlling of them. Kai talked about how their partner controlled the finances, told Kai what to wear each day, and made most of the major decisions of the household.
Kai was very satisfied with these elements of the relationship and was clear and consistent in expressing that their main reason for therapy was to process the infidelity. However, I remember sitting with feelings of worry and frustration. My prior training in domestic violence was influencing my view of this situation. I spent a lot of time with this client processing their ambivalence about the relationship, expecting that at some point they would realize that the relationship was abusive. It had never occurred to me that my assessment skills were limited to my educational and professional experience/orientation thus far and my client was not, in fact, in an abusive relationship.
It wasn’t until a year into my relationship with this client that they disclosed that they and their partner were in a caregiver/little (CG/l) relationship. A CG/l relationship is a subset of Bondage and Discipline, Dominance and Submission, Sadism, and Masochism (BDSM) that involves age play. BDSM and age play can exist across a variety of genders and sexual orientations, can be sexual, non-sexual, or some combination therein. A ‘Little’ can identify themselves as a toddler, child, or teenager, and within the CG/l relationship, the Little might behave in a way akin to regression, with behaviors potentially associated with their identified ‘age.’ This is sometimes referred to as accessing ‘Little Space.’ This should be differentiated from pedophilic fantasy in that the satisfaction is not derived from the fantasy of an adult having a sexual relationship with a child, but rather the Caregiver is helping to hold a co-created space for the Little to express themselves freely, to allow them to access innocence and curiosity. Additionally, sexual activity does not generally happen when the Little is in Little Space.
Age play also differentiates from incest fantasy in that for individuals who assume these roles, the satisfaction comes from the sense of being able to nurture or provide nurturance, not the idea of fantasy related to biological relation. This is
evident in the terms used. For example, the submissive person might be called the ‘little’ or ‘girl/boy,’ not ‘child/daughter/son.’ In conjunction with this, the ‘caregiver’ or ‘daddy/mommy’ may play a variety of roles as well. In the case of
Kai and their partner, Kai’s partner saw the ‘daddy’ role as that of a protector, teacher, disciplinarian, and nurturing support. Kai and their partner used the language of Daddy Dom/little (DD/l). As with any client-centered care, it always makes
sense to allow the person in the relationship to tell you the language that they want you to use for it.
There is limited research about this style of relationship, and yet, many who are in CG/l and other iterations of BDSM relationships report experiencing safety, healing, opportunities for exploration, among other therapeutic benefits.1,2,3 Despite the reported strengths of CG/l relationships, many clients I have worked with have experienced stigmatization by behavioral health providers toward the practice of CG/l and other BDSM relationships. Individuals who are open about age play
in online forums are often labeled by people outside their community as deviant. They experience stigmatization from outsiders despite their ability to demonstrate highly nuanced and reflexive responses to questions about their sexuality. Many
individuals in age play and other BDSM-related communities also show high levels of emotional literacy and clear understanding and communication of boundaries and consent—often more so than the general population.
Shifting Perspectives and Reflection
Providers can already be quick to pathologize client sexual practices, and this is especially so when an individual has identified that they experienced sexual trauma. Providers often do this without considering the strengths and benefits of sexuality in client healing. Rather than assuming that sexual practices are pathologically derived of trauma, a powerful shift in perspective is to consider how sexual practices are actually healing.
One of the ways we can reduce the likelihood of unintentionally harming clients when discussing issues of intimacy and sexuality is to be self-reflective. We would propose that while we should be asking our clients to reflect on their experiences of sex and sexuality, we must also turn inward and reflect on our sexual landscape and how it was shaped. I would invite my fellow clinicians and anyone reading this to consider the following reflection questions as a gateway to greater comfort when talking about sexuality in therapy spaces:
1. Where did I learn about sex? What messages did I receive about it growing up and from whom? What sensation-based and emotional language best describes my reaction when I think or talk about sex? What is happening in my body as I consider a
reflection question about it now?
