Positive Approaches Journal, Volume 10, Issue 3
| Site: | My ODP |
| Course: | My ODP |
| Book: | Positive Approaches Journal, Volume 10, Issue 3 |
| Printed by: | |
| Date: | Sunday, June 28, 2026, 1:45 PM |
Positive Approaches Journal | 5

Volume 10 ► Issue 3 ► November 2021
Beyond Silos:
Highlighting Multisystem Approaches in Pennsylvania
Introduction
Many people who have complex needs require thoughtful, creative, and integrated supports that entail out-of-the-box thinking and cross-system collaboration. To that end, Pennsylvania’s Office of Developmental Programs and Office of Mental Health and Substance Abuse have made a commitment to strengthen existing and viable models and initiatives while also exploring additional opportunities, including funding prospects, that could bolster innovative approaches to meet people’s needs. This issue will focus on ways that Pennsylvania has endeavored to better understand and meet the needs of people with complex needs, including children with medical complexities and/or behavioral health needs, and offer an overview of cross-office capacity-building efforts supported in part by the Money Follows the Person (MFP) funds. Finally, this issue will provide overviews of peer support services as a viable support model and of the PA Care Partnership philosophy of System of Care (SOC) as a foundation to build behavioral health supports and services for children, youth, young adults, and their families. These efforts are worthy of highlighting as we strive to get better at supporting individuals with intellectual disability and/or autism (ID/A) and individuals with mental health conditions in Pennsylvania.
Kristin Ahrens
Deputy Secretary, Office of Developmental Programs (ODP)
Kristen Houser
Deputy Secretary, Office of Mental Health and Substance Abuse Services (OMHSAS)
Positive Approaches Journal | 6-11
Volume 10 ► Issue 3 ► November 2021
Data Discoveries
The goal of Data Discoveries is to present useful data using new methods and platforms that can be customized.
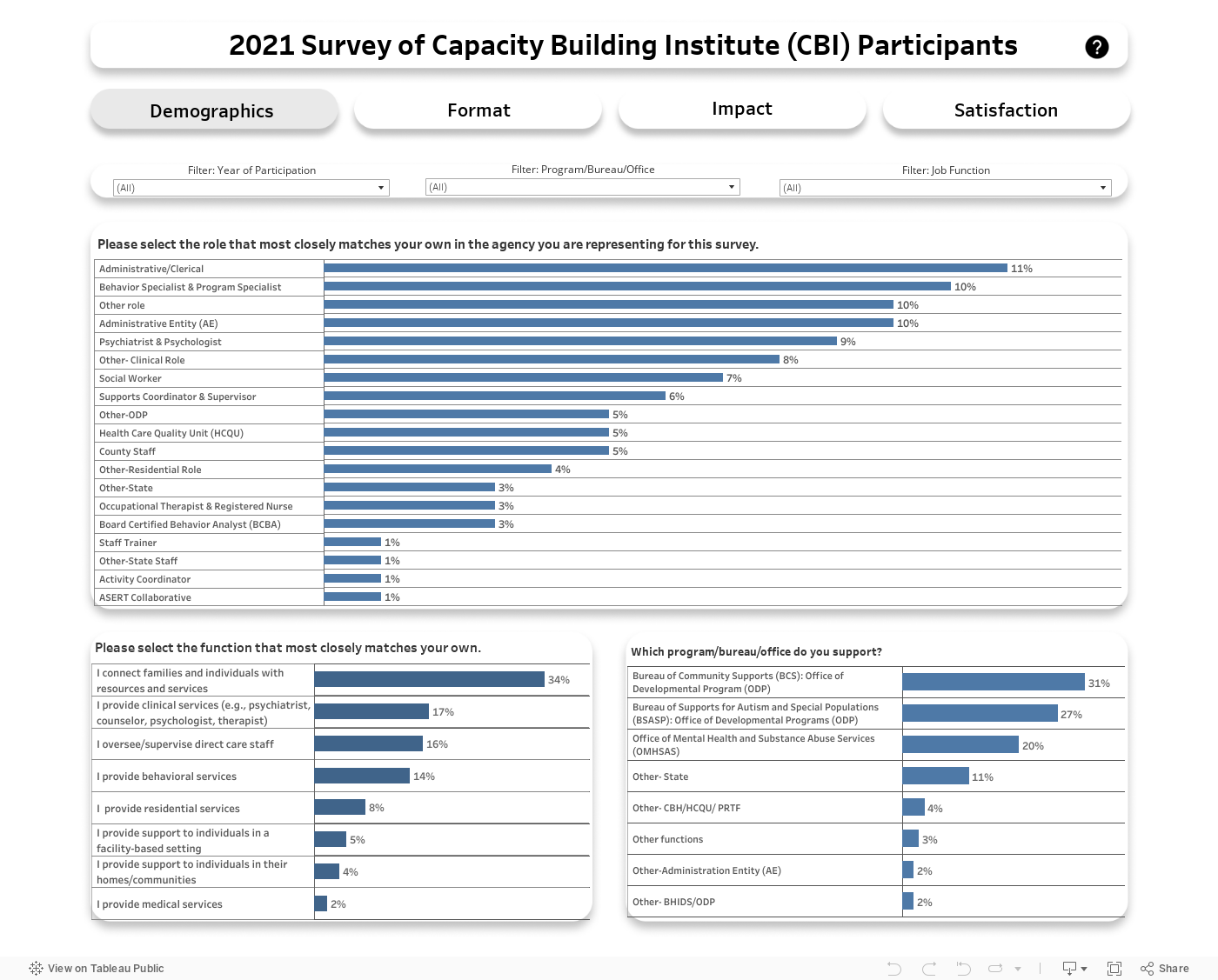
State initiatives to bolster the preparedness of state entities to train and deliver information and resources to staff are critical to building and maintaining optimal systems of care. In Pennsylvania, the Capacity Building Institute (CBI) offers professionals
from many systems in Pennsylvania supporting individuals on the autism spectrum, those with intellectual and other disabilities, and individuals with mental health diagnoses the chance to connect with other professionals, forming networks and teams
to address complex issues. Since the first cohort of CBI participants enrolled in 2016, cross-systems opportunities for professionals to engage and expand knowledge on promising practices, problem-solving strategies, resource sharing, and supporting
individuals with complex needs have emerged and grown. CBI participants attend a two-day per month intensive educational seminar over the course of nine months focused on a myriad of topics including trauma, behavioral assessment, self-care, sexuality,
and therapeutic modalities. CBI is one initiative funded by the Money Follows the Person (MFP) demonstration project and has led to collaboration between the Office of Developmental Programs (ODP) and the Office of Mental Health and Substance Abuse
Services (OMHSAS).
To learn more about the impact of CBI on attendees and how CBI has impacted their ability to perform their jobs more successfully as well as satisfaction with CBI overall, a survey was distributed to previous participants from the first four cohorts of CBI. Over 100 CBI participants completed the survey, representing more than half of those who participated. Survey respondents represented a diverse cross section of Pennsylvania service systems and representation across roles and job functions. The data dashboard below shows results from the survey.
Conclusion
For more resources and training to support the capacity building for professionals, visit the ASERT Collaborative’s LANTERN (Learning Assistance iNstruction Training Education Resource Network) eLearning platform: www.paautism.org/elearning/. There will you find courses on critical topics including mental health diagnoses, psychopharmacology, and neurodiversity. You can also contact the ASERT Collaborative Resource Center (info@paautism.org or 877-231-4244) to request a free, tailored training for your organization.
Hogan | 12-23
Volume 10 ► Issue 3 ► November 2021
Going Home: Children with Medical Complexities Cross System Successes
Heidi Arva & Jennifer Harniman-Crangle, LSW
Abstract
Early in the summer of 2018, interest around a new initiative emerged within the Office of Developmental Programs (ODP). The intent of the initiative was to support children with medical complexities residing in pediatric facilities by exploring our current system, learning more about existing services, and collaborating with other systems within the Department of Human Services (DHS) to support children to be able to return home to their families rather than grow up living in facilities. As the work began it became apparent that this initiative would require the support and involvement of multiple systems to achieve success.
