Positive Approaches Journal, Volume 10, Issue 2
| Site: | My ODP |
| Course: | My ODP |
| Book: | Positive Approaches Journal, Volume 10, Issue 2 |
| Printed by: | |
| Date: | Sunday, August 9, 2026, 12:53 AM |
Positive Approaches Journal | 5

Volume 10 ► Issue 2 ► August 2021
Supporting and Informing Paths to Transition
Introduction
In
writing this introduction on the journal’s focus on transition, I marveled at
how individuals, families, and health systems have encountered and faced many
changes to processes and strategies, especially in response to COVID-19.
Transition is the process of moving successfully from the old to the new or
adapting to a new situation that can happen quickly or slowly. COVID-19 has
made us focus on the importance of transition and of the “here and now” of the
integration of community systems.
There are many questions that individuals, families, advocates, and community systems consider with transitions, and the answers often include specific processes, strategies, and community systems.
In this journal, I hope you will consider these questions:
- What are the various roles that facilitate change for people and communities before, during, and at the completion of transition?
- In what ways should those roles contribute to the promotion of well-being throughout transition?
Transitions can be supported by research, and experience provides a framework for application in practice, guidelines, and research. As a result, defined models of care are developed and cultivated with the integration of systems of care for such outcomes as quality of life, sense of well-being, and healing. Reading of this issue will provide you with knowledge to the ongoing research, the provision of expertise and skills, and strategies for healthy transition processes and outcomes.
—Marlinda Smith, LCSW, Dual Diagnosis Initiative Project Lead
Department of Human Services, Office of Developmental Programs (ODP)
Positive Approaches Journal | 6-9
Volume 10 ► Issue 2 ► August 2021
Data Discoveries
The goal of Data Discoveries is to present useful data using new methods and platforms that can be customized.
The COVID-19 pandemic
has upended how we participate in and interact with our communities. The most
effective strategies for staying safe and healthy for much of the pandemic
revolved around staying distant from one another, avoiding community locations,
and limiting public gatherings. This has caused many to feel isolated, alone,
and separated from their family, friends, and community1. In December of 2020, a new set of tools were added to the public
health arsenal to combat the COVID-19 pandemic and aid our transition to the
reintegration back into the community: the emergency use authorization (EUA) by
the Food & Drug Administration (FDA) for use of several vaccines to prevent
COVID-19. Vaccine rollout started out slow, limited to healthcare workers and
other essential staff, then to high-risk populations like older adults and
those with certain preexisting conditions and diagnoses, and slowly trickling
until all Pennsylvanians were eligible for vaccination on April 19th,
2021 pending the approved ages of each vaccine. As of August 2021, over 5.7
million Pennsylvanians have been vaccinated with the peak of vaccination in the
spring2.
Despite the now widespread
availability of the approved COVID-19 vaccines, the number of vaccinations
being administered has slowed. Despite calls to action for vaccination to
decrease community transmission of the coronavirus, Americans have been divided
in their beliefs about the whether-or-not to get one of the COVID-19 vaccines3.
The amount of published research is increasing on the safety of COVID-19
vaccines and the importance of correcting vaccine misinformation and the
continued efforts to promote evidence-based information and practices will be
critical in in the continued vaccination outreach efforts.
Continued efforts to combat misinformation and promote vaccination will be essential to continue to support efforts for vaccination for all eligible populations. Vaccination remains one of the most effective means to decreasing community transmission and facilitating our ability to reintegrate into our communities to the extent we were able to before the pandemic4. For more information about vaccination from the ASERT Collaborative via the AID in PA initiative, visit:
- COVID-19 Vaccine Information:
https://aidinpa.org/resource/covid-19-vaccine/
- Getting
the COVID-19 Vaccine Social Stories:
https://aidinpa.org/resource/covid-19-vaccine-social-stories/
- Decision Making for the COVID-19 Vaccine:
https://paautism.org/resource/covid-19-vaccine-faq/
Dashboard Instructions?
The Dashboard below aims to provide resources and information on the COVID-19 vaccination rollout nationally and within Pennsylvania. Navigate the ‘COVID-19 Vaccine Progress’ tab by clicking on an icon to visit the source webpage. The visual displayed on the ‘COVID-19 Vaccine Publications’ tab shows a timeline of COVID-19 publications related to the general public’s attitude towards getting the COVID-19 vaccination. Each circle represents a publication, with the size and color indicating how often the article was cited.
References
1. Banerjee D & Rai M. Social isolation in Covid-19: The impact of loneliness. International Journal of Social Psychiatry. 2020;66(6): 525-527. https://doi.org/10.1177/0020764020922269.
2. Benefits of getting a COVID-19 vaccine. Centers for Disease Control and Prevention website. https://www.cdc.gov/coronavirus/2019-ncov/vaccines/vaccine-benefits.html. Updated August 2021. Accessed August 5, 2021.
3. Lueck JA & Spiers A. Which beliefs predict intention to get vaccinated against COVID-19? A mixed-methods reasoned action approach applied to health communication. Journal of Health Communication. 2020; 25(10): 790-798. https://doi.org/10.1080/10810730.2020.1865488
4. COVID-19 vaccine dashboard. Pennsylvania Department of Health website. https://www.health.pa.gov/topics/disease/coronavirus/Vaccine/Pages/Dashboard.aspx. Accessed August 5, 2021.
Hogan | 10-18
Volume 10 ► Issue 2 ► August 2021
Effectively Utilizing the Space Between What Was
and What Will Be
Francine Hogan
Summary
Life transitions can bring excitement, possibilities, and sometimes uncertainty and anxiety. Transition planning must start early, utilize a Person-Centered approach, solidify support, define the vision, and be as unique as the person transitioning. Person-Centered Planning can take place at any time in a person's life. It is best done before transition services are determined1. This all sounds good in theory, but putting it into practice can be more complex, especially during the unprecedented times of the COVID-19 pandemic. That is why the approach must be collaborative, flexible, and accessible to everyone. The LifeCourse Framework gives us everything we need to plan, implement, and sustain a successful transition. The Charting the LifeCourse framework was developed to help individuals and families of all abilities and all ages develop a vision for a good life, think about what they need to know and do, identify how to find or develop supports, and discover what it takes to live the lives they want to live.
“Begin with the End in Mind” is habit number two in Stephen Covey’s book “7 Habits of Highly Effective People2.” Many of us remember the impact Covey’s book had on business and management, but his book is more than that. It truly puts forward his theories in the form of a series of habits explaining the steady progression moving from dependence toward independence and finally to interdependence. To begin with the end in mind helps us understand how to plan for any transition.
“Begin with the End in Mind means to start with a clear understanding of your destination. You need to know where you are going in order to better understand where you are now so that the steps you take are always in the right direction2.” – Dr. Stephen R Covey
Transition is defined as movement, passage, or change from one position, state, stage, subject, or concept to another3. We all experience multiple transitions throughout our lifespan. For people with disabilities and their families’ transitions are particularly complex.
Traditionally, when we think of transition, we think of the major life changes such as Early Intervention to school, high school to adulthood, and adulthood to old age. Most recently, as a society we have experienced significant events that have caused us to think about what reintegration looks like post-pandemic. Where were we before COVID-19? Where are we now? Where do we want to go? All familiar questions when we plan for transitions. Transition planning is a process that help us decide what comes next and how we get there; it is more than just a hopeful exercise or brainstorming session. This process is a thoughtful set of activities, experiences, supports, and services that must start with a vision.
Successful transition necessitates the need to use the practices of a Person-Centered Planning tool, such as the LifeCourse Framework 4.
Charting the LifeCourse is a framework created to help
individuals and families of all abilities and ages develop a vison for a good
life, think about what they need to know and do, identify how to find or
develop supports, and discover what it takes to live the life you desire. Once
the principals and foundations of the Framework are understood, it can be used
and applied by anyone to plan or solve a problem.
The first step in using LifeCourse to plan for a transition is for a person to develop a vision of what they want and do not want in life. For this, it is important to consider all areas of the person’s life, also known as the 6 Life Domains (pictured below).

For example, when planning for life after high school, a person and their family should think about where they will live, how they will spend their day, how they will stay safe and manage money, how will they build friendships and community connections, and what role will they take in their own self-determination and in their community. Equally important are their personal strengths and assets, what is important to them and how to best support them. First, consider a person’s past experiences and opportunities. Which ones brought them closer to their vision? Those are the experiences that should be built upon or repeated in the future. Then, think about the ones that have led them away from what they want. Those experiences are lessons and should be acknowledged, so they can be avoided in the future.
It is paramount that everyone involved in this process assumes competence and has high expectations for the person at the center of the plan. Remember, experiences shape expectations and expectations shape experiences. A few negative outcomes should not be a life sentence for a person. For example: Stocking shelves at the local pharmacy might have been unsuccessful for a transition age student. It might have caused challenging behaviors, property destruction, and maybe even aggression toward others. That outcome does not mean the student is not employable. It just means that it was not the right fit. Keep expectations high and assume competence. Learn from the experience and try again.
We all access an array of integrated supports to achieve our
vision. The LifeCourse Framework helps us understand how we can have the
services and supports we need, when and where we need them. These integrated
supports can be privately or publicly funded and based on eligibility,
community supports that are available to anyone, relationship-based supports,
technology, and most important the strengths and personal assets of the person
at the center of the plan.
Using this Framework, we will present a transition case study and demonstrate how using the LifeCourse Framework resulted in a smooth transition and transformational change.
Case Study
Using Charting the LifeCourse to Transition Back to Services
Summary
JB is a 32-year-old who experiences an intellectual disability and autism. Prior to the COVID-19 pandemic (up to March 2020), JB attended a day program that provided Community Participation Support. JB’s day-to-day life during the height of the pandemic was isolating and frustrating. JB’s mom knew something had to change. Through mentoring sessions with the Pa Family Network, JB and his team were able to plan a transition back to community activities and to reimagine how he received services.
Background
Prior to COVID-19 JB attended a day program full time and lived at home with his mom. It was reported that he enjoyed the activities and had many friends. Up to the time of COVID-19 shutdowns, there seemed to be no reason to do anything different. That all changed in March of 2020. Some remote supports were provided, but they were not the right fit for him. His mom and Behavior Specialist reported that due to the changes in routine, days of inactivity, and loss of connections, JB was regressing, and had begun communicating his feelings through challenging behaviors. His mom took leave from her essential job to help him through this difficult time, but she knew this could only be temporary. The sudden closing and intermittent openings of the program created too much uncertainty for JB and his mom. JB’s mom reached out to the Pa Family Network after attending a LifeCourse workshop. She requested a mentoring session in hopes of using LifeCourse to think about JB’s life differently, and ultimately to inform their long-term planning efforts. Over a series of 3 sessions, JB had a complete LifeCourse Portfolio and an innovative plan develop.
What We Learned
Through the journey of our LifeCourse mentoring we learned JB is a social and engaging individual who struggles with language. JB is making progress using an icon exchange app on his iPad. It is important to him to watch sports, go to the gym, keep his things in order, stay occupied, and spend time with his older brother, sister-in-law, and his nephew. It is important for JB to have his wants and needs understood and honored, to have choices, stay safe while out and about, keep busy, and try new activities. His vision is to play sports, spend time with his friends and family, be healthy, have muscles, and make money. His mom added that she knows from her experiences that he wants choice and control. His mom added she wants a more reliable, person-centered approach to his services and for him to learn to do more for himself. He does not want uncertainty, chaos, or to be bored.