2. Have my sexual practices or orientation changed over time? If so, how have they changed? What factors might have been associated with the ways that my sexual practices have changed or have stayed the same?
3. How did my training/education address the topic of sex and intimacy?
4.What messages did I get about masturbation? About BDSM and other non-traditional sex practices? About polyamory? Where did these messages come from? How might my understanding of these things influence the way I address them in my clinical practice?
Conclusion and Recommendations
If you have done your self-exploration and are hoping to feel more comfortable and confident in broaching topics related to intimacy and sexuality with clients, the second and third authors have developed a MI infused training toolkit for having conversations about sexuality and intimacy that may be a helpful resource.4 MI prizes empathy and non-judgement and suggests microskills of asking open-ended questions, providing affirmations, reflections, and summaries to create space for clients to share their lived experience. For example, in the above case study, open-ended questions could be used to find out: What would an ideal intimate relationship look like for you? What are the parts of your relationship that you most enjoy and where, if at all, would you like to make changes? The use of affirmations may inspire your clients via your work of pointing out strengths rather than labeling and pathologizing. We cannot overstate how crucial affirmations can be when done genuinely and specifically. For example, just letting clients know you appreciate their willingness to share information about their relationships or affirming the importance BDSM plays in their relationships, can demonstrate non-judgement while showing clients you consistently see their strengths.
Reflections and summaries of what a client has expressed demonstrate that you are deeply listening to the information clients are sharing. A wonderful byproduct of this more mindful way of interacting is that it relieves the pressure from the behavioral health provider to achieve the unrealistic standard of being an objective expert. Instead the focus is on seeing the client as the expert in their own lives, learning how they see their situations. There is a fine balance between asking clients to educate us about their lives and experiences and asking them to educate us about topics such as BDSM. If topics emerge in these conversations that you are unfamiliar with, there are plenty of outside training opportunities on these topics.
The “righting-reflex,” a concept in MI that refers to our natural instinct to correct, give advice without permission, direct, provide warnings when we perceive danger, is one of the quickest ways to signal that you uncomfortable with the topics of sexuality, intimacy, and gender. Without intending to, this reflexive impulse can wall off significant domains of your clients’ lives (not just sexuality).
We suggest a ‘yes, and’ approach to helping clients heal with cultural sensitivity to their sexualities. Reflective work does not have an end point. It can (and sometimes must) happen in parallel with skill building and education. In the spirit of trusting the client’s wisdom in therapy space, we trust your wisdom with regard to an assessment of where your edges are and how you might move beyond them. For some, the temptation to jump to education in lieu of self-reflection might arise. For others, it might feel tempting to remain in self-reflection without seeking education. We encourage the reader to have a willingness to turn your attention to your own processes with a curiosity and willingness to reckon with where your stuck points might be, as well as look to the leadership of those with lived experience rather than relying on the limited lens of mainstream clinical training alone.
References
1. Ortmann DM, Sprott RA. Sexual Outsiders: Understanding BDSM Sexualities and Communities. Rowman & Littlefield Publishers, 2012.
2. Rulof P. Ageplay: From Diapers to Diplomas. The Nazca Plains Corporation, 2011.
3.
Tiidenberg K, Paasonen S. Littles: affects and aesthetics in sexual age-play. Sexuality
& Culture. 2019;23(2): 375-393.
4. Tennille J, Bohrman C. Conversations about intimacy and sexuality: A training toolkit using motivational interviewing. Temple University Collaborative on Community Inclusion for Individuals with Psychiatric Disabilities
website. http://www.tucollaborative.org/sdm_downloads/sexuality-and-intimacy-toolkit/
Biographies
Erin Hipple, MSW, MA, LCSW, Doctoral Candidate is an Assistant Professor at West Chester University and a trans, queer, polyam, and kink affirming trauma therapist. They use liberation-based, healing-centered frameworks in their teaching, therapy, and activism to help people think creatively, center joy + pleasure, anchor into their inner wisdom, and connect with each other in movement toward justice. Their current research examines activism, self + community care practices, and how these practices interact with larger systems of social service provision.