Identifying the need
The initiative to support children with medical complexities began with the recognition that although Pennsylvania’s Office of Developmental Programs (ODP) was licensing some pediatric facilities, the details of their care needs were unknown to the office. Although many of these children would be eligible for services in the ODP system, they were not yet registered with county Administrative Entities (AE) and therefore ODP did not have individualized support plans for each child. We did not know what was important to them, their likes and dislikes, medical and developmental needs, their goals, and so on. It was identified that several of the children had been residing in facilities for years. Children were growing up in facilities.
The Office of Developmental Programs believes that everyone should have an opportunity to live an Everyday Life1. “People with disabilities have a right to a life; a life that is no different than that of all other citizens. 1” Through this we value what is important to people; their rights, responsibilities, relationships, and opportunities to have a valued role in their community and contribute to society in a meaningful way.1
Although most individuals supported by ODP are adults, we hold these values not just for adults, but for all people across the entire lifespan. Children growing up in facilities is not consistent with ODP values.
It was in these early stages of the initiative that the work and recommendations from the Imagine Different Coalition were reviewed2. The Imagine Different Coalition is a group of parents, advocates, and professionals who are working towards supporting children with disabilities to have the opportunity to grow up in family homes. They are solution driven and have been an integral part of the initiative to support children with medical complexities within Pennsylvania. It was through the Imagine Different Coalition that we were introduced to a program in Texas which transitions children with medical complexities from congregate care settings into family homes. This program, known as EveryCHILD Inc., was used as a model as we began to explore ways to support children with complex medical needs in Pennsylvania3.
To learn more, we collaborated with other DHS offices to determine if we were supporting children with medical complexities and their families in a wholistic way. This cross-system collaboration created a unified approach to conceptualizing the needs of individuals and families while also exploring ways to meet those needs. In order to wholly support children, we need to not only support their medical and physical needs, but also provide them with the opportunity to grow up in a family with caregivers who love and support them, caregivers with whom they feel a special bond, and caregivers who can offer them comfort and nurture. We need to work together as a system to determine how we can improve efforts to provide families with the resources, training, supports, and services to feel confident and comfortable with supporting their children at home.
It was apparent that silos existed among different offices across the system who were independently supporting specific needs of children with medical complexities, including those residing in pediatric facilities. Within DHS alone there are two different offices that license pediatric facilities: ODP and Pennsylvania’s Office of Children, Youth, and Families (OCYF). Pennsylvania’s Office of Child Development and Early Learning (OCDEL) provides and oversees Early Intervention services for children in facilities while the OCYF has guardianship of several children within facility settings. Pennsylvania’s Office of Medical Assistance Programs (OMAP) funds the nursing and medical care provided to children during their stay in facilities. And finally, Pennsylvania’s Office of Mental Health and Substance Abuse Services (OMHSAS) oversees the mental health and behavioral health services for all children. In recognition of the different silos existing to serve this population of children, we realized that until we were able to come together and collaborate our efforts in support of the different aspects of the children’s lives, we were not doing our best to support the “whole” child.
It was around this time that former ODP Deputy Secretary, Nancy Thaler, began her role as the Special Assistant to the Secretary of the Department of Human Services. Within this role, Nancy focused on the children with medical complexities who were being served within Pennsylvania. She coordinated a DHS workgroup which included all the offices supporting children with medical complexities. The purpose of the workgroup was to discuss key challenges and diagnoses that have led to the placement of children in pediatric facilities. This workgroup explored the current system structure, discussed all services that are available to support children, and identified any gaps within the larger system. Soon after this workgroup was formed, Governor Tom Wolf issued an executive order that made a commitment to support vulnerable populations, which included children with medical complexities. This executive order strengthened our “why” and the importance of the work that we were embarking upon.
DHS staff acknowledged the importance of understanding the
needs of children with medical complexities and their families and sought
direct feedback from them regarding their vision around needs for system
change. Members of the DHS workgroup connected directly with individuals to
hear their personal stories and made a commitment to seek out the voices of
families. Representatives from ODP
traveled across the state to visit existing providers who support children with
medical complexities, including some pediatric facilities. We met with a wide
range of individuals at the facilities including social workers, medical
directors, nurses, and direct care staff. Representatives from the DHS
workgroup also took time to meet face to face with families and spoke directly to
children and their caregivers to hear and learn from their unique experiences.
There were four themes identified including a) a need for someone who was familiar with and understood all the different systems supporting children, b) a responsibility to support behavioral needs of children with medical complexities, c) a challenge to ensure that medical supports and behavioral supports were coordinating services by joining together to meet the complex needs of children, and finally d) a need to support families to overcome the barriers to going home.
Filling the gaps and overcoming barriers
The next phase of this initiative was to determine how to fill the gaps that were identified by the DHS workgroup. There was a risk of losing momentum and a need to ensure that the recently established collaborative relationships between DHS offices and others within the system were maintained to support one another as well as hold one another accountable to continue the work around this population. At the end of 2019, the DHS Transition Home Team was organized to provide an opportunity for state offices to discuss and identify barriers that children and families face around living together at home and strategize any necessary changes within the system to help overcome those barriers. The Transition Home Team consisted of representatives from the ODP, OMAP, OCYF, OCDEL, OMHSAS, Pennsylvania’s Office of Long-Term Living (OLTL), DHS Policy office, and the Family Facilitator. To establish continuity across the offices for the purpose of this team, lead contacts were identified within each of the participating DHS offices. Having clarity on who to contact within each office has been a great service to the collaboration and increases efficiency when overcoming obstacles.
We again acknowledged the need to involve different levels when seeking to overcome barriers within the system. This required ongoing investment and input from stakeholders and those at the community and provider level who are on the ground directly supporting children and families.
Using the EveryCHILD Inc. model from Texas, the PA Family Facilitator role was developed to help families and children with complex medical conditions move back into family life3. In 2020, ODP contracted with Philadelphia Coordinated Health Care (Pennsylvania’s Southeast Region’s Health Care Quality Unit) and hired Jennifer Harniman-Crangle, LSW as the Family Facilitator for Pennsylvania4. The purpose of this position is to partner with those at the community and individual level including medical providers, support teams, and other community networks to ensure that the child has a smooth return home. A contract was established with EveryCHILD Inc. to provide technical assistance and support to the Family Facilitator as this role was developed in Pennsylvania3.
The Department of Human Services offices have also collaborated with those at the county and community levels including Managed Care Organizations (MCO); Early Intervention (EI) Specialists; Children, Youth, and Families (CYF) case workers; pediatric facility providers; schools; mental-health providers; county Administrative Entities (AE); and waiver providers. There is not only an effort to raise awareness around this population and build capacity around supporting the whole child, but also to amend existing services and contracts to fit the needs of children with medical complexities. A DHS-wide bulletin was developed to ensure that all children across the different systems who are potentially eligible for ODP services are registered within the county system.
In recognition of the need to stay connected with stakeholders, ODP has presented information on the initiative and provided updates to Pennsylvania’s Information Sharing and Advisory Committee (ISAC) and has held regularly scheduled meetings with the Imagine Different Coalition.
The foundational work at the state and community level was established to ensure that we are wholly supporting children with medical complexities in homes within their community. This success relies on the ongoing cross systems collaboration for each individual. The following example of Maddy and Michael perfectly illustrate the importance and depth of cross system work.
Case Example
The Clients
Maddy (20 years old) and Michael (19 years old) are siblings who were the first discharge connected to the Family Facilitator project5. The siblings were in the custody of OCYF for over ten years. The parental rights were terminated and there were no other family members who were able to provide care. Maddy and Michael were placed in a pediatric nursing facility and remained together throughout that time, however, they were moved between three different facilities.