Some activities and opportunities on JB’s LifeCourse Trajectory include moving his communication app to his phone for convenience, gym membership, having a first-time job experience related to sports/gym, community volunteer opportunities, self-directing some of his services, building independent living skills, keeping in touch with friends from day program, and attending local sporting events. JB has many paid and unpaid supports available to help him achieve his vision. Some of these supports are his mom, brother, friends, Supports Coordinator, and church friends. Community supports include the local gym, high school sports, church, physical therapy practice, library, rock wall gym, AAA baseball team, “Community on the Move” committee, and multiple hiking/walking trails. He is skilled with the use of computers, iPad, iPhone, and can stay on Zoom for about 15 min. JB is a good problem solver, he is organized, likes things clean, he is friendly and enjoys new adventures. Eligibility related services include waiver, supports coordinator, employment services, gym membership, and Social Security Income (SSI).
Case Outcome
JB now attends his day program 2 mornings per week to keep in contact with old friends. Three afternoons per week, he uses Advanced Supported Employment services to support him with his job tasks at the local physical therapy practice and the gym. Both businesses found it hard to keep the equipment clean and organized, so JB’s employment supports provider helped the businesses create a job that was beneficial to all parties. Then, three mornings per week he focuses on developing independent living skills using In-Home and Community Supports. He is learning to vacuum the house, take out the trash, wipe down the counters, and prepare his preferred meals in the microwave. The rest of the time his staff assists him to volunteer, attend “Community on the Move “meetings to plan their 5K, explore trails, parks, and other community locations where he can learn community safety skills, exercise, and meet more neighbors. JB’s mom is his surrogate and utilizes the Supports Broker Service, which is designed to assist with some of the tasks related to self-directing waiver services. The Supports Broker is helping them to shape JB’s new self-determined everyday life. They are successfully using a traditional provider model and self-directing other services to help JB achieve his vision. JB’s mom is also confident that if there are more shutdowns his life will not be shut down with the system. She is managing staff that is trained well, connected to JB, and can continue helping JB work toward his goals even if everything is closed. JB and his mom have indeed experienced transformational change.
What if we raise our expectations of transition planning and instead of expecting simply transitional change we strive for transformational change? Dr. Erik Carter’s research: What Matters Most5 tells us that “the most powerful force for changing transition outcomes, in young people with significant disabilities, is not ultimately found in the transition plans we craft, the educational services we offer, the instruction we provide, or the systems we build, but rather in the expectations and aspirations individual parents hold for their sons and daughters.”
Life transitions require careful
planning, coordination, and communication, but we can achieve real
transformational change when we add the high expectations of everyone involved.
If you or your loved one experiences an intellectual disability and/or autism
and need assistance with planning or problem solving contact the Pennsylvania
Family Network.
The bridge we build, between what was and what
will be, should be a sound structure leading to the life you desire.
References
1. Person Centered Planning Can Take Place. Pacer’s National Parent Center on Transition and Employment website. www.pacer.org/transition/learning-center/independent-community-living/person-centered.asp. Accessed August 19, 2021.
2. Covey SR. Begin with the end in mind. 7 Habits of Highly Effective People. Free Press, 1989.
3. What Does Transition Mean? New York State Multiple Systems Navigator website. https://www.msnavigator.org/transition-to-adulthood/transitions-big-picture/what-does-transition-mean. Accessed August 19, 2021
4.
LifeCourse
framework. University Missouri -Kansas City Institute for Human Development
website. https://www.lifecoursetools.com/lifecourse-library/lifecourse-framework/. Published 2010.
Accessed August 19, 2021
5. Carter EW. What matters most: Research on elevating parent expectations. Institute for Community Inclusion. http://supportstofamilies.org/wp-content/uploads/parent-expectations_D21.pdf. Published 2015. Accessed August 19, 2021.
Biography
Francine Hogan has been involved with the disability field for over 19 years. Her advocacy work began when her now 21-year-old son Michael was diagnosed with an intellectual disability, autism and Tourette syndrome. Francine is an experienced presenter, locally and nationally, on multiple disability systems and topics. Currently, Francine is the Director of the Pa Family Network for Vision for Equality and a LifeCourse Ambassador. She oversees the operations of this statewide initiative, which helps families navigate systems, plan, network, and identify the services and supports their loved ones need to lead an everyday life. In this capacity she also serves as a Statewide Lead for the Pa Community of Practice for Supporting Families throughout the lifespan.
Contact Information
Francine Hogan, Director
Pa Family Network at Vision for Equality
1007 N Front Street, Suite 1N ~ Harrisburg, PA 17102
844-723-2645 ~ www.visionforequality.org
Hollander | 19-29
Volume 10 ► Issue 2 ► August 2021
Using Goal Attainment
Scaling to Measure Progress and Make Instructional Decisions
Jordan Hollander M.Ed BCBA
Abstract
Goal Attainment Scaling (GAS) is a method to standardize and measure outcomes for individualized goals. This article will review the core features of GAS and provide an example of how to develop a GAS chart, determine the Level of Attainment, and make instructional decisions based on that level.
As
we continue to return to the community after over a year of lockdowns and
limited gatherings related to the COVID-19 pandemic, it is important we take a
moment to reflect. For many of us the goals we had for ourselves have changed
significantly over the past year. Things that seemed to be urgent might now
seem unimportant, while other seemingly trivial activities might now feel
essential to our well-being in a still uncertain future. As we reflect on what
has changed for ourselves, it is just as important to help the people we
support reflect and reframe what is important to them moving forward.
A part of this reframing, especially for those who have had major changes to their routines, health, or social network, should be to revisit service outcomes and goals with the individual. This process will look different depending on the individual and their preferences. Some may prefer a more formal meeting, such as an Individual Support Plan (ISP) meeting, to review their outcomes or goals while others may prefer a more informal discussion before having a discussion with a larger support team. No matter how the discussion begins, it is important that the focus is not only on setting goals that are meaningful to the individual, but also developing a method to plan for and evaluate expected progress towards those goals.
Goal Attainment Scaling
With such individualized goals, it can be challenging to assess whether supports are effective in achieving the intended results. Goal Attainment Scaling (GAS) provides a solution to that challenge.
At its core, GAS is a criterion-referenced method to standardize and measure outcomes for individualized goals. Developed in the late 1960’s by Thomas Kiresuk and Robert Sherman to evaluate program effectiveness in mental health settings, GAS has since been adapted for use in a variety of health and school-based settings1,2,3. In Pennsylvania, the Adult Autism Waiver and Adult Community Autism Program have been using GAS to measure and report on individual outcomes since 2016.
The GAS process includes three basic steps, (a) identify an individualized goal (b) develop an individualized GAS chart, and (c) implement strategies and determine the Level of Attainment to report on progress 1.
Goal Setting
Collaborative goal setting is an essential component of effective service delivery but can often lead to vague and overly generalized goals that make it hard to track progress and determine if services are effective in achieving the goal3. GAS requires that goals be individualized and measurable1. The individualized component focuses on goals that are meaningful to the participant and in line with their values and vision for the future, while the measurable component ensures that a reliable GAS chart can be developed3,4.
In practice this can play out in a variety of ways, but typically it will begin with a conversation about what is important to the individual and what they want to get out of the service they are receiving. Once a general goal is identified, the support team needs to help refine this goal into something specific and measurable. This requires (a) knowledge of the individual’s current abilities related to that goal, as well as (b) an understanding of a reasonable expectation for the progress the individual will make towards that goal during the period for which the GAS chart is developed3.
Though not always practical, when obtaining knowledge about the individual’s current abilities, it is best to observe the individual demonstrating the skill to obtain baseline data. Another way to determine the individual’s current abilities is by identifying their Stage of Learning.
The Stages of Learning include (a) Skill Acquisition, (b) Skill Fluency, and (c) Skill Maintenance or Generalization. To identify an individual’s stage of learning for a specific goal, the team can start by asking a few questions. Has the individual ever done the skill before? Do they rely on others to begin or finish the skill? Does the individual know when they completed the skill? Is it realistic for the individual to learn this skill independently or will some support always be needed?
Once the goal is developed in this manner the expected outcome is discussed and an agreement is made between the individual and support team that this is important to the individual and a realistic expectation of what is likely to be achieved by the end of the GAS chart date4,5.
Chart Development
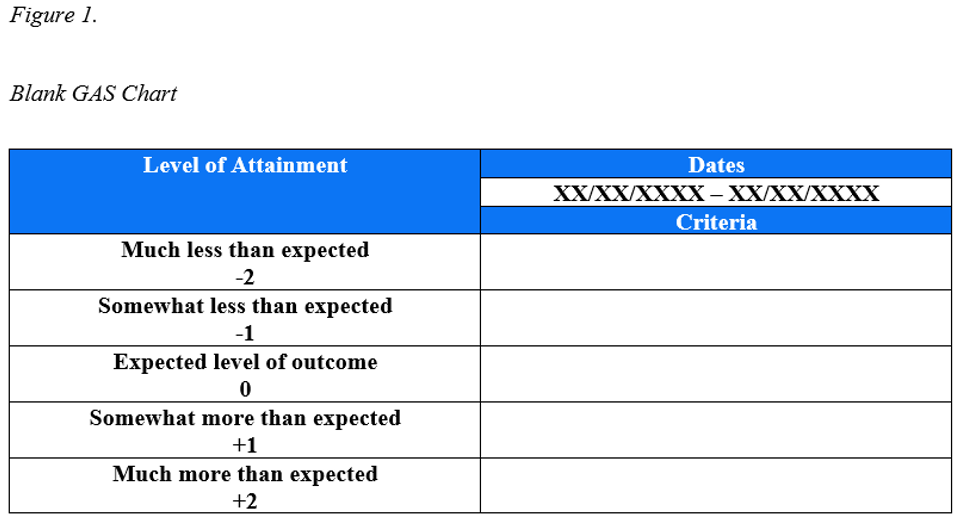
GAS measures goal attainment by establishing criteria for an expected outcome and then developing a 5 point rating scale based on that criteria. The scale ranges from -2 (much less than expected) to +2 (much more than expected) with 0 being the expected level of attainment. After the period specified, the goal attainment is rated using the GAS scale based on the criteria achieved during that period1,2. (See Figure 1.)
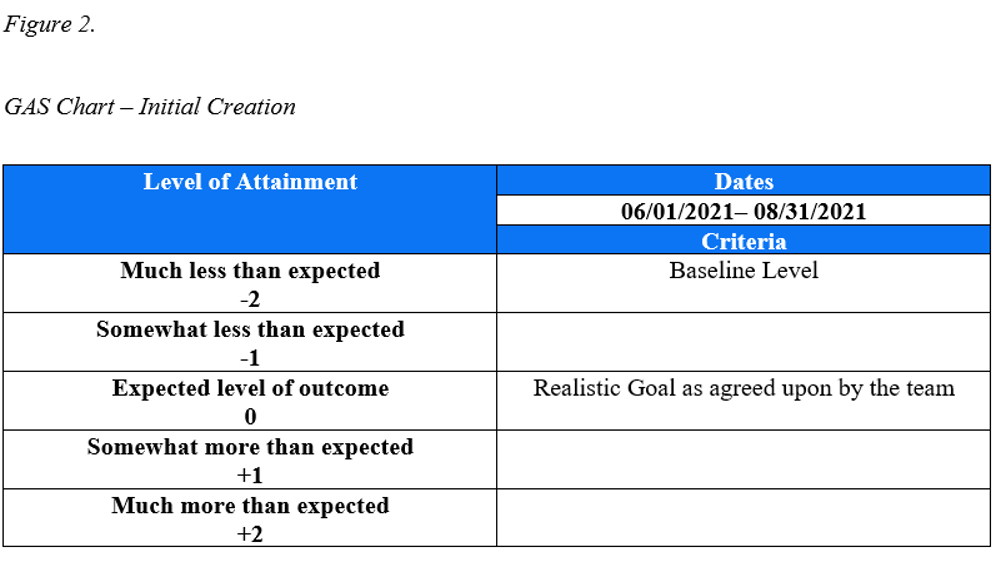
The information collected during the goal setting step will be used to fill out two of the points on the GAS chart. The information about the individual’s current ability or baseline data should go into the scale for level -2, as the intent is for the individual to make progress from where they were at the start of this goal. The realistic expectation of what is likely to be achieved by the end of the GAS chart date goes into the scale for level 0 as this is the expected level of outcome for the period. Level-1 is then filled out with a criterion point that would indicate some progress above the baseline that does meet the expected level. Finally, Levels +1 and +2 would include criteria that indicates the individual has made more progress than expected1,2,4,5. (See Figure 2.)