Julie Tennille, MSW, PhD, LSW, is an Associate Professor in the Graduate Social Work Department at West Chester University. Julie is Principal Investigator and Project Director on a Health Resources Service Administration Behavioral Health Workforce Education
and Training grant focused on Integrated Care in medically underserved communities, a member of the Motivational Interviewing Network of Trainers (MINT) and conducts research on the role of intimacy and sexuality in mental health recovery.
Casey Bohrman, MSW, PhD, LSW, Associate Professor in the Graduate Social Work Department at West Chester University. Casey is a member of the Motivational Interviewing Network of Trainers (MINT). Casey has worked in various areas of the mental health system from residential settings, to case management, to mobile crisis. Her areas of scholarship focus on recovery, harm reduction, structural violence and carceral abolition.
Contact Information
Dr. Julie Tennille
West Chester University of Pennsylvania
Graduate Social Work Department
267-968-317
Moore | 45-50
Volume 10 ► Issue 1 ► May 2021
Building a Socially
Fulfilling Life with a Mental Health Diagnosis: A Firsthand Perspective
Joan Moore
Introduction
For a long time, it was difficult for me to find fulfillment from my social life. It took a lot of work, and I continue working hard to maintain that sense of fulfillment. Professionals gave me a lot of advice on how to achieve this, but the process was very much my own. Sometimes the best path for me was not the path that was recommended. In comparing my experience with other people I've helped, both in my professional role as a Certified Peer Specialist (CPS), and in my personal life, I've noticed that each person has had a unique approach to building a social network they feel good about. People have different social needs, and different ideas of what constitutes social connectedness. Having a mental illness can pose unique social challenges. In this article I will discuss my own personal experience in overcoming these challenges, and the observations I have made throughout the process.
___
My Path to Social
Connectedness
I have been learning how to communicate my entire life. Communication is a crucial part of human existence, yet also a major source of frustration for many people. I've always found it interesting that something so fundamental to human life is not necessarily something that comes easily.
I never would have described myself as having poor communication skills, but I often felt mis-understood, which caused me to feel segregated from other people. I began experiencing this feeling of segregation as early as grade school. My relationships with my friends and family were often turbulent, and I felt as though I didn't belong. I believe mental illness played a large role in the feelings of segregation I experienced.
There were some aspects of my social life which were directly impacted by my mental illness. My illness caused severe mood swings, and I was unable to manage my emotions. My explosive displays of emotion made the people around me feel uncomfortable, or afraid. My situation was further aggravated by a personality disorder, in which passive aggressive behavior was my standard response to conflict. This created a huge barrier to my ability to have and maintain a healthy social life, and it was one of the hardest barriers for me to overcome.
For some people, even the treatment process can pose barriers. To effectively manage my mental illness, I had to undergo multiple inpatient stays, and intensive outpatient treatment. Mental health professionals often told me that it would be better for me to avoid making too many friends in the mental health system. There was concern that two recovering individuals might have a negative impact on each other, especially if one was to have a relapse or experience a personal crisis. When an individual is involved in such extensive treatment, there is not a lot of opportunity to meet people outside of the mental health system. For some individuals, the limited ability to meet people outside of the mental health system when one is so deeply embedded in the mental health system can definitely be a barrier.
There have been instances where I felt negatively influenced by another individual in recovery, however, the negative instances have been outweighed by the positive relationships I have experienced. These relationships have been very important to my continued recovery. In the same way that negative can feed off negative, positive can feed off positive. Discouraging people with significant mental illness from being friends with one another might not be the best approach for everyone. I believe that humans are complex and have diverse needs in all aspects of recovery. Some people may benefit from developing better and broader communication and relationship skills instead.