Maddy is an amazing young adult with a sassy sense of humor that she communicates through her eye rolls and smile. She loves to be pampered and always wants to look her best.
Michael is a strong young man with amazing potential. He wants to direct his day and enjoys being outdoors. He has preferences that he clearly communicates through vocalizations and his body language.
The Problem
Prior to the development of the family facilitator role, it was assumed that at age 21 each sibling would move into a group home in the community. Being that they are a year apart in age, it was very unlikely that they would end up together. Ensuring that these two siblings remained together was paramount and was important to the Community Umbrella Agencies (CUA) worker who had a substantial relationship with them and to Maddy and Michael. There were times when they were separated due to hospitalizations, and they were both observed looking for each other.
The Vision
In June of 2020, a referral was made to the Family Facilitator by the Managed Care Organization (MCO) Special Needs Case Manager. The conversation started with, “I don’t know if this is a case you can help with but…”. The case manager shared that in her quarterly contacts with the CYF worker she was aware that her client had a sibling, and that the CYF worker (who supported both Maddy and Michael) was very worried about finding a home for the two of them and felt very uncertain about their future.
In a follow up call with the CYF worker, we discussed the history and the problem. We focused on the vision which was to keep Maddy and Michael together and find them a permanent home, not a placement, of which they have had many. We utilized the Charting the LifeCourse Trajectory and Star of Support to create a map that would get this group of supporters on working towards the same outcome6. The CYF worker later shared that during that initial call she started to feel hopeful and excited about the siblings’ future.
Conversations with Maddy and Michael were challenging since this was during the height of the COVID-19 pandemic. Seeing them in person was challenging, so all communication happened remotely using FaceTime. The CYF caseworker talked to the siblings about the move and Maddy and Michael did their best to share their thoughts and feelings through their non-verbal communication.
Systems and advocates
Michael and Maddy’s team started out small but quickly expanded. A core group of four people representing four different systems (ODP, Managed Care Organization, OCYF and the facility) grew to twelve systems totaling eighteen people joining regular meetings: three state offices (ODP, OMAP, and OCYF), County Intermediate Unit, provider agency, medical community, pediatric facility, DHS nurse, County Court, County CYF, Supports Coordination, and County Administrative Entity. Everyone who came to the table were committed to creating a great life for Maddy and Michael, which also meant we had to agree on what that life would look like.
While planning for Maddy and Michael’s discharge, team members were able to ask questions about the vision for the siblings so that we all had a clear understanding of what we were creating. We asked people to come with an open mind and be willing to develop a knowledge base of services in systems outside of their own, and to weave together supports.
Prior to the development of this project the most likely outcome would have been for Maddy to move when she turned 21, and Michael to continue to live at the pediatric facility. When he turned 21, he would most likely move to a different group home, or maybe even a nursing home. By including all the systems supporting these siblings from the beginning of these efforts, we were able to create a solution in which they could stay together, forever; while reducing loss and trauma, increasing stability, predictability, and happiness. We needed each and every team member to make this a reality.
Through the collaboration of this team, guided by the Family Facilitator, and their willingness to come together, learn about other systems, and devote time and effort to the vision versus a placement, Michael and Maddy now live in the community together!
The Present
Three years have passed since some of those early conversations around reviewing how children with medical complexities are supported in PA. Within that time there has been great movement due to the cross-system efforts and relationships that have been established in an effort to consider ways that we can become even better in PA at supporting the needs of children with medical complexities. When considering the cross-systems work involved with this initiative and the ability to unite siloed offices and programs it is apparent that this has been nothing less than a tremendous accomplishment within PA.
References
1. Pennsylvania Department of Human Services, Office of Developmental Programs. Everyday Lives: Values in Action: 30th Anniversary Edition. 2021.
2. Imagine Different Coalition. PEAL Center and Pennsylvania Developmental Disabilities Council. 2016.
3. EveryCHILD Inc. Contracted with the Texas Health and Human Services Commission. https://everychildtexas.org/. Created July 2000.
4. Southeastern Pennsylvania Heath Care Quality Unit (HCQU): Philadelphia Coordinated Health Care (PCHC) a core program of The Philadelphia Mental Health Care Corporation (PMHCC). 1999.
5. Names and other identifying information have been changed.
6. Charting the LifeCourse framework. University Missouri -Kansas City Institute for Human Development website. https://www.lifecoursetools.com/lifecourse-library/lifecourse-framework/. Published 2010. Accessed August 19, 2021.
Biographies
Heidi Arva is a Clinical Consultant for the Office of Developmental Programs – Bureau of Supports for Autism and Special Populations. Prior to working at ODP, she spent over 14 years providing direct support to children and families. Since 2018, she has been the lead within ODP working on the department wide initiative to support children with medically complex needs.
Jennifer Harniman-Crangle, LSW joined Philadelphia Coordinated Health Care (PCHC), SE Region’s Healthcare Quality Unit, in January 2020 as Pennsylvania’s first Family Facilitator. Jennifer is a licensed social worker with over 20 years of experience supporting families in Pennsylvania across the lifespan.
Contact Information
Heidi Arva
Clinical Consultant, Office of Developmental Programs
717-395-9549
Jennifer Harniman-Crangle, LSW
Family Facilitator, Philadelphia Coordinated Health Care (PCHC)
267-951-3433
Cherpes, MD | 24-41
Volume 10 ► Issue 3 ► November 2021
The Collaborative Capacity Building Initiatives:
A Joint Project of the Office of Developmental Programs (ODP) and the Office of Mental Health and Substance Abuse Services (OMHSAS)
Gregory Cherpes, MD
Abstract
Individuals with intellectual disabilities and/or autism (ID/A) who also have a concurrent mental health condition are often referred to as having a dual diagnosis. Though estimations of the prevalence of dual diagnosis vary over a wide range, the prevalence of 35% is a commonly referenced value.1,2,3 The professional organization National Association for Dual Diagnosis (NADD) has published this estimation in their discussion of dual diagnosis.4 A report on National Core Indicator TM data using In-person Survey data that was collected in 2017-18 by 35 states and the District of Columbia showed approximately 48% of the 22,513 survey respondents, 10,729 identified having both an ID diagnosis and at least one of the following diagnoses: mood disorder, anxiety disorder, psychotic disorder, or “other mental health diagnosis.”5 The percentage of state respondents for whom a dual diagnosis was reported ranged from 34% to 64%.
Regardless of the
specific percentage of individuals affected, such cooccurrences are significant
and reflect significant challenges for individuals to receive comprehensive and
inclusive community-based resources. Despite the notion of dual diagnosis representing
on many levels an integrated construct from which to approach the support of an
individual with ID/A, the support systems themselves and individuals with
mental health conditions are often distinct and separate systems.
In the Commonwealth of Pennsylvania, the Department of Human Services’ Office of Developmental Programs (ODP) and Office of Mental Health and Substance Abuse Services (OMHSAS) have a long-standing partnership in recognizing the importance of collaboration. This article focuses on some of the ways that the Offices have been able to collaborate with the goal of building capacity throughout the commonwealth and among a variety of stakeholders. Specifically, the focus will be on activities that have been supported at least in part by the Money Follows the Person (MFP) program and have contributed to the Collaborative Capacity Building Initiatives.
Collaborative Capacity Building Initiatives
First authorized in 2005, the Money Follows the Person (MFP) demonstration supports state efforts for rebalancing their long-term services and supports system so that individuals have a choice of where they live and receive services.6
The goals of the MFP grant program include:
· Increase the use of home- and community-based services (HCBS) and reduce the use of institutionally based services
· Eliminate barriers that restrict the use of Medicaid funds to let people receive long-term care in the settings of their choice
· Strengthen the ability of Medicaid programs to provide HCBS to people who choose to transition out of institutions; and
· Put procedures in place to provide quality assurance and improvement of HCBS.