Level of Attainment
Once the goal is set and the GAS scale is developed, the individual begins working on the goal with their support team and data are collected for the set period. This data can be captured through observations, rating scales, or other self-reporting methods. The data that is captured should provide enough information to identify all the components of the criteria listed for each level in the GAS scale. At the end of the set period, the data is reviewed, and Level of Attainment is assigned based on the criteria for the corresponding level in the GAS scale. 1,2 The team can then use this information to make instructional decisions about the goal. If the individual has not made expected progress, this should prompt conversations about the goal, its importance to the individual and potential changes to how any teaching or support components of the goal are implemented by supporters.
GAS Example
Ted
is a 25-year-old man who receives waiver services. Before COVID-19, Ted had a
job working at a small coffee shop cleaning tables, washing dishes, and
cleaning the bathrooms. The coffee shop closed their indoor dining at the
beginning of the pandemic and is set to reopen in the next few weeks. Last
week, Ted’s boss reached out to let Ted know that they want him to come back to
work but asked if he would be willing to work a morning shift instead of his
usual afternoon shift.
Ted is excited to go back to work but is concerned about switching his shift times. Ted is used to having all morning to get ready for work and is concerned about having to wake up earlier and potentially being late or rushing and forgetting to complete steps of his morning routine. Hearing this, Ted’s support team works with him to set a goal. Ted’s original stated goal is to avoid being late to work, and his team helps him to break the goal down into something more specific. They determine that for Ted to complete his morning routine and make it to work on time he needs to wake up by 6 AM and leave by 8 AM. Ted and his team work together to figure out the supports that Ted will towards this goal. They help Ted set an alarm, make a task list for his morning routine, and go over some strategies around sleep hygiene. For the next week, Ted agrees to try and complete this routine as an experiment, even though he does not have to go to work. After a week, Ted was able to wake up at 6AM, complete his morning routine and leave by 8AM on two out of five days with some prompting from his brother. Ted and his team agree it is realistic that he can improve to 5 days per week, but Ted thinks he will still need some prompting from his brother. The team also agrees not to use waking up at 6 AM as part of the goal criteria, if Ted completes his morning routine and leaves the house by 8 AM, but Ted agrees to continue to track what time he is waking up. Using this information, the team creates a GAS chart (see Figure 3) as well as a way for the team to keep track of when he wakes up, how much of his morning routine he completes and when he leaves the house.
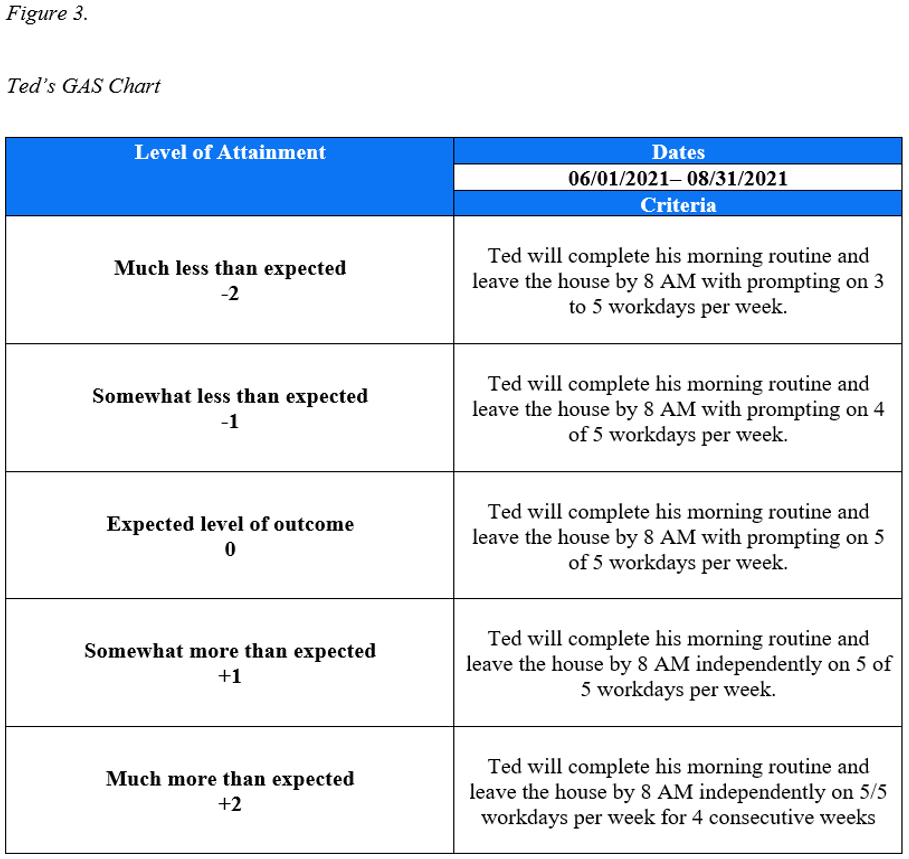
On September 30th, the end of the GAS Chart
date, the team will review the data and determine a Level of Attainment for the
period and use that information to update the goal and support strategies
related to the goal as necessary.
Conclusions
In our field we use words like “outcomes,” “goals,” and “visions” to discuss how we can support people in planning for the future. GAS is a tool used to provide support and communication about what is and is not working to help the people we support meet the ultimate goal, to live a meaningful, self-determined Everyday Life.
Resources
References
1. Kiresuk TJ, Sherman RE. Goal attainment scaling: A general method for evaluating comprehensive community mental health programs. Community Mental Health Journal. 1968; 4: 443–453. doi:10.1007/BF01530764.
2. Kiresuk, TJ, Smith A, Cardillo JE. Goal Attainment Scaling: Applications, Theory, and Measurement. Hillsdale, NJ, England: Lawrence Erlbaum Associates, Inc; 1994.
3. Shogren KA, Dean EE, Burke KM, Raley SK, Taylor JL. Goal attainment scaling: A framework for research and practice in the intellectual and developmental disabilities field. Intellect Dev Disabil. 2021;59(1):7-21. doi:10.1352/1934-9556-59.1.7.
4. Lee CE, Shogren KA, Segal J, Pezzimenti F, Aleman-Tovar J, Taylor JL. Goal attainment scaling—community-based: A method to incorporate personalized outcomes into intervention research with youth and adults on the autism spectrum. Autism; June 2021. doi:10.1177/13623613211024492.
5. Ruble L, McGrew JH, Toland MD. Goal attainment scaling as an outcome measure in randomized controlled trials of psychosocial interventions in autism. J Autism Dev Disord. 2012;42(9):1974-1983. doi:10.1007/s10803-012-1446-7.
Biography
Jordan Hollander M.Ed BCBA is a Senior Clinical Consultant for the Office of Developmental Program – Bureau of Supports for Autism and Special Populations. He has been working for the past 12 years to help people on the Autism Spectrum identify goals, and work towards achieving them through a person-centered approach that utilizes the principles of Positive Behavioral Supports. Jordan has worked in various Direct Support Professional (DSP) roles as well as in Clinical and Operational management positions for various service providers throughout Southeastern Pennsylvania.
Contact Information
Jordan Hollander M.Ed BCBA
Rabian | 29-36
Volume 10 ► Issue 2 ► August 2021
Moving in the Same Direction: A Case Study of How Integrated Care Can Support Independence and Community Living for Individuals with Complex Needs
Brian Rabian, PhD
Abstract
The case of “Steven” highlights the progress possible for individuals presenting with complex challenges when stakeholders are committed to open communication and coordination, and when systems support innovation in programming. For Steven, the journey from managing crises through hospitalizations to stable community living was achieved through development of a new treatment model, and ongoing expansion of his care team to include members able to help address unique needs. Steven’s case highlights the breadth of services available to individuals when all available treatment systems and funding sources are utilized.
Through collaboration with members, families, providers, advocates, and counties, Community Care Behavioral Health (Community Care), a nonprofit behavioral health managed care organization (BHMCO) created in 1996 to support HealthChoices, Pennsylvania’s mandatory managed care program for Medicaid recipients, has implemented and supported innovative programs reflecting the core principles of the Everyday Lives1 initiative of the Pennsylvania Department of Human Services. These principles include that all individuals with disabilities should be able to experience the same opportunities, relationships, rights, and responsibilities as their fellow citizens, and this includes being a member of a community, with appropriate supports available. The independence of individuals dually diagnosed with mental illness and an intellectual disability or autism can best be achieved through a shared commitment by stakeholders to best practice guidelines, ongoing education, and shared decision making. Representatives from Community Care, including these authors, have been fortunate participants in the ongoing Capacity Building Institute (CBI) a joint initiative of Pennsylvania’s Office of Developmental Programs (ODP) and Office of Mental Health and Substance Abuse Services (OMHSAS). CBI offers an in-depth learning opportunity to professional stakeholders, across a diverse array of agencies (e.g., direct support providers, managed care organizations, residential treatment centers, state hospitals) with the goals of promoting best practices, while building a statewide cohort of individuals and systems better equipped to effect change. These goals are particularly important in the treatment of individuals who are dually diagnosed, as they are often subject to experiencing frequent transitions in treatment due to complex and fluctuating needs. The diversity of participating stakeholders in CBI shed light on how traditionally distinct service systems with separate funding sources and eligibility requirements can work in concert for the benefit of the member. The following case discussion highlights the use of ongoing evaluation and frequent coordination to support transitions and foster independence in the treatment of an adult man presenting with challenging medical and behavioral concerns.3 This description does not represent an actual individual. Rather, it reflects the collective clinical experiences of members of the Community Care workgroup and is intended to highlight the positive change available to all individuals when stakeholders work together.
Steven
Steven is a 45-year-old man diagnosed with impulse control disorder, and intellectual disability-severe. He presents with multiple medical conditions that require regular attention, and that have caused some to describe him as “delicate.” During an extensive history of treatment, Steven experienced multiple involuntary hospitalizations, due to difficulties in maintaining medical stability, and safety concerns related to aggression directed toward staff and self-injurious behaviors. The hospital was viewed as critical to helping Steven regain stability when in crisis, with extremely limited community options available to help fill this role. These hospitalizations underscored the concern carried by Steven’s parents, and fueled their advocacy for the establishment of better community options for people like Steven2. Steven’s parents, now both in their late 70’s, are committed to Steven’s goal of being maintained in a community setting, with as much independence as he is able to develop.
When younger, Steven often experienced regression in medical and behavioral functioning due to several factors. Steven possesses a limited vocabulary, and his articulation makes him difficult to understand. Steven’s parents have worked regularly with providers to transfer their understanding of his speech. Steven has long had problems with poor sleep, with no obvious contribution from sensory or environmental factors. He is prone to leaving his bed and walking around the house at night, and lack of sleep contributes to dysregulation, including refusal to comply with his medical treatment.