Even though some of the peers in my support system were dealing with significant problems, the relationships were invaluable to me in multiple ways. Being able to help my peers in their recovery process has been a crucial part of my own recovery. Supporting others helped me find meaning in what I had gone through myself. People felt comfortable asking me for help because of my personal experience and watching me move forward in my recovery helped my peers see possibilities for their own lives.
Whether through my work as a Certified Peer Specialist (CPS), as a friend, or as a community member, helping other people manage their mental health has been a huge part of my life. One thing I frequently share with my peers is the thought process I experienced after receiving a diagnosis. In those early years, I believed that I was incapable of getting better, and that I would never be able to manage my emotions outside of an institutional setting. I remember one day, while feeling hopeless in a psychiatric unit, I started wondering: "Why can't I get better? What am I doing wrong?" I knew that people kept telling me I needed to do more to help myself, but I was going to therapy, and completing the homework. I didn't know any other way to help myself. I was feeling bored in my hospital bed, so I asked for a book at the nurse's station. They gave me a cognitive behavioral therapy book for teenagers, and I read it front to back. I became really interested in the idea that I could control my own emotions by changing my thoughts. This was really one of the most important steps early in my recovery. I spent the next few years learning and practicing the skills I obtained in cognitive therapy and dialectical behavior therapy.
After learning healthy and effective interpersonal skills, I realized that my recovery was suddenly moving much faster. Amazingly, finding a better way to interact with other people seemed to be a necessary first step that I had to complete before I could move on with my recovery. This was a life changing realization for me. It became easier for me to manage conflict after learning better communication skills, and rationalization. Rationalization was an important skill I learned from cognitive behavior therapy, and it helped me learn how to challenge the way I thought about things. This made a huge difference in the way I was able to process my interactions with other people. These skills helped me feel less misunderstood and gave me the ability to be assertive about my wants and needs. Once I no longer had to deal with the constant ups and downs of tumultuous relationships, I was able to really focus on getting my other symptoms under control.
Learning better communication skills was an extremely important step, but I still had more work to do. Despite having the skills, I still felt a lack of fulfillment in my social life. I realized some important things at this point. I still had preconceived notions of what a healthy social life was supposed to look like, and I was uncomfortable with the idea of being alone. After some extensive reflection, I realized that I was depending on other people to make me feel happy. This was an impossible expectation because I could not control the behaviors of other people. I had recently started attending college and decided that it would be a good idea for me to get a fresh start in a new town where I didn’t know anyone. This was very scary for me since I had always depended on companionship for my happiness. I realized that the extreme emotional responses I was having to other people’s actions was limiting my ability to progress further in my recovery. This is when I decided that moving somewhere new might be my best option. I wasn't totally cutting myself off from supports but was instead simply gaining some distance.
After moving, my life changed. I became fully engaged in my education, and I was enjoying myself. Even though I had not made many close friends in college, I interacted with a lot of people. I started becoming more confident and found enjoyment in hobbies such as painting and electronics repair. After some time, I realized that I actually enjoyed my alone time a lot. Instead of craving more time with people, I started craving more time by myself. I had finally managed to become comfortable with myself. It wasn't until I reached this point that I felt true fulfillment and social connectedness. In the past, my desperation for human interaction had taken over my ability to maintain healthy boundaries. Finding happiness in solitude is what brought me out of toxic relationships and helped me strengthen the relationships I had with my support network. I was no longer overwhelming my supports with my need for constant companionship.
To this day, I am still learning and improving my communication and socialization skills. I use the knowledge and experience I have gained to help my peers, and I learn from my peers as well. Many people have stories about finding social connectedness, and first-hand testimonies can provide important information to both professionals, and other peers. I believe there is a lot to be gained from peers and professionals sharing stories, knowledge, and working together. We can learn from each other and find new ways to help individuals in recovery learn to thrive in all aspects of their lives.