During the 2016-2020 funding cycle for Money Follows the Person, ODP and OMHSAS partnered to create the Collaborative Capacity Building Initiatives. This was a series of projects with the focus on individuals with complex needs due to the presence of ID/A as well as mental health needs. These efforts were foundational in establishing enhanced communication and interface among the support network necessary to increase capacity to serve individuals with complex needs in integrating settings. Staff from ODP and OMHSAS, including Pennsylvania’s State Operated Facilities, along with community providers of various backgrounds from a range of integrated settings and behavioral health managed care organizations all participated in training and educational activities, building toward a transdisciplinary framework for support.
By design, the components of the collaboration were selected to:
- Increase capacity of integrated community settings to support those most vulnerable who required institutional settings
- Increase capacity of institutional or less integrated settings, such as acute or longer-term treatment settings, to support transition back to integrated community settings
- Promote trauma informed approaches
- Promote best and promising practices to enhance resilience and recovery
- Offer caregiver training and education across the continuum of service sites
- Offer provider and direct service worker education, training, technical assistance, quality improvement activities, and enhanced recruitment abilities
Initiatives from the 2016-2020 MFP cycle included:
Annual Dual Diagnosis Conference
Beginning in 2017, ODP and OMHSAS collaborated to host an annual conference focused on topics pertinent to supporting individuals who are dually diagnosed. The conference has been held either independently or in conjunction with ODP’s Everyday Lives Conference.
Professional Conference Series
This series of single-day sessions brings experts from various fields to provide specialized opportunities for clinicians in practice and in training, such as psychiatric residents, certified registered nurse practitioners, registered nurses (RNs), licensed practical nurses (LPNs), social workers, behavior specialists and direct support professionals (DSPs). Through a variety of topics, the series provides enhanced exposure to and education about the needs of individuals with I/DA and mental health diagnoses. As with many of the initiatives, the forum also provides attendees with the opportunity for networking with other service professionals. Topics have included:
- Advanced Biographical Timeline
- Advanced Functional Behavioral Assessment (FBA): Tips, Tricks, and Tools to Develop Quality FBAs
- Percussion/Drumming and People with I/DA
- Supporting Healthy Aging Across the Lifespan
- Improving Outcomes for Persons with Intellectual Disabilities and Mental Health Issues by Recognizing Fetal Alcohol Spectrum Disorders and Modifying Approaches
- Supporting Individuals with Sensory Impairments
- Healthy Sexuality
Mental Health First Aid
Mental Health Frist Aid7 is a standardized, 8-hour, in-person training course that teaches people how to identify, understand, and respond to signs of mental illnesses and substance use disorders. This course has long been in use in Pennsylvania and has been well supported by OMHSAS prior to these initiatives. The Collaborative Capacity Building Initiatives strived to bring this training to the target audiences of individuals with I/DA, families, DSPs, supports coordinators (SCs), HCBS service providers, and State Operated Facilities with the goal of increasing awareness and capacity to recognize signs and symptoms of mental illness. No modifications were made to the standard curriculum and topics covered included anxiety, depression, psychosis, and addictions. The instructors who provided the course for this initiative did have experience supporting individuals with I/DA, however.
Dual Diagnosis Curriculum
Developed as a collaboration between ODP, OMHSAS and the commonwealth’s Health Care Quality Units (HCQUs), the Dual Diagnosis Curriculum consists of 20 lessons for DSPs, SCs, and other stakeholders. The lessons have been recorded as online modules and are available on the ODP website, www.MyODP.org.
Functional Behavior Assessment (FBA) Training
An interactive, self-paced, virtual FBA training was developed by Pennsylvania’s Bureau of Supports for Autism and Special Populations as a replacement for the previously established train-the-trainer model. The training content includes assessment and replacement of challenging behaviors, as well as development of a treatment or behavior support plan that can be used across settings and across the lifespan. Consisting of eight online modules, the course is responsive to the individual learner’s progress on tests and quizzes throughout the training. The training offers traditional and fast-track options, dependent on test/quiz scores. Becoming available in 2020, the virtual training allowed for continuity during the COVID-19 pandemic in a way that would not have been possible with the previous in-person training process. The FBA training is currently available on the ODP website, www.MyODP.org.
Capacity Building Institute
Named after the overarching collaborative initiatives, the Capacity Building Institute (CBI) is jointly guided by ODP and OMHSAS to provide broad, in-depth educational experience to a range of professional stakeholders who support individuals with I/DA and mental health conditions. The course occurs 2 days per month over a period of 9 months. Through didactic, experiential, and small breakout group discussions, CBI offers high level education with a focus on best and promising practices from multiple perspectives in supporting individuals with complex needs. Attendees represent a wide spectrum of professionals and include residential service providers, behavior specialists, practicing clinicians, managed care organizations, state hospital staff, state operated intermediate care facility staff, residential treatment centers, HCQUs, Autism Services, Education, Resources, and Training Collaborative (ASERT), as well as staff of ODP and OMHSAS.
The goals of CBI include:
- Expand the knowledge of all elements of the partnership serving people with multiple diagnoses in the widening array of therapeutic supports that are effective for the general population
- Provide crosswalk information to assure that promising practices are available for all individuals regardless of the degree of intellectual disability
- Promote a more seamless response system between the OMHSAS and the ODP systems
- To facilitate the development of county, region, and state-wide networks that can work together to address issues regarding individuals who are challenging to support
- Develop a state-wide resource list of local go-to people to help find solutions to individual issues
- Identify key issues and problem-solve on a systemic level
- Explore and quantify the issues creating barriers for the practitioner and caregivers in their ability to support people with complex needs
- Create and share recommendations for policy and best practices with the Deputy Secretaries of ODP and OMHSAS
As noted above, a key component of CBI beyond the educational experience is the opportunity to develop a statewide cohort of individuals and systems becoming better equipped to effect change on micro and macro levels. The first cohort of attendees began in 2016. CBI is currently supporting its fifth cohort with plans to begin recruitment for the sixth cohort in early 2022. The core curriculum has developed over time and has been informed by the attendees. Numerous attendees have contributed to the education of the participants as subject matter experts. Curriculum topics have included:
- One Page Descriptions
- Trauma
- Learning from a person’s biography
- Psychiatric perspectives/working with a team
- Behavioral assessment
- Caregiver fatigue
- Self-Care
- The role of the social therapist
- Therapeutic modalities
- Autism
- Pharmacotherapy
- Psychotherapies
- Eye movement desensitization and reprocessing (EMDR)
- Biofeedback
- Neurofeedback
- Creative and Expressive Therapies
- Genetics
- Self-advocacy
- Family advocacy
- Physical manifestations of trauma
- Life Course
- Sexuality
- Grief and loss
- Resources of ODP and OMHSAS
In the small group breakout discussions, which run throughout the duration of the institute, participants focus on and discuss complex and challenging situations, often applying information gained from the didactic work. In the final session of each cohort, attendees give presentations to the deputy secretaries of OMHSAS and ODP, discussing key issues, barriers, and solutions to the myriad challenges discussed over the course of the 9-month institute.
Continuing the Work of Collaborative Capacity Building
Looking beyond 2020 and intending to continue the work of building capacity, ODP and OMHSAS have committed to continuing close collaboration and coordination of activities through new initiatives, and in doing so, anticipate reaching an even broader set of stakeholders. Certainly, much has changed since the initiation of the MFP funded Collaborative Capacity Building Initiatives. Though both Offices have long appreciated the impact of trauma in the lives of our stakeholders and the need for trauma-informed practices, events occurring nationally and globally have served to heighten this appreciation. Pennsylvania is uniquely poised to address the challenges posed to long-term care system transformation and is building on the collaborative experiences of the 2016-2020 MFP cycle amidst the development of the Governor’s Trauma Informed Pennsylvania (PA)A Plan.8
In order to achieve these goals, components of the collaboration will require a multi-pronged approach to engage and have impact on the necessary participants. New initiatives in this comprehensive approach will include:
TRAIN: Trauma Recovery for Autistic, Intellectually
disabled, and
Neurodiverse individuals
Unfortunately, we know that autistic, intellectually disabled and neurodiverse individuals are at high risk for trauma exposure and victimization. They encounter many barriers if and when treatment is sought. One of the most challenging barriers is lack of providers who feel prepared to support them.