Steven’s medical well-being is often seen as a driver of his behavioral functioning. He experiences frequent physical discomfort, and his medical needs have resulted in a significant medication regimen, and ongoing nursing assessment and assistance. Most of Steven’s medications are managed through his primary care physician, but he does also see a psychiatrist for the management of anxiety and mood, and a urologist to help manage persistent incontinence. The coordination of medical professionals is critical to his well-being, as he is prescribed medications for more than seven different conditions. Not surprisingly, in addition to his ongoing behavioral goals, Steven has goals related to adherence with his medical treatments. The most constant indicator of discomfort and predictor of behavioral regression has been Steven’s engagement in medical refusal behaviors, aggression, and self-injurious behaviors. When agitated, Steven attempts to pinch staff. He also scratches or pinches himself. A major point of coordination between Steven’s parents and his treatment team focused on helping team members better understand indicators of Steven’s discomfort, and to proactively use preferred activities to help distract from these sensations. Avoidance of the use of restraints in the treatment of individuals who are dually diagnosed is of paramount importance to protect their rights. In Steven’s case, restraints were further deemed inappropriate due to his physical fragility and risk of injury. Following a particularly dangerous episode, Steven’s treatment team sought and received a short-term prescription for Steven to wear extra-long sleeves to prevent pinching, and they began offering soft objects to occupy Steven’s hands temporarily. Use of these methods was also paired with several preferred activities, such as singing, watching videos, and walking with a staff member. Steven eventually began to seek out the soft objects, in part to signal his desire to engage with others. Steven’s progress in reducing hitting and pinching opened the opportunity for him to safely participate in activities through the ARC in his home county, and he built positive relationships with peers through shared walks and recreational activities.
An ongoing challenge in Steven’s treatment involved the inability of any one agency or provider to adequately accommodate Steven’s significant needs related to housing, communication, nursing, safety, and recreation. It should be noted that most of Steven’s early support came through his diagnosis of intellectual disability, which opened eligibility to specialized services through his home county and ODP. However, his parents were unaware of behavioral supports that might be available to Steven through Medicaid and his county HealthChoices program until this option was raised at a school coordination meeting. This discovery opened opportunities for Steven to receive case management, behavioral consultation, and staffing to implement positive behavioral strategies.
Efforts to help Steven transition to the community as an adult resulted in multiple rejections for placement. It was the shared commitment across multiple stakeholders that eventually opened opportunities for Steven slowly to transition out of his parents’ home, and to be maintained long-term in his community. The first step involved getting all stakeholders to the table together, with Steven’s interests as the central focus. In Steven’s case, stakeholders include Steven, his parents, a community supports coordinator, representation from ODP, and a Clinical Manager from Community Care. Weekly coordination meetings identify community resources available to Steven, engage in collective decision-making, and support natural and paid resources. In Steven’s case, the stakeholders regularly attending coordination meetings has grown to include multiple prescribers, consultants, and a dietician. Despite the benefits experienced through this coordinated effort, Steven’s placement continued to be characterized by crisis episodes leading to hospitalization, and occasional short-term respite stays at his parent’s home due to unforeseen challenges brought on by experiences such as staff turnover.
A significant change in Steven’s care followed the development of several community resources through the Behavioral Health Alliance of Rural Pennsylvania (BHARP). Specifically, Steven benefited greatly from the development and availability of the Dual Diagnosis Treatment Team (DDTT) model in 2014, which was the result of a workgroup focused on how to respond to unmet needs of dually diagnosed individuals. The workgroup included representatives from county Mental Health and Intellectual Disabilities departments, Community Care, ODP, OMHSAS, and psychologists with specialized knowledge of this population. The multidisciplinary treatment team developed in the DDTT model allows for medical and behavioral needs to be met in a community setting, in which independent living skills might be developed. Specifically, the DDTT treatment team includes a psychiatrist, Program Director, Behavioral Specialist, Nurse, Service Coordinators, and Pharmacy Consultant. For Steven, the integration of physical and behavioral health allowed for better avoidance of crises, and the ability to respond more quickly to acute needs.
Several years
after development of DDTT, a partner model was created. Community Stabilization
and Reintegration Unit (CSRU), a residential treatment facility for adults, is
particularly helpful as a temporary step-up for individuals in crisis.
Together, CSRU and DDTT function as a continuum of care for adult members, as
members can easily go between both programs, which are meant to assist each
other. Steven is representative of many individuals who have benefited from the
existence of these programs. Data from Community Care’s records over the past
two years indicate that DDTT has served more than 379 distinct individuals,
ranging in age from 15 to 76 years, across dozens of counties in Pennsylvania.
Similarly, CSRU has served more than 75 distinct individuals in that time,
ranging in age from 15 to 70 years. Programs such as these, along with nearby
availability of hospitals in the member’s community, serve as important safety
nets in the transition to community placement.
One of the hallmarks in Steven’s treatment that should be observed in the treatment of individuals with similar needs, is the role of ongoing evaluation and coordination. When Steven first presented at his DDTT agency, he suffered from significant physical challenges. The treatment team recognized that Steven’s transition could not be viewed as routine or predictable. As a result, they brought in a medical consultant to conduct a thorough evaluation of Steven’s needs during the transition and beyond, which resulted in a change in dietary recommendations, temporary use of a visual board to aid in communication as staff learned to understand Steven’s speech, and a recommendation to increase tactile activities to maintain social interaction and reinforcement. Ongoing evaluation has allowed the treatment team to adapt to the changing nature of Steven’s needs, and expand team members as needed to meet Steven’s developmental, cognitive, emotional, behavioral, and medical needs in as comprehensive a manner as possible. It is fair to say that, without the excellent coordination between service systems, Steven’s ability to be maintained in a community might have been untenable. His case underscores how even complex challenges can be overcome to the benefit of service recipients when available stakeholders are committed to common goals and creative problem solving.
References
1. Everyday Lives: Values in Action. Pennsylvania Department of Human Services, Office of Developmental Programs. 2016.
2.
Salzer
M. Community inclusion as a human right and medical necessity. Positive
Approaches Journal, 2019;8(2), 29-35.
3. Westerfield SE. Utilizing effective communication across teams to support successful transition into the community. Positive Approaches Journal, 2020;9(2), 86-94.
Biographies:
Brian Rabian is a Manager of Psychological Services and Professional Advisor for Community Care. Prior to joining Community Care, he was a faculty member at the Pennsylvania State University, University Park, and Director of the Penn State Psychological Clinic.
Contact Information
Brian Rabian, Ph.D.,
Community Care Behavioral Health Organization
Workgroup members from Community Care, who participated in the writing of this article include the following: Tiberiu Bodea, Duncan Bruce, Michael George, Jamie Pyo, Teri Stanley, RaeAnn Taylor and Jennifer Willier
Self-advocates United as 1 | 37-42
Volume 10 ► Issue 2 ► August 2021
My Life, My Way:
After the Pandemic: Let’s Talk
with Self-advocate
Self-advocates United as 1 Members and
Facilitators
Self-advocates United as 1, Inc. (SAU1) is a statewide Pennsylvania non-profit, led by a volunteer board of directors who are all people with developmental disabilities. SAU1 was founded in 2007 and gained its independence in 2015. SAU1 Power Staff are mostly professional self-advocates with support from experienced facilitators from all over the state. SAU1 volunteers and staff are passionate about SAU1’s mission: To support the self-advocacy of people with disabilities for positive impact in our communities and in people’s lives.
SAU1 manages the Self Advocacy Power Network for All (SAPNA), a project of the Pennsylvania Office of Developmental Programs (ODP) since 2016. SAPNA provides interactive events for self-advocates written and led by professional self-advocates. SAPNA also supports leadership development including empowering self-advocates to use their voices in meetings and events that affect their lives, to put into action our belief that there should be Nothing About Me, Without Me!
SAU1 staff and volunteer leaders met virtually to talk about “My Life, My Way – After the Pandemic,” following a request from ODP to offer personal experiences and thoughts. The people involved included 11 self-advocates and 4 facilitators who are also family members. Everyone shared their own personal views, not the views of the organization. People could give multiple answers to each question and are included in the narrative and captured in the charts when more than one person gave the same answer. Our goal and hope is for people to learn from their answers.
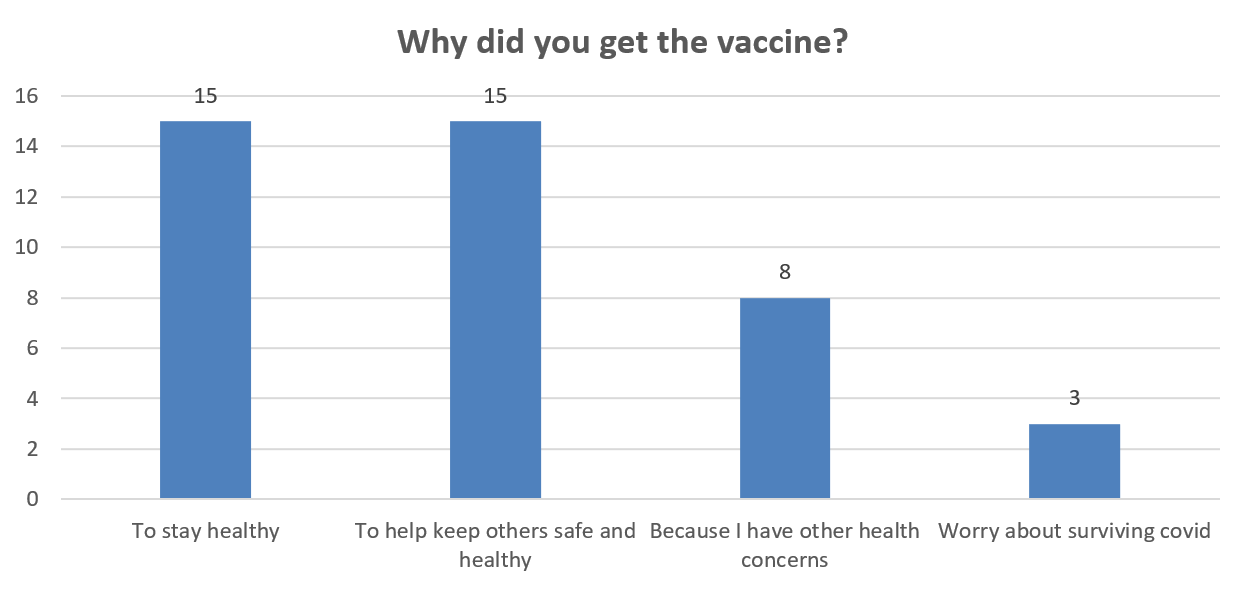
“If you are vaccinated, why did you decide to do it?”
Everyone
shared that they wanted to stay healthy, and to help keep others safe and
healthy. Many shared thoughts of people
important to them – a Grammy, a mother with cancer, a 91-year-old father, and
grandchildren and others who could not be vaccinated. One person said, “It is better to be safe
than sorry, and I’m proud that I don’t want to get anyone else sick.” Many
shared that they have other health issues or conditions and worry that they
might not survive COVID. One took the advice of his doctor who said it was the
best thing to do because of their health and disability. One went through three
personal COVID scares and doesn’t want any more. Another shared that people get
really sick from COVID, and vaccines keep him safe. One lived through a mild
case of COVID and decided that if that was what a mild case was like, she did
not want to risk getting a more serious case. Another doesn’t want to lose any
more friends to COVID. One person wants to protect himself from people who
don’t take COVID seriously. He feels getting vaccinated is his responsibility
both as a human being and a citizen. (See Figure 1.)
Figure 1.