Biography
I am an individual who has been living with a significant mental illness since childhood. Through years of hard work, I was able to take control of my symptoms, and build a life that I am happy with. I now work as a certified peer support specialist at Unity Family Services in Kittanning, PA. Prior to this I worked for the National Alliance on Mental Illness through the Armstrong/Indiana County Consumer and Family Satisfaction Team for several years. Outside of these professional roles, I have also spent a lot of time helping other individuals with mental illness find ways to manage their symptoms and take back control over their lives.
Contact Information
Joan Moore
724-548-8601
Murray & Northridge | 51-61
Volume 10 ► Issue 1 ► May 2021
Social Skills for the “Real World”:
Lessons
Learned from the Autism Services, Education, Resources and Training (ASERT)
Social Skills Groups
Michael
J Murray, MD and Jesse Northridge, LCSW
Abstract
Social skills challenges are one of the core deficits associated with autism spectrum disorder (ASD) and have been consistently identified as an area of high need on the ASERT Needs Assessment. This article reviews important components of effective social skills intervention to help staff intervene and address identified challenges for those with ASD. The ASERT Social Skills Programs are discussed including some of the findings from the adult program. The article concludes with a “Top 10 Tips” list to consider when planning social skills interventions.
Social connectedness is an important factor in overall health and wellness. The COVID-19 pandemic has revealed the wide health disparities in our country and the enhanced vulnerability from poorly integrated social networks that many individuals with Intellectual and Developmental Disabilities (IDD) experience. This article reviews the structural and functional components of strong social networks, including a review of different types of social capital. Suggestions for evaluating and strengthening social networks according to an individual’s expressed goals are offered.
___
The 2011 Pennsylvania Autism Needs Assessment conducted by ASERT found social skills training as among the most commonly reported unmet core need across the lifespan.1 The updated 2018 Pennsylvania Autism Needs Assessment conducted by ASERT revealed an ongoing need for social skills training access, and found that only 43% of individuals spend some time with friends. Time spent with friends varied from a high of 6.8 hours per week for those 0-5 years old to a low of 3.9 hours per week for those 31-35 years old.2
Social skills differences are the core challenge for ASD. Differences with fluently decoding social information and executing appropriate responses can become more impairing as individuals with ASD age given the increase in demands of social interactions and the increasing expectation of mastery of these skills. Adolescents are particularly vulnerable to struggle with social connectedness with peers as their social environment rapidly changes with increased emphasis on social communication (both verbal and non-verbal). Despite these needs, there is little empirical evidence for best practices for improving social interaction skills for adolescents and adults with ASD.3
In recognition of the high need for improving service access and to establish treatment efficacy, ASERT developed manualized social skills interventions for adolescents (ages 13-18) and for young adults (ages 18-30). A literature review found a significant improvement in targeted social skills in 62.5% of studies with adolescents and young adults with ASD that utilized modeling, scripting, direct instruction, prompting, and role play as social skills interventions.4 In order to capitalize on these findings, the ASERT social skills groups employed direct instruction utilizing video modeling (both prepared and self-modeling) paired with peer generalization during naturalistic social activities. Outcomes included self-report, caregiver-report, and behavioral observations.
Video modeling is helpful in that it provides a visual representation of the skill in context to a situation. In other words, the discussion expands to not just talking about “how” to greet someone but also “when” and “why.” Verbal and non-verbal communication strategies can be highlighted. A variety of models can be presented demonstrating varying degrees of proficiency (e.g. some examples demonstrating skills done well and some examples where there could be improvement). These variations help the individual gain a deeper understanding of the mechanics of the interaction/social skills. Furthermore, demonstrating alternative skills based on different hierarchies/social roles (e.g. greeting your boss vs. greeting your uncle) and degree of familiarity (e.g. the more structured greeting for someone you are initially meeting vs the typically informal greeting for someone you know well) in the different examples helps develop mastery. Periodically obtaining and viewing self-models where participants watch videos of themselves executing different skills can lead to greater insight and self-monitoring.