This training curriculum, which is intended for licensed therapists of various disciplines, aims to address this deficit. A multi-disciplinary team from central region ASERT at the Penn State College of Medicine has developed this curriculum through consultation and input from experts within the c and nationally. The first cohort of licensed therapies participating in TRAIN has been enrolled. The curriculum will be presented in 2 phases:
- The initial phase of the curriculum occurs over 12 weeks and incorporates webinar and self-guided learning experiences. During this phase, therapists will learn evidence-based and emerging best practices to treat neurodiverse survivors in trauma recovery. Trainees will have the opportunity to receive feedback from the trainers on their understanding and application of the material.
- The second phase of this curriculum is through participation in bimonthly supervision calls with the lead trainers who will provide mentoring as therapists begin using the course content in their work. There will be an opportunity for ongoing supervision and mentoring after course completion for therapists who wish to continue growing their skills and collaborate with their colleagues.
Pennsylvania START Model – A Pilot
Currently for individuals with I/DA with a cooccurring mental illness who experience crisis, there are gaps in the community mental health system. These individuals often require a high level of specialized skill in assessment and development of treatment approaches. Often, these individuals are at high risk for extended inpatient hospitalizations, incarcerations, and admissions to state facilities. Current models in place through the Dual Diagnosis Treatment Teams and the Assertive Community Treatment models have shown some positive outcomes. However, there continues to be a need to build on these models and PA will pilot the use of the Systemic, Therapeutic, Assessment, Resources and Treatment (START) model in addition to these promising practices. START is a research-based model of services and supports for individuals with an intellectual/developmental disability (IDD) ages six and older who also have a mental health (MH) diagnosis or behavioral health needs. The START program model was implemented in 1988 by Dr. Joan Beasley and her team to provide community-based crisis intervention for individuals with IDD and behavioral health needs. START is a person-centered, solutions-focused approach that employs positive psychology and other evidence-based practices. Cited as a model program in the 2002 U.S. Surgeon General’s Report on mental health disparities for persons with intellectual/developmental disabilities, START is a comprehensive model of service supports that optimizes independence, treatment, and community living. START is an evidence-informed model that utilizes a national database. START is a national model, adopted in several states. By design, the program builds upon existing resources and services. The PA START pilot project will be initiated under a contract with the University of New Hampshire (UNH) Center for START Service and PA. The UNH team will provide training and technical assistance to the PA START team. Allegheny County is serving as the lead for this 3-year pilot. During the pilot, all counties in PA will benefit from the expertise and information available through START UNH, including the START newsletter. Ultimately, if the pilot is successful, the hope is to expand START services to the entire commonwealth, incorporating what is learned from the pilot and adjusting along the way.
Project Reassure (Resilience and Stress Support Rallies Everyone)
For Pennsylvanians with I/DA and their caregivers, the unprecedented levels of stress due to the pandemic may be particularly high for a population that is at high risk for victimization. Trauma related to the pandemic has been both direct and indirect, including disruption of routine, changes in services and changes in interactions with natural and paid caregivers. Some may have experienced an exacerbation in preexisting or unresolved trauma issues. Fostering resilience for both providers and participants is critical in enhancing adaptive stress responses. At present, there are limited provider supports to address building resiliency. Masters level therapists/supervisors and DSPs have potential for high contact with program participants but may not be prepared to address or even recognize the trauma/stress needs for the individuals that they support or for themselves. Therefore, ODP and OMHSAS have planned in conjunction with a multi-disciplinary team from central region ASERT at the Penn State College of Medicine a two-phase approach to address these critical issues: developing micro-learning resources and creating trauma focused learning collaboratives.
- Phase 1-Micro Learning Resources-The first phase will be the creation of a collection of highly engaging, brief digital “micro-learning” resources that live on a curated mini site within the existing website, AIDinPA (www.aidinpa.org). These resources will expand existing content about COVID-19 response and other trauma related issues. New materials will be developed to supplement information gaps and respond to new needs. Material will reflect the learning styles and modes of engagement of those who are familiar with web-based resources. Digital best practices will include brief and focused trainings covering 1-2 key points, each allowing learners to access information and learn at their own pace and strategies that emphasize high engagement with ready real-life application of material and opportunities for individual distinction.
Feedback about the site’s functionality will be obtained through collaboration with stakeholders.
- Phase 2-ECHO -The Extension for Community Healthcare Outcomes (ECHO) project will focus on the expansion and targeted dissemination of the micro-learning resources but will also create a structured framework of trauma focused learning collaboratives and technical assistance opportunities. This effort will encourage building and bolstering system wide capacity to serve those in need of trauma informed care. ECHO will be directed at master’s level supervisors, group home managers, behavior specialists and program coordinators to help sensitize the system to resilience building. ECHO addresses population health needs in a scalable way– moving knowledge instead of participants via tele-mentoring and collaborative care. The ECHO model™ has hub-and spoke knowledge-sharing networks, led by expert specialist teams (hub) and mentoring multiple community providers (spokes).
The ECHO model is not “telemedicine” where specialists assume the care of the client; it is a guided model aimed at practice improvement, in which local providers retain responsibility for supporting their clients, operating with increasing independence as skills, confidence, and self-efficacy grow. This virtual learning community offers expert mentoring and feedback from specialists.
Providers
from multiple locations connect at scheduled times with a team of specialists
through videoconferencing. The providers present de-identified client cases to
the hub team who then mentor the providers as they learn to support
participants with complex issues. These case-based discussions are supplemented
with brief presentations to improve content knowledge and share evidence-based
practices. Each ECHO develops its own curriculum to achieve its intended health
parity outcome; a hub and its associated spokes meeting around the prescribed
curriculum is termed a “clinic”. When this project is operational, likely in
2022, the clinics will focus on increasing awareness of trauma resultant from
and activated by COVID-19 in those with I/DA.
The project will have statewide impact and enhance home and community-based programming. It is a sustainable and easily accessible resource used by DSPs in varied settings supporting individuals with diverse needs. Each spoke participant is intended to be a supervisor of other professionals and expected to transfer information to help their team members use the repository for their shared cases.
Conclusion
Despite the many challenges and potential barriers that have been ushered in or exacerbated during the COVID-19 pandemic, many opportunities exist to address and diminish the barriers. Building on a foundational partnership, ODP and OMHSAS will continue to collaborate and engage in ongoing efforts to build capacity across the commonwealth. Increasing capacity through educational experiences, novel program introduction and enhanced professional networks will help to further build the necessary supports for individuals with complex needs to enjoy an everyday life in the community.
References
1.
Szymanski L, King BH. Practice parameters for the assessment and treatment of children, adolescents, and adults with mental retardation and comorbid mental disorders. American Academy of Child and Adolescent Psychiatry Working Group on Quality Issues. J Am Acad Child Adolesc Psychiatry. 1999; 38(Suppl. 12):5–31s.
2. Cooper SA., Smiley E, Finlayson J, Jackson A, et al. The prevalence, incidence, and factors predictive of mental ill-health in adults with profound intellectual disabilities. Journal of Applied Research in Intellectual Disabilities. 2007;20: 493–501.
3. Morgan VA, Leonard H, Bourke J, Jablensky A. Intellectual disability co-occurring with schizophrenia and other psychiatric illness: population-based study. Br. J. Psychiatry. 2008;193: 364–372.