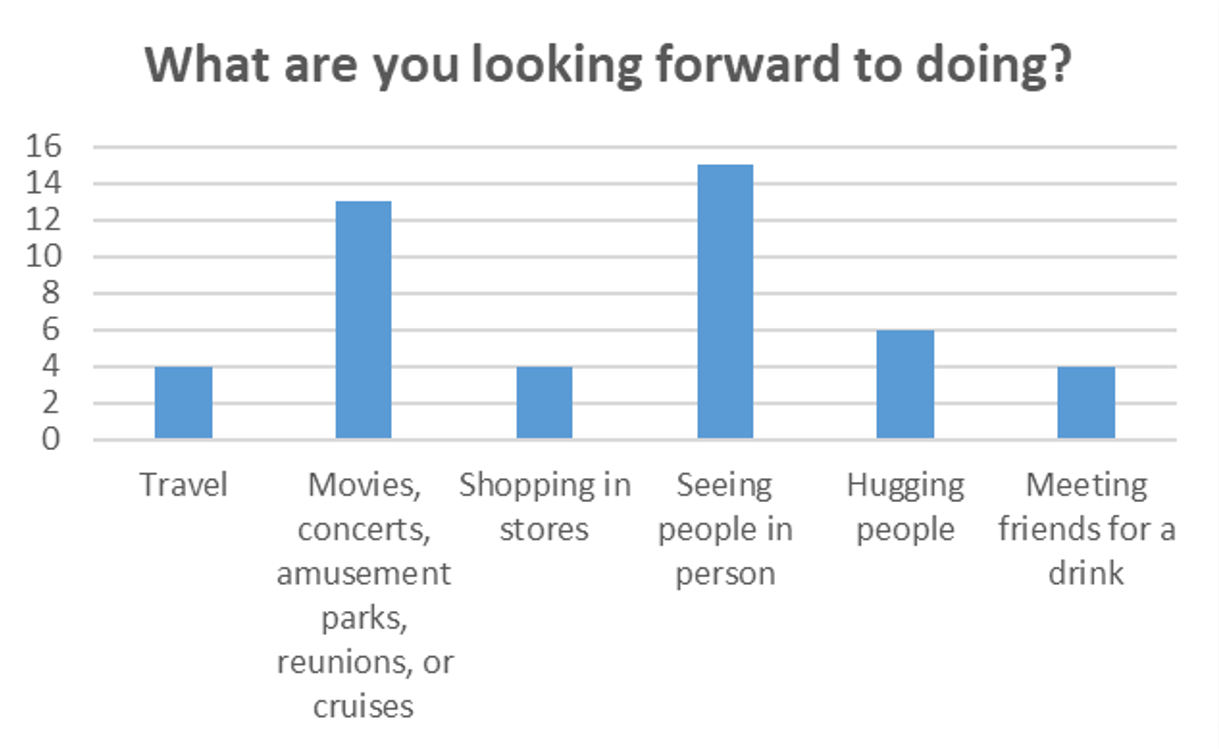
“What is something you are really looking forward to doing?”
People
were very excited to talk about things for which they have been hoping and
waiting. Several shared that they can’t wait to travel, out of town, overnight.
Dreams of going to the movies, to concerts, to amusement parks, to family
reunions, on a cruise, shopping in a store instead of online, and meeting
friends for drinks were all talked about. Being able to see people in person,
including family members and friends, and hugging them were also important.
Everything they liked to do before the pandemic is important to them all. (See
Figure 2.)
Figure 2
“How are folks feeling about returning to things in the community?’
Most
are anxious, unsure, and nervous. Some are ready to go slowly and put
themselves out there. For those in areas where masks are no longer mandated for
vaccinated people, some feel anxious when they go out without a mask since they
are so used to it. One person shared that he had been to a couple of festivals,
and it felt weird because he didn’t recognize friends since it had been two
years since he’d seen them. Others are looking forward to returning to some
sense of normalcy, but their families are concerned that something else –
especially another pandemic – may come, so are being very cautious. Some are
worried because they don’t know if others are vaccinated, and some because
people invade their sense of “space” when in public. Some are comfortable continuing
to do things remotely, like using delivery for groceries and meetings online. A
couple of people feel great and are excited, one can’t wait to go out and
“spend the big bucks,” and another shared relief that it isn’t such a crisis
anymore. One person felt the world had turned upside down, that the first are
last and the last are first. He worries we will go back as a society to where
we were before COVID, but hopes we continue to develop. (See Figure 3.)
Figure 3.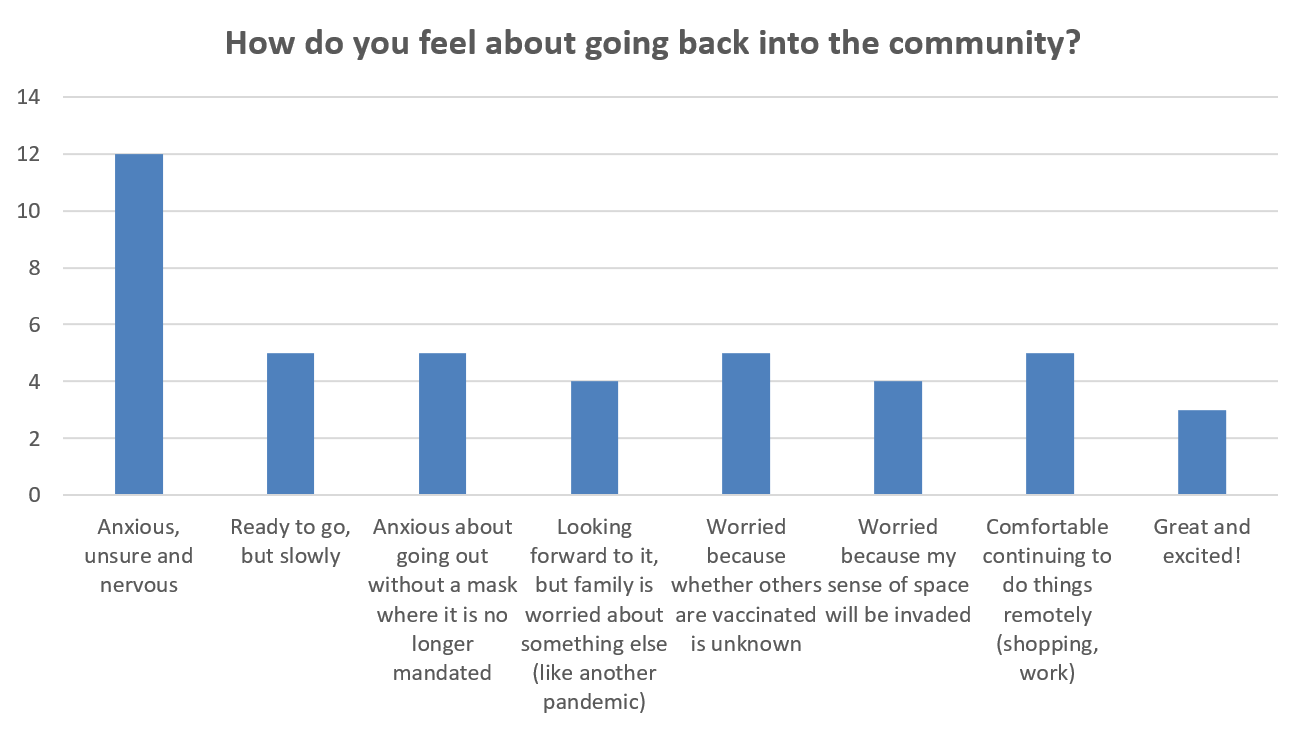
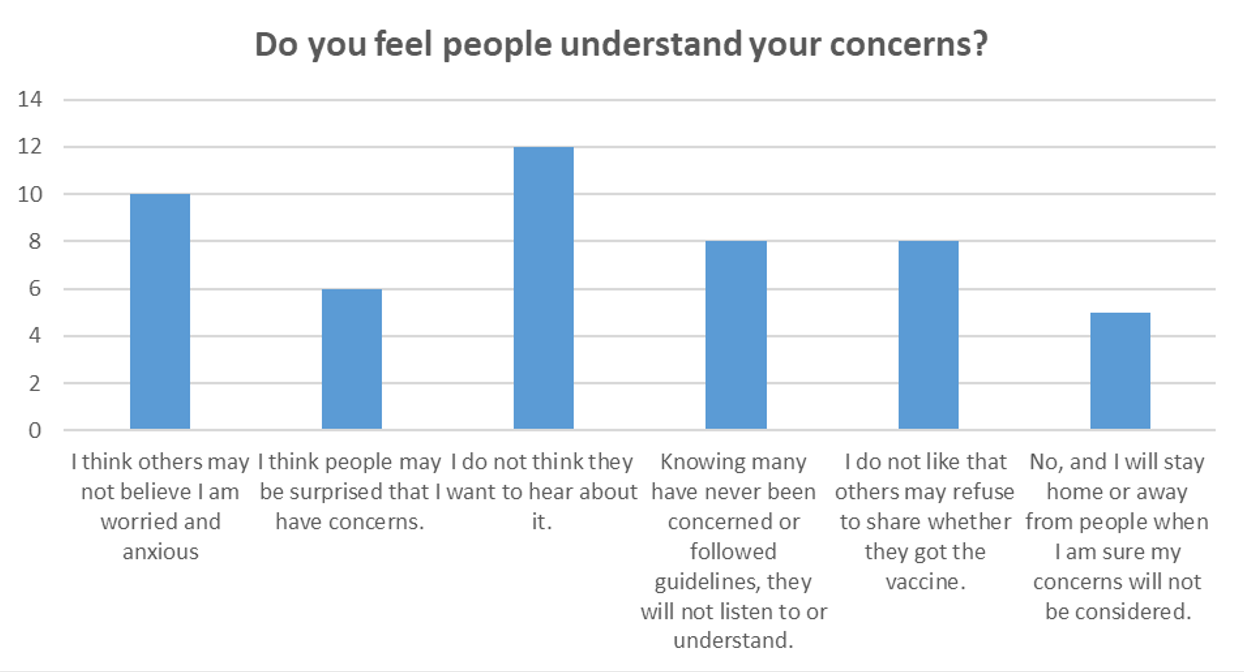
Do you feel people understand your concerns?”
We
at SAU1 feel this is the most important question, because speaking up works
only when people are listened to and heard.
Not surprisingly, the answers show that this is cause for great anxiety
and worry. Many shared that others may not believe those who are worried or
anxious, or may be surprised by our concerns, or just won’t want to hear about
it. For those in rural areas, there are many people who have never been
concerned or followed guidelines which shows that they will not listen to or
understand others’ concerns. There are still people who think COVID was just a
hoax and refuse to listen to science. Some don’t like that family, friends,
staff, and others refuse to share whether they have been vaccinated. Some are
scared about people who did not get the vaccine. One-person shared concern and
bewilderment that some health care workers are choosing not to be vaccinated.
Others are staying home or away from other people when they know their concerns
will not be considered. (See Figure 4.)
Figure 4.
People
with disabilities have many of the same dreams and hopes as most other people,
even as a pandemic starts to wind down. They may be experiencing more worry and
anxiety because of increased vulnerability due to existing health
concerns. In this, as in all aspects of life, each person with disabilities
must be encouraged to speak up, and others must truly listen and give them the
same respect other people have to My Life, My Way.
Contact information
Go to www.sau1.org or email us at info@sau1.org to learn more about us and our work.
Swindle | 43-54
Volume 10 ► Issue 2 ► August 2021
A Win/Win: Using Both
Personal Spiritual Strength to Heal and Experiencing Post-Traumatic Growth to
Heal with a Transition and Reintegration in Sight
Fr. Mark Swindle
Abstract
As human beings, we have the capability that allows us to positively rise to a higher level of functioning because of challenges we face in life. This higher level of functioning can be thought of as a positive psychological change and is not considered a new concept. Early writings and arguments of different faiths and beliefs hold true to the teaching that the general understanding is that suffering, and distress can actually be associated with positive changes in one’s life.1 Post-traumatic growth is often a part of mental health recovery. It is one area that can be identified in supporting mental health recovery and directly associated with spirituality. When an individual, (a patient in this case,) is taking the next step and moving towards transitioning and reintegrating back into the community, their spiritual well-being is integral in the recovery process and just as important at the time of their discharge.