Peer generalization not only provides “real-world” practice, it helps promote generalization of skills which can be a significant barrier to social skills intervention.5,6 Additionally, peer generalization allows for greater social validity
of instruction and targeted skills as peers can provide additional feedback to participants regarding the evolution of skills and social expectations. An example of this is the use of popular slang terms and idioms among the peer group.
Finally, targeted skills should match the participant’s goals. The ASERT social skills groups were aimed at individuals who desired more friendships and/or to feel more comfortable in social situations. All were able to use spoken language to maintain
conversations with others. This curriculum focused on verbal and non-verbal social conversation skills. This curriculum would not be appropriate for someone who communicated differently or whose goals were different such as learning to cope better
with sensory hypersensitivities in social interactions. Furthermore, outcome measures should reflect these goals. As improved non-verbal social communication was one of the things targeted in the pilot study of this intervention, amount of eye contact
in a 5-minute interaction with a novel peer was tracked as an outcome measure. As shown in Figure 1, the amount of eye contact—shown in green—did statistically and significantly improve (p=.002) for the 29 study participants from pre-intervention
(average of 144 seconds) to post-intervention (average of 177 seconds) to 3-month follow-up (average of 186 seconds).
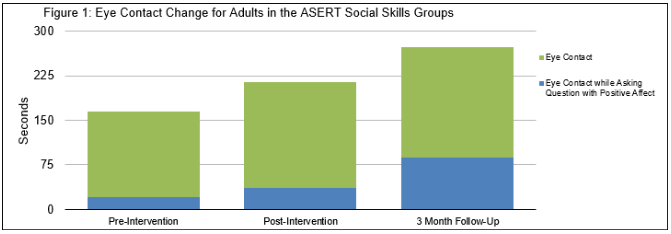
However, when thinking of communication and social impact, eye contact is even more important when you are asking a question during
a social interaction. Furthermore, doing so while having a positive affect (smiling or conveying interest) is even more impactful as it lets the other person know there is interest in their response. This reflects the “when” and “why” of social skills
mentioned previously. This high-impact eye contact—shown in blue—also demonstrated statistically and significant (p=<.001) growth across the three 5-minute observation periods. Preintervention the study participants averaged 21 seconds of
this high-impact communication. This increased to an average of 37 seconds and, perhaps most encouraging, this increased to an average of 87 seconds at the 3-month follow-up observation. These findings demonstrate that there was substantial growth
in this skill following their participation in the group and indicate successful generalization of skills.
Though this data requires a lot of time and effort to collect and analyze, its principles can be applied to clinical practice. For instance, if an individual has identified improving their ability to maintain social conversations as a goal, measuring
the length of conversation with peers would provide some feedback on progress—the “how.” However, working through the “when” and “why” of this goal with the individual may reveal hopes to use this skill to develop more friendships. In that situation,
a more nuanced— “high-impact”—way of measuring progress might be determined which would not take a lot of extra effort. Progress and success could be measured through the length of dialogue and number of open-ended questions the individual asked peers.
Increasing both conversation duration and the number of asked open-ended questions may effectively convey interest in the other person. Similarly, increasing conversation duration but declining number of asked questions may provide the individual
with valuable information as to what may be going wrong in their attempts at establishing friendships.
The following are suggestions for enhancing the impact of social skills interventions. While they are based on the experience of the ASERT team conducting social skills groups for adolescents and adults with ASD, most—if not all—of them are generalizable
to other social skills challenges not related to ASD.
Top 10 Tips for Leading an Effective Social Skills Group
1.
Break it down. Break it down. Break it down.
a. Social interactions are incredibly complex. There are hundreds of muscles throughout the body and over forty in the face. Subtle movements in these muscles can communicate important details in the course of a conversation. For example, Guillaume Duchenne documented how two facial muscles, the zygomatic major muscle and the orbicularis oculi muscle, work together to communicate genuine joy and amusement.7 When these muscles are not engaged, others have a propensity to view it as simply a “polite” smile. For an individual on the autism spectrum, recognizing these subtleties can be a Herculean task. When trying to help someone learn or improve social skills, it is frequently necessary to break down skills and concepts into smaller components. Individuals can then be instructed how to interpret situations based on which social cues are present.