4. IDD/MI Diagnosis. National Association for the Dually Diagnosed website. IDD/MI Diagnosis - The NADD. Accessed November 16, 2021.
5. What Do NCI Data Reveal About People Who Are Dual Diagnosed with ID and Mental Illness? National Core Indicators (NCI) website. NCI Data Brief: Guardianship nationalcoreindicators.org). Published October 2019. Accessed November 16, 2021.
6. Money Follows the Person. Medicaid website. Money Follows the Person | Medicaid. Accessed November 16, 2021.
7.
Mental
Health First Aid website. Mental Health
First Aid. Accessed November 16, 2021.
8. 2020 Trauma Informed PA Plan. Scribd website. 2020 Trauma Informed PA Plan | PDF (scribd.com). Accessed November 16, 2021.
Biography
Gregory Cherpes, M.D. is the Medical Director for the Office of Developmental Programs. He is board certified in general psychiatry as well as child and adolescent psychiatry. Dr. Cherpes' clinical, research, and educational efforts have been devoted to addressing the healthcare needs of people with intellectual and developmental disabilities across the lifespan. Prior to joining ODP in 2015, he served as the Director of Behavioral Health and the Director of The Center for Prader-Willi Syndrome of The Children's Institute of Pittsburgh; the medical director for Child, Adolescent and Developmental Disability Services at Allegheny East Mental Health/Mental Retardation (MH/MR) and is the former medical director of two of the state's Health Care Quality Units.
Contact Information
Gregory Cherpes, MD
Office of Developmental
Programs
gcherpes@pa.gov
Durgin | 42-57
Volume 10 ► Issue 3 ► November 2021
Pennsylvania System of Care: Improving Services and Supports for
Youth and Families with Behavioral Health Challenge
Mark B. Durgin
Introduction
The PA Care Partnership philosophy of System of Care (SOC) builds and promotes equality and trust by including youth, caregivers, providers, and systems that serve children and young adults based on the individual community's strengths and culture. A SOC is achieved by strengthening the collaboration of the commonwealth and county efforts in a statewide approach to build behavioral health supports and services for children, youth, young adults, and their families. A seamless system of care builds effective community-based services and supports that meet youth and families' needs to assist with behavioral health challenges.
Pennsylvania's Department of Human Services, Office of Mental Health and Substance Abuse Services (OMHSAS) has been the recipient of four (4) Substance Abuse and Mental Health Services Administration (SAMHSA) grants that have allowed the commonwealth to build an infrastructure to implement a statewide approach to SOC to serve children, youth, young adults, and their families who have, or need effective community-based services and supports to assist with behavioral health challenges, since 2009.
Through a SOC philosophy, the PA Care Partnership builds and promotes equality and trust by including youth, caregivers, providers, and systems that serve children and young adults based on the individual community's strengths and culture. Adopting this philosophy doesn't mean that communities throw out the programs, services, and supports that they already have in place. A SOC is not a thing, a service, or a program—it is an organizational construct anchored in partnerships—between families, youth, government agencies, private providers, and communities. This makes the System of Care flexible and adaptable enough to work almost anywhere.
A system of care is defined as a spectrum of effective, community-based services and supports for children and youth with or at risk for mental health or other challenges and their families that:
- Build meaningful partnerships with families and youth
- Organize into coordinated networks
- Address Cultural and linguistic needs
In order to help families function better at home, in the community, and throughout life.1
The mission of the PA Care Partnership is to strengthen the collaboration of the commonwealth and local efforts in weaving behavioral and mental health supports and services into a seamless system of care for children, youth, and their families. This is achieved through the development of local and state leadership teams focusing on the SOC values, providing training inviting multiple systems (Child Welfare, Juvenile Justice, Mental Health, Education, Early Childhood, etc.) to attend training, and through including youth and family with lived experience in decision making.
The vision for the PA Care Partnership is for every youth and family in the commonwealth to be able to access and navigate a unified network of effective services and supports, which are family and youth-driven, community-based, culturally competent, and meet their individual needs. Pennsylvania's SOC model has evolved into a sound philosophy and flexible approach to promote equity and trust among youth, caregivers, child-serving systems, and provider partners based on the individual community's strengths and culture. The goal of a System of Care is to modify the way that youth, families, government, and counties interact with each other so that:
- Youth/young adults and families with lived experience are central to the design, implementation, and operation of services and support working in equal partnership
- Youth and family organizations support individual youth/young adults and families and participate fully in policy and funding decisions
- All child-serving system partners collaborate, share resources, and coordinate with each other and with youth and families
- Natural supports are equally as valuable as formal supports (i.e., paid services)
- Communities engage and transform to become welcoming and supportive of all youth, young adults, and families
The SOC concept is not new to Pennsylvania. There are currently five (5) System of Care grants operating in Pennsylvania, funded through SAMHSA. The current grants are the PA Care Partnership, the Philadelphia System of Care, Allegheny County System of Care, Behavioral Health Alliance of Rural PA, and the Luzerne-Wyoming System of Care. Although these grants have different initiatives from the PA Care Partnership, the core function and values remain similar. These grants work in concert to address the needs of Pennsylvania’s youth and families to build a more robust, equitable, and service-driven SOC.
The SOC not only builds
upon but strengthens our state's strong history with our Child and Adolescent
Service System Program (CASSP). Both are comprehensive approaches that support
children and adolescents with complex behavioral health challenges and their
families. They seek to ensure that services and/or treatment are planned
collaboratively with the family and all agencies and/or systems involved in the
child's or adolescent's life.
Essential to an effective SOC is having system partners working together. System partners help families function better at home, in school, community, and throughout life.2 Systems vary throughout the commonwealth and may include a combination of public agencies, private organizations, and the faith-based community. Your county may have more or fewer systems, but typical system partners might include:
- Mental health services
- social services
- educational services
- health services
- substance abuse services
- vocational services
- recreational services
- juvenile justice services
- early childhood services
- domestic violence services
- autism and intellectual disability services
The challenge—and opportunity—comes in de-siloing systems that don't typically work together, such as mental health and juvenile justice (court system). When youth and family-serving systems are integrated effectively, mechanisms are established to manage and coordinate care in a person-centered approach that meets the needs of youth and family's social, emotional, and physical health. In addition, this integration taps into the natural and community support available to youth and families.
A SOC, however, expands the role of youth and families as decision-makers at the individual, county, and state levels to ensure they receive the most beneficial, culturally, and linguistically competent services and supports. This is achieved by having youth and family as part of county and state leadership teams, employed as peers, as part of behavioral health treatment and planning processes. As a result, systems work more effectively, allowing communities to respond and adapt to challenges nimbly to improve outcomes for youth and families. Information related to outcomes is detailed below.
The PA Care Partnership has worked with the following counties: Blair, Carbon, Chester, Crawford, Delaware, Erie, Fayette, Greene, Lackawanna, Lawrence, Lehigh, Luzerne, Monroe, Montgomery, Northumberland, Philadelphia, Pike, Venango, and York.
Counties working with the PA Care Partnership Grant:
- Collaboration between county system partners agencies, youth, family, and providers
- Education of partners (youth, family, child welfare, juvenile justice, mental health, education, early childhood, intellectual disabilities, etc.)
- Support and enhance services and supports for youth, young adults, and families
- Partnership with natural and community supports
- Creation of policy and funding decisions, including youth and family's full support and engagement with lived experience
- Education and support families and youth to be equal at meetings and training
- Collaboration of partners who share resources and coordinate with one another and with youth and families
- Community engagement and transformation to become welcoming and supportive of all youth, young adults, and families
- Enhancement or increase services and support for youth in the target population with guidance and support to implement required youth and family services and support the planning process
Core Values
An effective SOC relies on the adoption of a core set of values that easily adapts to the realities of any community, including the kinds of challenges that come with stretched resources and decreased budgets. In adopting these core values, systems work more efficiently and save community resources by preventing or reducing entry into higher levels of care or out-of-home placement. Moreover, youth and families have an equitable role in making decisions about their own care leading to better outcomes.