___
Challenges
We all experience both physical and mental challenges throughout time and for most of us, we call this “going through life.” Some of us are faced with more physical aches and pains in our bodies than others. For some of us, we seek the consultation and treatment from a medical physician when we suffer from intense and/or prolonged physical pain. If physical therapy is prescribed, we are told to perform certain exercises to help our muscles grow stronger. This is because the breakdown of muscles invariably leads to their buildup, allowing them to grow stronger. Where/who does one turn to when their soul aches? How does one deal with an “aching” soul? When an individual is challenged with a spiritual related issue, they seek a person who can best relate to their issue at hand. In a hospital, this person is most likely the chaplain. Chaplains can also be considered a physician – a physician of the soul.
We all experience mental challenges time to time and for some, these mental challenges are greater than others and there can be multiple factors that lead to mental illness. As we “go through life,” we know that breakdowns often hurt and the grief that remains is real. There are times in life when we experience great sadness and undoubtedly, mourning is part of life which everyone will undergo. A job of the chaplain is to simply “meet” the patient in whatever place they are at any given time. A chaplain does not always need to provide advice or counseling in every matter. Chaplains are not able to make any sort of judgment calls or sway the patient to any sort of personal beliefs. Chaplains are comprised of all types of individuals and individual beliefs should not become a factor when ministering to patients.
As a Christian chaplain working in a state mental hospital, I can speak for myself that when I provide pastoral care to a patient in the worst trouble, I remind the patient of a few things: that God’s work is secure, God’s will is good, and God’s strength is ours. Those who are suffering with mental illness and who also turn to a “Higher Being” can experience post-traumatic growth as a divine discipline whereby God is producing a deeper faith. I have found that in patients with severe mental illness, the ones who possess some sort of spirituality and have God in their daily lives, have a different, more positive outlook of life. It is as if God draws the individual into a deeper faith-based belief system. It is a patient’s personal faith-based belief system that defies all sense of hopelessness for them and thereby, allows for growth. As a chaplain, I reassure the individual that grief and suffering is a signal of hope, and mourning is just the beginning of growth to come. Chaplains convey the message that an individual needs to focus on the good and those new possibilities are possible and await them upon their transition and reintegration into a new life after the mental hospital. These possibilities are the very result of their lives being turned upside down. When providing spiritual support to an individual, chaplains will often talk about the spirituality of suffering. Within the realm of spiritual suffering, a chaplain assures the patient that we are not called as human beings to seek or desire pain in our lives.2 We further talk about how having a positive spirituality of suffering in place can help when the opportunity comes their way to face the difficult challenges of life and, in confronting them, they will be able to find what God is saying to them in ways they may not have understood or valued previously.
Mr. C. is a patient in the hospital that I met a little over a year ago. One duty I perform as a chaplain is to perform an initial spiritual assessment on a patient when they are admitted. Upon speaking and assessing Mr. C., I sensed immediately that he had strong and healthy spiritual strengths within him. Mr. C. currently attends every one of the spiritual group sessions I offer as well as Sunday Worship Services. He loves to sit and talk one-on-one about spirituality and God. One day while I was talking with Mr. C., he began to share with me about how he enjoys reading anything he can get his hands on about any religious topic. As I got to know Mr. C., he began to share more and more with me about his mental illness. He understood and knew exactly why he was in the hospital and the plan he needed to follow to be discharged. Mr. C. told me that he was not proud of what he had done previously in his life that resulted in him being admitted to the hospital. He shared with me that of all things that accounted for his mental illness, one of them was a wrong done by the church. I did not completely understand what he meant until he elaborated more. Come to find out, it was through the teachings of Mr. C.’s faith denomination within his local church that he began to take the teachings more and more literally until it caused him to change his entire belief system about God and the world. Being a chaplain in a mental hospital, I have occasionally had patients who take the Bible in the most literal sense. And so, while leading a good spiritual life in his local community, according to Mr. C., he began to suffer more and more. He began to plunge into a spiritual darkness because of the fact others were telling him exactly how he should believe. He was basing his religious beliefs on how others believed, rather than making religion part of what he believed. It is now, while in the hospital, that he is beginning to obtain a healthier perspective on his spiritual well-being. He has the opportunity, through time, to explore his inner self and understand that everything in the Bible cannot be taken in the most literal sense. Mr. C. views his mental illness as going through a spiritually dark period and that he can appreciate, amidst this darkness, that now he is able to emerge stronger. It is through the darkness that a new spiritual light is being illumined and he can start fresh and have a new beginning once he is discharged. I asked Mr. C. why he feels this way. It is certainly a challenge to him, that, by being hospitalized, he has called himself to gain a new perspective on his life and his faith. He is more grateful for what he has because of the positive ways he views himself. He can deal with illness more willingly when it comes in his life. In other words, how Mr. C. views himself and those around him, and all situations in between, is more important to him than what he is viewing or what he was forced to believe previously. How he reads and studies his Bible with the guidance of a chaplain and the information he learns by attending spiritual-related groups have provided him with new perspectives on his faith-based beliefs. Mr. C. views his spirituality in a more positive way now than previously. As the chaplain, I did not change Mr. C.; rather, he changed himself. Mr. C. has stated numerous times that he would like to become a chaplain some day or some sort of counselor that helps others in their struggles. Mr. C. feels he would be able to help others because he has gone through similar struggles in his personal life.
Keys to Success
Post-traumatic growth is positive psychological change experienced as a result of adversity and other challenges in order to rise to a higher level of functioning3. Post-traumatic growth includes “life-changing” psychological shifts in thinking and relating to the world. These shifts contribute to a personal process of change that is extremely meaningful. Some of the outcomes that have been seen in individuals that have experienced post-traumatic growth include some of the following: greater appreciation of life; changed sense of priorities; closer, more intimate relationships; greater sense of personal strength; and recognition of new possibilities and choices for one’s life and spiritual development4. The chaplain’s job is to encourage and foster the growth of an individual’s confidence and self-esteem arising from the struggle with adversity. The chaplain will remind the patient that they must remember to keep spirituality in the forefront of their recovery process once they are transitioned and reintegrated into society. Specifically, the patient’s spiritual growth and development will aid them in the following:
- Changes in how they relate to other people
- Recognition of new opportunities, priorities, or pathways in life
- Greater appreciation for the value of one’s own life (and life in general)
- Recognition of one’s own strength
As a chaplain, I consider all the above as being important in an individual’s spiritual growth and development. I continuously remind my patients that they are every bit as capable of strengthening their spiritual lives and their belief system and that they will be strengthened from their struggle.
Chaplains use their own life experiences when meeting with patients and convey to the patient what value there is in considering the potential of their personal growth as the result of suffering. Chaplains try to have the patient think, that even in the aftermath of negative events in their life, that there may be value that will follow. As a chaplain in a hospital where the patients are mentally challenged, it is common to hear them say that they feel like life will never be the same again once they are discharged. Those that possess strong spiritual strength will see for themselves that they have grown stronger, and they will be able to use this strength in the future. As chaplains, we remind the patient that they do have the ability to transition and reintegrate themselves back into society and to lead a fulfilling and a positive life again. We remind them that, through their personal experiences, they now possess wisdom.
Some chaplains use the phrase of “finding a meaning in hell” or, “going through a spiritual desert” when talking to a patient about their past or even, their present. A patient’s “hell” and “desert” are words that are used to describe anything traumatic and horrible they are or have gone through in their lives. One patient I meet with on a regular basis is Miss W. I see Miss W. at least twice a week when she participates in my spiritual group sessions, one-on-one meetings, or Sunday Worship Service. In worship service, she always sits in the front row and is always the first to volunteer to take a reading part. During the testimony and sharing portion of the service Miss W. often attributes her current state of peacefulness and happiness because she continuously reflects on what going through the “spiritual desert” means in her life. Miss W. admits her childhood was not a happy one due to what she considers mental abuse by close family members. She further stated that her teenage and early adulthood years were not so good because of the same reason. She feels like she made many “walks through hell” in her life and had been stuck in many “spiritual deserts.” Miss W. admits, that because of enduring them, she is the person she is today. Miss W. feels that she has experienced growth at so many levels in her life which she feels bears witness to her strong spiritual strengths. Because of the nurtured faith-based belief system she obtained in the hospital, she now feels that she is a “changed for-the-better” person and as a result, now has an enormous capacity to overcome problems in her current day-to-day life. Upon performing Miss W.’s initial spiritual assessment, this was certainly not the case. She displayed very few signs of spiritual strength at all. For me, it was not surprising after hearing the sort of mental abuse she previously experienced. My job is to encourage Miss W. and build confidence in her that she has the potential to grow from her past negative experiences. While she cannot change her past, she can certainly change her future. I am a witness to Miss W.’s changed outlook during her stay in the hospital by the way she now participates in our discussions and the enthusiasm she shows in worship services. Her spiritual strengths far outweigh her spiritual weaknesses. Just as Mr. C. in the previous scenario, Miss W. attributes her road to recovery and success are direct results of her spirituality and strong belief in God (her Higher Being.) She understands that even though her past may have been negative due to other individuals’ actions and not being shown the love she so desperately longed for, she can now find that person that loves her unconditionally – God! Miss W. understands that while she cannot change the past or the individuals in her past, she is able to change herself! Through spiritual groups she has learned to take control of her thoughts and can actually choose which thoughts to have. She chooses positive thoughts! This is growth! Miss W. is currently waiting for a spot to become available in a group home and once it does, she is excited to be discharged from the hospital and begin to lead a healthier and more productive life in serving others. She is overcome by joy with the anticipation that this will become reality for her soon.
Conclusion
Regardless of how a patient has changed because of mental illness or where he or she stands on the path of life, the chaplain can help with their journey back to society. Many times, the local community religious leaders, rather than the health care providers, may be the first point of contact for an individual who may be struggling with their return to society. Chaplains can play a vital role in educating their community colleagues about challenges that may confront the individuals as well as services that can provide additional assistance. Many times, a chaplain is asked to research and find a local church in the place the patient is being discharged to. This is a sign that the patient intends, or at least, is thinking about, a place where they can continue their spiritual journey.
Chaplains are there to provide a comfort to those seeking help or sharing hardships. The goal is to help facilitate the transition to the normal rhythm of life, assist the individual with defining his or her new “normal,” as well as supporting the family while the transition is taking place. This includes, but is not limited to, helping the individual feel comfortable, valued, understood, and fully integrated into the community and family. Especially important is assisting the individual to move on with their lives and to enjoy the happiness that they have earned and deserve.
As a chaplain I can offer the patient the following piece of advice. The advice is this: that they have a choice - they can simply stand at the threshold of the opportunity to change and grow after a traumatic experience, which results in incessant complaining about all that happened in their previous life - or - they can take advantage of the opportunity to walk through the spiritual threshold to a new life. I remind them that this is up to them to decide for themselves, and the opportunity is there for them to take. Carl Jung has a powerful quote that I often like to use. He states that, “Your visions will become clear only when you can look into your own heart.” He furthers explains that “Who looks outside, dreams, who looks inside, awakes5.”
Steve Taylor, in his book, Out of the Darkness: From Turmoil to Transformation, sums it up perfectly as he writes,
“There will always be some degree of
suffering in our lives and when it comes, we should not try to see it wholly in
negative terms. We should always be aware that, buried inside it, there is an
opportunity for growth and transformation…Beneath the terrible, painful surface
there is a massive reservoir of spiritual potential…Spiritual awakening exists
as a potential inside everyone. It is just that normally the potential is
dormant. To manifest itself, it normally has to be triggered by turmoil and
trauma6.”