2. Emphasize a take-away point.
a. For many individuals on the spectrum, there can be too much information to absorb within the timeframe of a group therapy session. For individuals who have difficulty in this type of learning environment, identifying a key message or concept for them to remember can be helpful for content retention. This concept should be reviewed several times throughout the session in order to promote learning through repetition. Even if other information is forgotten, emphasizing a take-away point can help increase the likelihood that key concepts are remembered and practiced.
3. Include more socially proficient peers.
a. There is a sizable difference between awareness of a skill and being able to use it effectively. The appropriate application and generalization of social skills can be incredibly challenging for individuals with autism. When groups are limited to others with social challenges, individuals may not recognize how the use or misuse of skills would impact social interactions outside of the group. The addition of more socially proficient peers for the purposes of practice and generalization can be highly impactful. Furthermore, many group participants have self-reported that opportunity to practice with peers is highly valuable and appealing.
4. Manipulate dyads.
a. When including peers and planning activities for social skills practice, consider how personalities and skill levels can be manipulated for growth. For example, pairing individuals who are both naturally shy could potentially motivate one of them to become more active in the interaction. Encouraging someone with significant social deficits to work with someone with strong interpersonal and leadership skills can be a great way of helping to further develop social communication skills. All dyads will have benefits and drawbacks. Be mindful of these dynamics and consider how you can manipulate them to promote skill development.
5. Allow individuals to critique their own interactions.
a. Upon viewing a recording of their social interactions, most individuals invariably notice aspects about their verbal and non-verbal communication they were unaware of in the moment. For example, some may recognize the overuse of verbal commentary or that they have a highly rigid body posture. Because social interactions are so complex, it can be difficult for individuals—particularly individuals with autism— to recognize all of the cues present in a situation. They also may not recognize how their own non-verbal cues are influencing the interaction. Although few individuals enjoy scrutinizing videotaped recordings of themselves, these recordings provide great opportunities to gain insight into skill strengths and needs. Depending on the skills being targeted, it may be beneficial to construct situations where these skills are needed. For example, individuals learning about effective interview skills could be videotaped during a mock interview. After the recording is complete, group leaders can help the individual to identify social cues present in the interaction as well as review which skills were used effectively/ineffectively.
6. Get everyone involved.
a. Many individuals who participate in social skills groups prefer discussion-style format, but this style of instruction can present challenges. Some group members may become overly passive and others may try to dominate the conversation. However, over-direction questions to group members may dissuade an individual from sharing relevant information or even sustaining their attention until it is “their turn.” To deal with this, it is recommended that group leaders periodically shift the target of their questions between specific individuals and the larger group.
b. Group leaders should also utilize different types of questions. For example, open-ended questions can be a great way of inviting ideas, general observations, and discussion of personal experience. However, some individuals may feel these questions are too broad and difficult to answer. Conversely, closed-ended questions are typically much simpler to answer, but may limit the amount of discussion on a topic. Group leaders can also use probing questions to help group members identify appropriate social information or hypothetical questions to consider how skills could be applied in alternative situations.
7. Give the group some control.
a. Group members tend to be more interested and engaged if they have a sense of ownership over the group. Seek feedback from group members about their preferences and allow the group to make decisions whenever possible. For example, there could be many different scenarios and activities available for individuals to practice targeted skills. Allowing the group to decide the activity will provide another “real-world” social communication opportunity and may lead to greater investment in the practice.
8. Tailor materials to the group.
a. All therapy interventions, particularly those which are highly manualized, carry concerns about fidelity. Significant modifications to the curriculum may weaken the effectiveness of the intervention. However, rigid adherence to the manualized treatment risks group members not understanding key concepts and skills. Sometimes, modifications can be helpful and appropriate if group members are struggling to understand material. Some group members may need additional review of core concepts. At times, group members may raise questions not directly related to the curriculum but may be highly relevant to their needs and/or experiences. By staying attuned to the group’s abilities and interests, group leaders can help members stay engaged with the material and maximize their learning.