The PA Care Partnership has developed eleven (11) Core Values, which are the foundation of a system of care. Additionally, the values have been vetted and approved by the Technical Assistance Network, part of the University of Maryland School of Social Work, the national technical assistance provider for SOC grants. These values transition the SOC toward a public health framework by focusing on treatment for individual children with serious behavioral health conditions and addressing promotion, prevention, early intervention, and education to improve total health—physical, oral, developmental, and behavioral health.
The System of Care values guides and direct how to implement the philosophy throughout the Commonwealth of Pennsylvania.
- Youth-driven is having youth included in decisions that affect their care and well-being. Youth are supported in various ways by sharing their experiences and opinions to be leaders at the county and state levels.
- Family-driven means families have a primary decision-making role in caring for their children, and opportunities are provided for leadership positions at the county and state levels.
- Home- and Community-based builds on the community's strengths where the family lives, providing community-based high-quality services accessible to families.
- Strength-based & Individualized Practices & Processes identify and build on the youth and young adult's individual strengths and concerns. Family plans are created by teams of people to which they are connected.
- Trauma-informed means that every part of an organization or program understands the effects of trauma on the individuals they serve and promotes cultural and organizational change in responding to those they serve.
- Culturally and Linguistically Competent is the integration and transformation of knowledge, behaviors, and attitudes from and about individuals or groups to enable all team members to work effectively in cross-cultural situations.
- Connected to Natural Helping Networks are personal associations and relationships, independent from formal services, developed in the community that enhance the quality and security of a family or person's life.
- Data-driven, Quality, and Outcomes-Oriented Decisions are made using concrete information about what is happening, rather than personal stories or gut feelings to identify high-risk children and youth.
- County Leadership Team and Governance Boards are comprised of representatives from child-serving and transitional age systems, family members, and youth partners.
- Multi-System Integration ensures that services and supports are integrated at the system level, linking child and transition-aged serving agencies and programs across administrative, funding boundaries, and mechanisms.
- Youth and Family Services and Supports Planning Process facilitates integrated services and supports planning among youth, families, and key child-serving systems.
The Pa Care Partnership provides or sponsors a variety of training to the counties currently involved with the grant as well as to systems, providers, community agencies, youth, and families across the commonwealth. These trainings focus on the values of SOC to address multisystem integration, trauma-informed, cultural and linguistic competence, and being youth and family driven.
Trainings and Technical Assistance including:
- Trauma Workshops Through Lakeside Global Inc. – 2–4-hour workshops focusing on becoming trauma-aware/trauma-informed
- Coach Approach to Adaptive Leadership – Developed for health and human services, this training focuses on changing conversations, empowering others, and creating a culture of collaboration and support.
- Family Roadmap Training – Trains family members using guides and curricula to break up big, overwhelming problems into tasks they can handle.
- Youth and Young Adult Roadmap Training- trains youth, youth adults, and providers to help people break up big, overwhelming problems into tasks they can handle.
- Wellness Recovery Action Planning (WRAP) is a simple and powerful process for creating and maintaining wellness, developing a daily wellness plan, identifying setbacks, and gaining support.3
- System of Care: A Comprehensive Toolkit for County Implementation - A toolkit created by the PA Care Partnership to implement a System of Care with or without funding.
- System of Care Orientation – Helping counties, systems, partners, youth, and families implement a System of Care.
- System of Care Values
- Youth Engagement
- Family Engagement
Evaluation is a significant component for the grant implementation to report outcomes to SAMHSA and help counties and the commonwealth fully understand the impact of the supports and services. There is discretion on the types of services and supports which can be implemented. However, the services selected must have multiple encounters over time and be youth and family driven.
For the PA Care Partnership grant, counties have used the following:
- High fidelity wraparound enhanced services for transition-age youth
- Enhanced supportive living programming
- Juvenile treatment courts
- Intensive behavioral health services (IBHS)4
o IBHS support children, youth, and young adults with mental, emotional, and behavioral health needs.
o IBHS offers a wide array of services that meet the needs of these individuals in their homes, schools, and communities
- Family based5
o The Family based team is composed of:
§ A Master’s level mental health professional who functions as the primary therapist
§ A Bachelor’s level mental health worker who provides support and case management services
§ Through weekly individual and family therapy sessions, the team works with the youth and their family to identify barriers to communication, conflict resolution, bonding and areas of family life that have an impact on and are impacted by the child’s mental health issues
- Family peer support6
o This is a 5-day comprehensive training using the Family-Run Executive Director Leadership Association (FREDLA) Parent Peer Support Provider Practice Model.
o This Practice Model provides a framework for the essential functions of a Family Peer Support Specialist, offering core competency training and practicing of skills across the 6 phases of family peer support: Connect, Discover, Support, Empower, Prepare and Take Care.
- Youth peer supports7
o Youth and Young Adult Peer Support Services for young people are provided by Certified Peer Specialists (CPS) who have lived experience with mental health and related challenges.
o CPS are individuals trained to share their own stories of recovery and resiliency.
o They engage and inspire Transition Age Youth (TAY), ages 14-26, to plan for what is important to them in their everyday life.
- Peer-driven case management8
o Behavioral Health Case Management with either Youth or Family Peer Support imbedded in the program.
Through our evaluation data, we have enrolled 293 youth in the longitudinal evaluation. 94% of youth enrolled have two or more services involved, and 92% have mental health services involved at intake.
Data collected as part of the grant provided the following information:
- 13% of youth have experienced a traumatic event, series of events, or set of circumstances.
- 25% of youth had attempted suicide at intake.
- As a result of supports and services, the following positive outcomes were noted.
o 11% increase in overall health (Youth were asked to rate their overall health)
o 18% increase in daily functioning (Youth were asked how well they were functioning in daily life in the past 30 days, regarding the following categories: Handling Daily Life, Getting Along with Family, Getting Along with Friends, Doing Well in School/Work, Ability to Cope, Satisfied with Family Life)
o 5% decrease in psychological distress (Youth were asked how they were feeling in the past 30 days, regarding the following categories: Nervous, Hopeless, Restless or Fidgety, Depression, Effort, Worthless)
o Noted decreases in illegal substance use (-3%), tobacco use (-3%), and alcohol use (-1%)
o 5% increase in youth remaining in the community
o 2% increase in youth/family perception of care, with
91% reporting positive perception. (Youth were asked what they thought about
the services they received in the past 30 days, the people who provided it, and
the results)
In closing, Pennsylvania has had a long history of implementing SOC philosophies across the commonwealth. While counties and the commonwealth may vary in implementing a SOC, foundationally, they all have the same core values of being youth and family-driven, culturally and linguistic competent, and trauma-informed. In Pennsylvania, we must support the role of youth and families as decision-makers at the individual, county, and state levels to ensure they receive the most beneficial and culturally and linguistically competent services and supports. Through a SOC philosophy, systems, providers, community partners, youth, and families build and promote equality and trust. Children and young adults receive the services and support based on the individual community's strengths and culture.
Other Resources
Behavioral Health Alliance of Rural PA,
Luzerne-Wyoming System of Care
Trauma Workshops Through Lakeside Global Inc.
Coach Approach to Adaptive Leadership
System of Care: A Comprehensive Toolkit for County Implementation
High Fidelity Wraparound
References
1. System of Care Definition and Philosophy. National Technical Assistance Center for Children’s Mental Health website. https://gucchd.georgetown.edu/products/Toolkit_SOC_Resource1.pdf. Accessed November20, 2021
2. System of Care: A Comprehensive Toolkit for County Implementation: Enhancing Your Strengths to Build a System of Care. Pennsylvania Care Partnership website. https://www.pacarepartnership.org/uploads/PA_Care_Partnership_Toolkit_-_ELECTRONIC_VERSION_FINAL.pdf. Published August 2020. Accessed November 20, 2021
3. What is WRAP? Wellness Recovery Action Plan website. https://www.wellnessrecoveryactionplan.com/what-is-wrap/. Accessed November 20, 2021
4. Intensive Behavioral Health Services. Pennsylvania Department of Human Services website. https://www.dhs.pa.gov/HealthChoices/HC-Providers/Pages/BHProvider-IBHS.aspx. Accessed November 20, 2021.