All of us have experienced at the very least one, if not multiple, types of transformational situations in our lives and it is often as a result of some sort of traumatic life event. Consequently, we were forced out of our “normal” way of thinking and behaving. Some of us work through these transformational situations in different ways than others. For many, the situations produce negative long-term impacts that lead to mental illness. When dealing with an individual, I try to provide the assurance that I understand that trauma is essentially negative; however, by persevering through the traumatic experiences, I make sure to ask them if they have come to a new and more informed meaning of themselves and life. And if so, that their new experiences are positive. My aim is not to push the patients to experience growth. The result I look for is for the patients to simply be aware and informed of the positivity that can follow because of their strong spiritual strengths. The silver lining is that, even as horrible as life’s situations are, it is certainly possible that a patient with mental illness can be equaled with positive long-term outcomes. By using both personal spiritual strengths to heal and by experiencing post-traumatic growth, an individual certainly has the potential to succeed. When an individual has the skills, courage, and the patience to face the terror and find a way to experience it and accept it, success awaits them as they transition and reintegrate into society over time. This is a win/win.
References
1. Lees AB. Posttraumatic growth. Psychology Today. https://www.psychologytoday.com/us/blog/surviving-thriving/201904/posttraumatic-growth. Published April 18, 2019. Accessed May 2, 2021.
2. Catechesis E&. Posttraumatic growth and the spirituality of suffering. USCCB. https://www.usccb.org/news/2020/posttraumatic-growth-and-spirituality-suffering. Published September 8, 2020. Accessed May 10, 2021.
3. Post-traumatic growth. Wikipedia. https://en.wikipedia.org/wiki/Post-traumatic_growth. Accessed May 10, 2021.
4. Tedeschi R, Calhoun L. Tempered by fire. Psychology Today. https://www.psychologytoday.com/us/blog/beyond-resilience/201309/tempered-fire. Published September 24, 2013. Accessed June 3, 2021.
5. Jung C. Trauma, spirituality and post-traumatic growth. Your Strength to Heal. https://strengthtoheal.org/trauma-and-spirituality/. Published December 9, 2014. Accessed June 15, 2021.
6. Taylor S. Post-traumatic growth and spiritual awakening. Spacious Awakening: Randy Compton, M.A. http://spaciousawakening.com/articles/post-traumatic-growth-and-spiritual-awakening/ . Published March 29, 2021. Accessed June 20, 2021.Biography
The Very Reverend Fr. Mark Swindle earned a Bachelor of Arts Degree in Slavic Languages and Literature and Germanic Studies and Linguistics from Indiana University in Bloomington, Indiana in 1993. Having worked in the corporate world for nearly 15 years he received the calling to pursue an ecclesial path to serve others in a more profound way. He entered the seminary and graduated with a Master of Divinity Degree from St. Sophia Ukrainian Orthodox Theological Seminary in New Jersey and ordained to the priesthood in 2011. Fr. Mark is assigned as the pastor of The Protection of the Holy Virgin Ukrainian Orthodox Church in Pittsburgh, Pennsylvania where he currently serves the congregation. In addition to being a pastor, he participates in local community outreach programs and speaks at various pastoral events around Pittsburgh. In 2014, Fr. Mark enrolled in the Chaplaincy Program at the VA Pittsburgh Healthcare System in Pittsburgh, Pennsylvania where he completed four units of Clinical Pastoral Education which totaled over 1600 hours. Fr. Mark became a Dual Board-Certified Chaplain in October 2016 from The Association of Certified Christian Chaplains, Orlando, Florida and then in January 2018 became dual board certified from The Spiritual Care Association, New York, New York.
In 2015, Fr. Mark joined the Spiritual Support Department at Torrance State Hospital (TSH) in Torrance, Pennsylvania where he presently provides his service as a Chaplain. TSH is a dynamic, treatment oriented, psychiatric facility that emphasizes thorough and accurate assessment and individualized treatment based upon contemporary evidence-based practices and encourages patient participation in their ongoing Active Treatment Program. Patients are active partners with Treatment Team members in the development of individualized treatment plans and active treatment schedules. Over 150 different types of groups have been developed to provide programming at various times and days of the week to afford patients the opportunity to have treatment that is individualized to meet their needs, as well as interests. Spirituality Support Groups are very popular among the patients’ daily schedules. Fr. Mark facilitates daily spiritual support group sessions for the patients, one-on-one individual sessions as well as leads weekly worship services. He provides pastoral care to all of the divisions of the hospital including the Civil Units, Forensic Units and the Sexual Rehabilitation Treatment Program (SRTP) Units.
Contact Information
Fr. Mark Swindle, Chaplain
724-459-4555
Zortman, Morris, & Vivaldi | 55-66
Volume 10 ► Issue 2 ► August 2021
Use of Remote Monitoring to Positively Impact Individuals by Removing the Struggle Between the Person and Their Supports
Anne Zortman, MS,
Timothy W Morris, and Meredith Vivaldi
Abstract
A common misconception in the field of Intellectual and Developmental Disabilities (IDD)/Dual Diagnosis is to automatically add supports and services when someone is engaging in maladaptive behaviors. However, for someone where the impetus for maladaptive behavior is driven by control and creating chaos in their environment, less support can be more impactful in effective change. This article will review how remote monitoring and other positive strategies can be implemented to support a person with Borderline Personality Disorder and IDD to remove the struggle taking place between the person and his supports.
[Borderline
Personality Disorder] occurs in the context of relationships. Unlike other
psychiatric diagnoses, if you put someone with schizophrenia on an island all
by themselves, their mental illness would still be evident. If you put someone
with BPD on an island, you wouldn’t necessarily see the symptoms — whatever
happens, happens in the context of [interacting] with someone else.
--Dr. Perry Hoffman1
___
Introduction
Supporting people diagnosed with both intellectual disabilities and mental health disorders often presents unique challenges. Those challenges can be increasingly complex when a personality disorder is present. The symptoms of personality disorders materialize in the context of relationships. More specifically, Borderline Personality Disorder is marked by interpersonal disturbances2. People diagnosed with Borderline-Personality-Disorder inherently display more argumentative, antagonistic, and less cooperative behaviors3. These behaviors can create barriers to functioning in social relationships, including relationships with those in a supportive role3. When a person engages in ongoing discord and hostility in their interactions with supportive services, the unique challenge becomes maintaining the therapeutic value of the support without becoming the source for conflict. This dynamic calls for an inventive approach to find that balance.
Case Study
Grayson was adopted at 14 months of age; however, not much else is known about his life prior to age 13. At the age of 13, he began a series of psychiatric inpatient hospitalizations and ongoing psychiatric care. During this time, he was diagnosed with mild intellectual disability (ID), borderline personality disorder (BPD), anxiety disorder (AD), and bipolar disorder (BD). When Grayson became an adult, he received services from multiple agencies, often changing providers as the result of unsuccessful discharges. His services varied from living in community homes to living independently with In-Home and Community Supports services. Grayson displayed a consistent pattern of high-risk aggressive behaviors including property destruction, physical assault, terroristic threats, and allegations against supporters. Although he is articulate and is independent across many areas of functioning, he could not effectively navigate or maintain healthy social relationships, including those with his adoptive family His relationships were marked by his volatile reactions to perceived mistreatment or lack of respect. These perceptions resulted in acts of vengeance in the form of physical aggression, homicidal threats, and allegations of abuse or neglect. In 2016 at the age of 35, Grayson was placed on probation for making terroristic threats. During this time he also returned to the care of his adoptive brother after being discharged from a community home due to physical and verbal aggression. Although he reports that he very much valued his relationship with his brother, he was not able to maintain a healthy relationship with him and manifested old patterns of behavior. He threated to “shoot up” his brother’s home and was incarcerated for 30 days following this threat. The court recommended that he be placed in a community home to address his ongoing behavioral support needs. Grayson moved into a community home in July 2018 but by June 2019, the provider determined they were no longer able to support him. He then chose to move into a community home with Person Directed Supports (PDS).
When Grayson started services with PDS, he presented with his historical behavioral patterns of verbal and physical aggression, terroristic threats, property destruction and allegations against supporters. An initial functional behavioral assessment was completed during his first 60 days of service with PDS. This initial assessment involved direct observation of Grayson by the behavior specialist, interviews with Grayson and his supporters, review of records related to his psychosocial and developmental history, and review of behavioral data collected daily by support staff. Behavioral data collected included the time each behavior occurred, duration of the behavior, what had occurred prior to the behavior, description of actual behavior, strategies used to address the behavior, the response to strategies, anything else that was effective in de-escalating the behavior, and what Grayson did once he was deescalated. The initial Functional Behavioral Assessment indicated that Grayson’s maladaptive behaviors serve social functions in the form of obtaining attention and escape/avoidance. Social attention was the most common outcome of his various provocative and threatening statements and the severity of his statements increased when attention was not immediately given. He also effectively utilized physical aggression and elopement to escape non-preferred situations and tasks. After several months of continued observation of Grayson, ongoing interviews with supporters, and analysis of the behavioral data, themes around his behaviors became evident. He sought control and a feeling of power in his dynamics with others and that interpersonal conflict with supporters facilitated that sense of control. He displayed hypervigilance against perceived mistreatment or not being respected by supporters. It was hypothesized that Grayson operates from a core belief that he lacks worth and will not be respected. The behavioral data indicated that he was creating this narrative with his direct support staff and it was evident that adding additional support resulted in increased conflict. In an effort to reframe how he views supports, our team at PDS began looking into ways to change the role of supporters and to change the form of supervision without reducing the level of support Grayson would require. Our goal was to shape supports in a way that he could value the relationship with his supporters instead of seeking conflict with them.
Initially, Grayson moved into a home with two other individuals and received 2:1 staffing supports. He immediately struggled sharing his living environment and expressed his desire to live more independently. He made ongoing attempts to turn support staff against one another to create discord. Police involvement, psychiatric inpatient hospitalizations, and numerous self-reported allegations of abuse and neglect increased. To mitigate the conflict, Grayson moved into a 1-person community home with PDS, and staffing supports were reduced to 1:1. Despite the change in environment and level of support, he continued his pattern of dysfunctional interpersonal dynamics. Supporters grew wary of working with him due to frequent self-reported allegations and investigations that required supporters to be on leave. It was evident that a different approach in supporting Grayson with his complex behavioral needs and strong desire for independence was needed. We hypothesized that continued reduction of in-person supports, while still accounting for safety, would lead to a balanced situation where he could focus on living his life independently and remain receptive to help from supports in doing so. This led us to investigate using technology to aid in supervision and reduce the amount of in-person support provided.
An independence plan designed to incrementally build up to remote monitoring was developed and proposed to Grayson. We also collaborated with our administrative entity, supports coordination organization, Pennsylvania’s Office of Developmental Programs’ (ODP), and state licensing staff to finalize the details of the plan. The plan started with staff engaging in active and passive staffing at varied timeframes to simulate the conditions of remote monitoring without removing staff from the property. During passive staffing conditions, staff remained in a designated area of the home and would only interact with Grayson if there was an emergent need. The intention of the incremental plan was to slowly back away in-person support without sudden change as transitions can be a trigger for him. Having staff remain on site but in a passive mode that was not accessible to Grayson created an unintended power struggle between him and staff likely due to perception of abandonment as the staff are still in the home but not interacting with him. This was an important observation, further confirming his interpersonal distortions and functions of his behaviors. The incremental nature of the initial plan also was difficult for him to follow and predict as there were contingencies attached. Multiple steps prevented him from settling into the plan and kept his focus on the power struggles and changes versus making progress and skill acquisition. The focus remained on chaos in relationships. In order to address Grayson’s continued desire for full independence while also considering his need for clear, predictable relationship boundaries, we created a more concrete, structured plan that went directly into remote monitoring.