9. When possible, try to use at least two group leaders.
a. Having a second group leader allows for easier multitasking and addressing any emerging needs during the session. As one leader leads the discussion, the other group leader can prepare the next activity. If an individual in the group requires one-on-one attention, support can be given without disrupting the entire group process.
10. Consider the benefits of snacks.
a. Abraham Maslow described a hierarchy of needs and described physiological needs as a necessity before other human motivations can take place. 8 Indeed, when hunger and other needs are not met, it can be difficult for individuals to focus on other tasks. Providing snacks is an easy way of helping individuals stay in a proper headspace during sessions.
Conclusion
In summary, social skill interventions are an area of high need for many individuals with ASD and other neurodevelopmental needs, and these needs typically persist across the lifespan. Additionally, social skills increase in complexity and nuance as individuals age; skills interventions need to reflect this. Helping individuals understand the proper context of skills expression—the “when” and “why”—can help promote generalization and adaptive functioning. Consider the power of video modeling, the critical benefit of peer generalization and other social exposures, and crafting outcome measures which truly reflect the skill’s socially valid expression when working on social skills. These efforts are time well-spent. Improved socially functioning can be a critical factor in increasing adaptive behaviors, greater community participation, more robust person-centered goal-setting, and risk reduction for victimization.
References
1. Pennsylvania Autism Needs Assessment: A Survey of Individuals and Families Living with Autism, Report #2: Service Needs. ASERT website. https://needs.paautism.org/wp-content/uploads/2020/05/Needs-Assess_ServiceNeeds_Sept-2011_M.pdf. Published 2011. Accessed May 4, 2021.
2. Pennsylvania Autism Needs Assessment: A Survey of Individuals and Families Living with Autism, Explore the Data: Social & Spirituality. ASERT website. https://needs.paautism.org/explore-the-data/social-spirituality/. Published 2018. Accessed May 4, 2021.
3. Reichow B, Volkmar F. Social skills Interventions for individuals with autism: Evaluation for evidence-based practices within a best evidence synthesis framework. J Autism Dev Disord. 2010;40(2):149-166.
4. Roth M, Gillis J, DiGennaro RF. A meta-analysis of behavioral interventions for adolescents and adults with autism spectrum disorders. J Behav Educ. 2013;23(1):258-286.
5. Rao P, Beidel D, Murray M. Social skills interventions for children with Asperger’s syndrome or high-functioning autism: A review and recommendations. J Autism Dev Disord. 2008;38(2):353-361.
6. White S, Keonig K, Scahill L. Social skills development in children with autism spectrum disorders: A review of the intervention research. J Autism Dev Disord. 2007;37(10):1858-1868.
7.
Duchenne GB. The Mechanism of Human Facial
Expression. New York, NY: Cambridge University Press; 1990. Maslow AH. A theory of human motivation. Psychol Rev. 1943;50(4):370–396.
8. Maslow AH. A theory of human motivation. Psychol Rev. 1943;50(4):370–396.
Biography
Michael Murray, MD is an associate professor of Psychiatry and Behavioral Health at Penn State College of Medicine. He is the director of the division of Autism Services for Penn State Health and the director of the central region ASERT collaborative. He is the creator of the Multi-Media Social Skills Program for Adolescents and the Multi-Media Social Skills Program for Adults—the ASERT social skills curriculums.
Jesse Northridge, LCSW is a licensed clinical social worker. He is part of the clinical team at the Autism and Developmental Disorders Clinic in the Department of Psychiatry for Penn State Health. In addition, he is a team member for the central region ASERT collaborative. He is the lead therapist for the ASERT social skills groups.
Contact Information
Michael J. Murray, MD
Penn State Health / Central ASERT
717-531-1115