The remote monitoring plan combined
direct in-person supervision with off-site virtual supervision. To achieve
this, video cameras were installed near the ceilings in all common areas of the
home. Cameras were not installed in the bedroom or bathroom. Video was provided
continuously but not recorded. During remote monitoring hours, support staff
monitored the video feed at another home located approximately 15 minutes from
Grayson’s home. Grayson was also able to access supporters on a cell phone
designated for calls during times of remote monitoring. To develop the schedule
for in-person supervision hours in the home, multiple factors were considered.
The in-person hours needed to be during times when Grayson would want to
participate in activities inside and outside of the home and when it made sense
to have a supporter present to assist with tasks. The behavioral data was reviewed
to ascertain if there was an average length of time supporters were able to
work with Grayson before maladaptive behaviors occurred. Based on these
considerations, it was determined that he would receive a total of 8 hours of
in-person support each day. The 8 hours were divided into three separate
in-person shifts: 5:30 AM-7:30 AM, 11:00 AM-2:00 PM, and 5:00 PM-8:00 PM. These
timeframes encompassed medication administration times, his preferred times for
meals, and times when he would typically want to go out into the community. If
appointments were not able to be scheduled during the set in-person support
hours, supporters would leave the remote monitoring site to provide
transportation and assist with the appointment. After the appointment, he would
be transported home and supporters would return to the remote monitoring site
until the next in-person support time. Grayson often stated a desire to live
more independently. When developing the remote monitoring plan with him,
emphasis was placed on how replacing in-person supports with remote supports
created an environment for him to build those independent living skills while
supporters were not in the home with him. This helped him buy into the plan. Again,
we collaborated with the administrative entity, supports coordination
organization, ODP, and state licensing to ensure the team was in agreement and
all factors had been considered. Maintaining ongoing communication with this
larger team was vital to implementing the plan.
When the remote monitoring plan was launched, Grayson’s behaviors demonstrated a near immediate change. (See Figure 1 and Figure 2.)
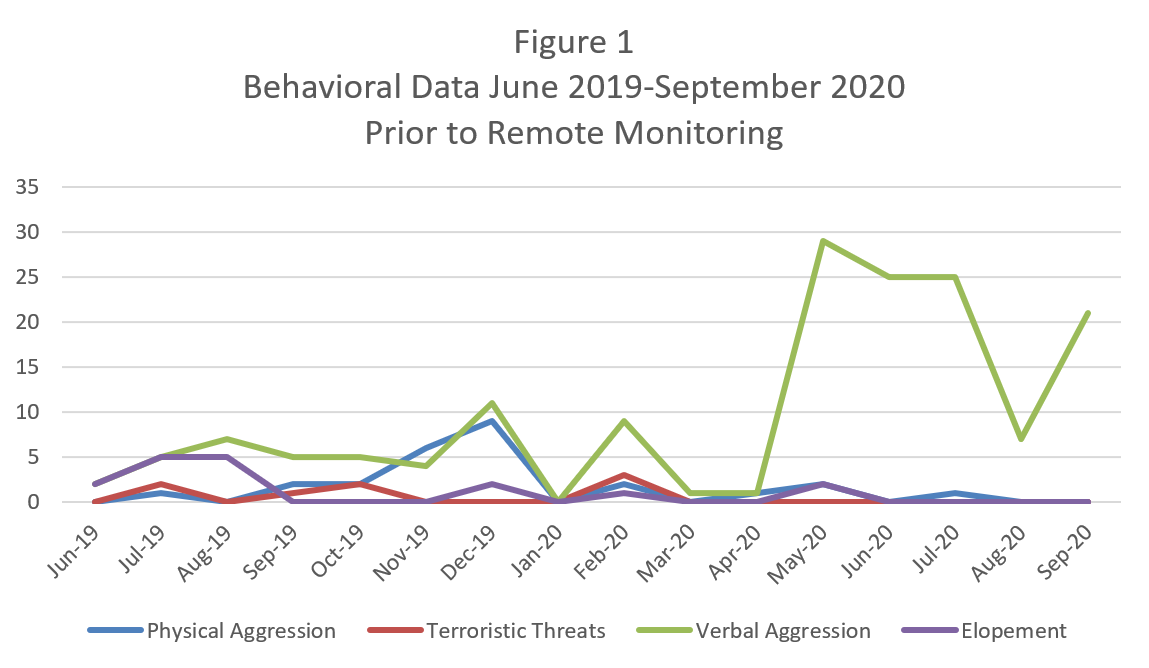
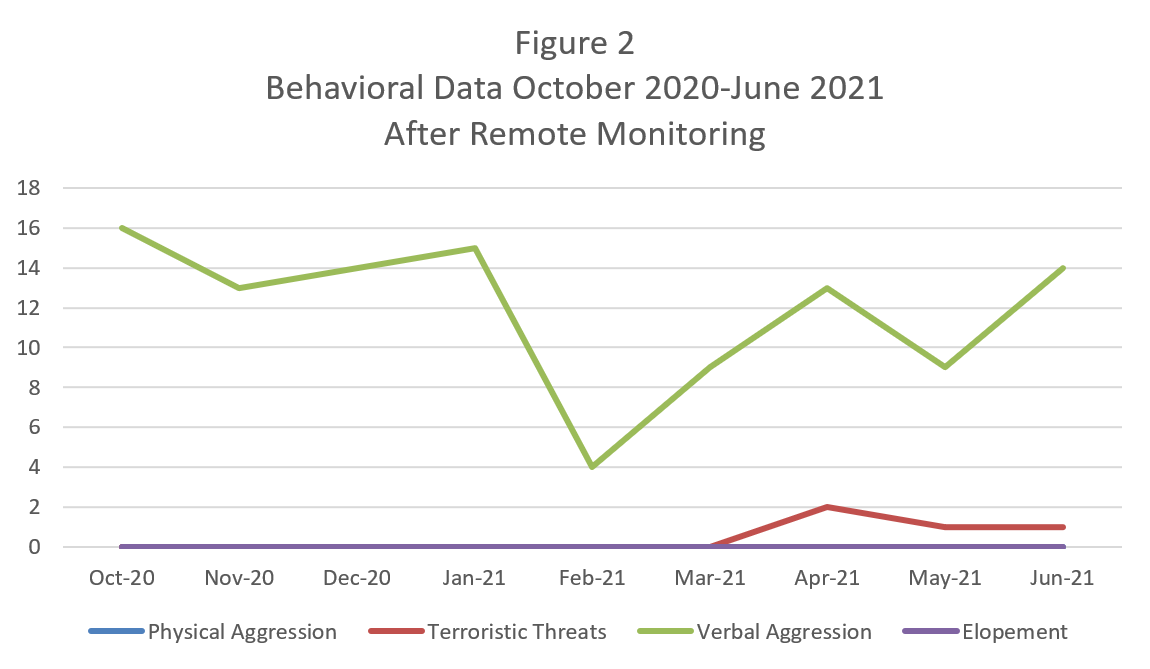
He stopped all terroristic threats toward his direct support staff. He no longer engaged in property destruction, eloped from the home, or made threats to harm himself. In the 9 months since the remote monitoring plan started, he has only engaged in physical aggression on one occasion and it was noted that this occurred during a period when staff were not able to utilize remote monitoring and had to implement the passive staffing schedule while on the property. Grayson continued to utilize some provocative language with the suspected function to obtain a reaction from his supporters. Instead of verbal threats to harm supporters, he shifted to making sexual comments, often in the form of jokes or songs, to see how supporters would respond. Supporters were consistently successful in redirecting him from his commentary and in-person staffing hours have been used with more intention and purpose. Interestingly, Grayson did not completely shed his narrative around his perception of not receiving respect and his related need to retaliate against that perception. He shifted his focus to members of the management team within PDS. This manifested in ongoing unsubstantiated allegations against those team members but not allegations against his supporter. In making PDS administrators the focus of his discontent, he has been more successful in navigating relationships with his supporters and building skills and interests that foster his independence. As intended, use of remote monitoring helped remove the conflict between Grayson and his supporters and created an opportunity for him to value his supporters in a way that had not previously occurred to him.
Conclusion
Grayson’s story demonstrates the
opportunity for increased innovations in supporting individuals with complex
behavioral presentations. High risk behaviors often seen in people with
Borderline Personality Disorder are rooted in social function and present a
unique challenge as the physical presence of support often provides the trigger
as well as the reinforcement. Additionally, these high-risk behaviors can
prevent an individual from achieving levels of independence they are otherwise
capable of achieving, resulting in increased frustrations with the levels of
support in place and making the supporter the target of that frustration. It is
often the case that as high-risk behaviors increase, the presence of support
also increases. With Grayson’s diagnosis of borderline personality disorder,
this only exacerbated his feelings of resentment toward his supporters and lead
to behaviors that not only stunted his progress but put him and his supporters
at further risk of harm.
The collaborative efforts of the state administrative entity, supports coordination organization, ODP, and licensing were key in designing this plan. Team meetings were held while designing the plan and then quarterly meetings were held once the plan was implemented. Email updates were also provided on an as needed basis. Keeping the team informed each step of the way ensured we were all on the same page and could problem-solve from an informed place. Taking a person-centered approach in addressing Grayson’s complex needs proved paramount to the overall success of the remote monitoring. Seeking to understand Grayson rather than participate in his narrative of opposition and conflict led to an outcome where he is able to engage in supportive services without putting himself or others at risk of harm. This experience is an example of not only how remote monitoring can be used to enhance the independence of people in supportive services, but also how it can restructure services for those who struggle with the interpersonal dynamics of support.
References
1. Villiant M. Most accurate article on BPD we have read—kudos. Borderline Personality Disorder.org website. https://www.borderlinepersonalitydisorder.org/most-accurate-article-on-bpd-we-have-recently-read-kudos/. Accessed June 10, 2021.
2. Hoffman
PD, Fruzzetti AE, Buteau E. Understanding and engaging families: an education,
skills and support program for relatives impacted by borderline personality
disorder. Journal of Mental Health 2007; 16 (1): 69-82.
3. Schmahl C, Herpertz SC, Bertsch K, et al. Mechanisms
of disturbed emotion processing and social interaction in borderline
personality disorder: state of research
agenda of the German clinical research unit. Borderline Personality Disorder
and Emotional Dysregulation 2014; 1(12);1-17. https://doi.org/10.1186/2051-6673-1-doi:10.1186/2051.6673.1.12. Published: September 2014. Accessed: June 10,
2021.
Biographies
Anne Zortman, M.S. is the Clinical Director of Behavioral Health Services for Person Directed Supports, Inc. She earned her Master’s in Clinical Psychology at Millersville University. Anne has worked in various areas of the mental health system including Adult Community Living Arrangements, Partial Hospitalization, Outpatient Therapy, and Behavioral Health Rehabilitative Services.
Timothy W Morris, graduated Manga Cum Laude from Shippensburg University with a Bachelor of Science, Major in History, Minor in Psychology. He has worked with adjudicated youth, as a Crisis Counselor at the Carlisle General Hospital, and has been with Person Directed Supports for over 19 years working with individuals with IDD and Dual Diagnosis. He also has two amazing sons, Layne and Tristan, who help him hone his behavior modification techniques as they continue to grow into fine young men.
Meredith Vivaldi is the Executive Director of Person Directed Supports. She has been with PDSI for almost 8 years and in the field for over 20 years. Meredith started working with children with varying disabilities and then moved into the adult population with PDSI. She is National Association of Developmental Disabilities (NADD) certified and specializes in dual diagnosis individuals. Outside of work Meredith enjoys traveling and being with family.
Contact Information
Anne Zortman
azortman@persondirectedsupports.com
717-729-3388
Tim Morris
tmorris@persondirectedsupports.com
717-372-8540
Meredith Vivaldi
mvivaldi@persondirectedsupports.com
610-509-7115