5. Family-based Services. PA-Mentor website. Family-Based Services | Pennsylvania (pa-mentor.com). Accessed November 20, 2021.
6. Free Family Peer Support Specialist Training. Mental Health Partnerships website. Free Family Peer Support Specialist Training | Mental Health Partnerships (MHP). Accessed November 20, 2021.
7. Youth/Transition Age/Young Adults. Montgomery County, PA website. Youth/Transition Age/Young Adults | Montgomery County, PA - Official Website (montcopa.org). Accessed November 20, 2021.
8. Family, Parent, and Caregiver Peer Support in
Behavioral Health. SAMHSA website. Value of Peers
Infographics: Parent Support (samhsa.gov). Accessed November 20, 2021.
Biography:
Mark B. Durgin joined OMHSAS as a contractor in 2016 as the Director of Pennsylvania Care Partnership. Mark holds a B.S. in Criminal Justice from York College of Pennsylvania, focusing on parole and probation. In addition, Mark has over 20 years of professional experience in Pennsylvania's child-serving systems, working with youth and families at a county and state level.
Contact Information
Mark Durgin
Thaler | 58-74
Volume 10 ► Issue 3 ► November 2021
Serving Children and
Youth with Complex Behavioral Support Needs
“No provider will
serve him.”
Nancy Thaler
Abstract
When we hear the words, “no provider will serve him,” we know that we have a crisis; our service system is failing a person whose needs are very great. From my experience over five decades as a direct support worker, a houseparent, a provider agency administrator, and a state director, I can say that this is not new. We have struggled, since the earliest years of providing community services in the 1970s, to meet the needs of people whose behavior is problematic and can be dangerous. This article is based on information about 50 children and young adults who were in crisis and referred to the Pennsylvania Department of Humans Services in 2021. The interpretation of their challenges and needs and the description of the strategies that may address their needs is based on a synthesis of my experience in the field of developmental disabilities and developments in the field of trauma and behavioral health over several decades.
Introduction
“People with complex behaviors” is the language we use today to describe “people who are difficult to serve,” or “people with challenging behavior,” or “people who are dually diagnosed.” Regardless of the label, the challenge is the same. These individuals present behavior that is dangerous to themselves or others around them, behavior they cannot control, behavior that can be strange and frightening.
Over the decades, we have acquired new knowledge and additional resources. We know more about diagnoses such as Autism Spectrum Disorder (ASD) and bipolar disorder; we have new medications that are more targeted to a diagnosis than Thorazine and Haldol were. We know about trauma and the profound impact it has on a person’s ability to function; and we have new therapies.
We are doing better. There are many children and adults who have challenged and pushed us to our most creative limits. There are many providers who have expanded their knowledge base, have individualized services, and have learned to serve people with creativity and commitment.
But we need to do more. As a system we need to reach everyone.
Who are the children and youths with complex behaviors? What do we know about them? What makes their behavioral support needs complex?
Since the Department of Human Services’ publication of the Bulletin on Complex Case Planning for Children and Youth Under Age 21, issued August 2021, more than 50 individuals, from many counties across the commonwealth, have been referred to the Department of Human Services (DHS) with a request for assistance. The department receives a referral form and sometimes additional information such as social histories and evaluations. An analysis of the information about the first 50+ children and young adults tells us something about who they are and what their needs are. This group of young people is not a random sample; they are simply the first referrals sent to the department after the Bulletin’s implementation. But because there are similarities in their histories and needs, we can glean information to inform our efforts to improve services to children and youths with similar needs. The most significant information we can glean from a review of available records follows:
- Behavior - or more accurately multiple behaviors – this is the issue that is always identified as the reason a provider will not be willing to serve the child or youth. The most common descriptions of problematic behavior include:
o Hyperactivity
o Failure to Bond
o Aggression/hurting others
o Screaming
o Sleep Disturbance
o Property Destruction
o Fire Setting
o Refusal to Cooperate
o Elopement
o Theft
o Cannabis Use
o Enuresis
o Feces Smearing
o PICA
o Suicide Ideation
o Self-harm (self-hitting, head banging, self-mutilation, running into traffic, attempted suicide)
o Sexual acting out (public masturbation, promiscuity, predatory behavior)
- A majority (77%) are teenagers and young adults ages 14 to 19
- More than half (65%) are boys
- A majority (76%) have had at least five out-of-home placements, some as high as twenty
- Most are served by multiple systems of care. All are eligible for services from more than one system such as the Office of Children and Youth Services and Families, The Office of Mental Health and Substance Abuse, the Office of Developmental Programs and in a few cases, the justice system. Many receive services from local programs such as youth shelters.
- A significant majority (84%) of these youths have at least one mental health diagnosis, combined with more than one developmental disability. The diagnoses most often recorded are:
o Cognitive
§ Autism
§ Attention Deficit Hyperactivity Disorder
§ Brain Injury
§ Intellectual Disability
§ Fetal Alcohol Syndrome
§ Lead Poisoning
§ Syndromes including Prader-Willi and Von Willebrand Disease
§ Communication Deficits
o Health Conditions
§ Diabetes Type I and II
§ Epilepsy
§ Dysmenorrhea
§ G-tube
o Mental Health
§ Post-traumatic Stress
§ Developmental Trauma
§ Intermittent Explosive Disorder
§ Conduct Disorder
§ Dysregulation Disorder
§ Reaction Attachment Disorder
§ Anxiety
§ Depression
§ Bi-Polar Disorder
§ Obsessive Compulsive Disorder
§ Oppositional Defiance Disorder
§ Impulse Control Condition
§ Psychosis
§ Schizophrenia
§ Gender Dysphoria
- A percentage (38%) are from adoptive or foster families.
- More than half (68%) have a history of complex trauma. defined as trauma that occurs early in life and is persistent. This trauma is most often physical and/or sexual abuse.
- A small number have significant physical health problems or additional issues that require special attention. These include sexual identity exploration, Type II diabetes, problematic sexual behavior, involvement in the criminal justice system
- None of the older youths have a home or family to go to. Often, they do not meet the criteria for admission to a hospital or Residential Treatment Facility
- Unfortunately, race is not specified is the referral documents
When we are successful in meeting the needs of these individuals, what has worked?
Formal and informal interviews with DHS regional staff, county staff, and case managers have provided some insights. Counties, managed care organizations, and providers in many areas of the state are working together and “thinking outside the box.” Success is more likely when cross-systems teams work together to understand the needs of these children and youths and develop solutions.
- Using a System of Care approach and the principles of the Children and Adolescent Service System Program (CASSP).
- When local systems collaborate, bring their knowledge and resources together, and function as a team, it is far more likely that a solution will be found.
- Creating a positive environment that works for the individual. That environment typically involves:
o A setting for just a few or for a single individual
o A setting that is trauma-informed to assure there is no inadvertent re-traumatizing. This, of course, requires knowing the youth’s trauma history
o Enhanced staffing at a 1:1 ratio and sometimes 2:1
o Routines and activities to match the person’s emotional state
o Activities that build on the individual’s strengths and preferences, so he/she experiences success and develops self-confidence and self-esteem
o Treatment - including for trauma – that is aligned with the individual’s diagnoses
- Adjusting rates
o Negotiated or enhanced rates are often necessary to support a more individualized living arrangement, staffing ratios, and services
- Focusing on building trust and relationships
o A strengthening of support ties with friends and relatives
o Consistent, trained staff who are committed to the youth
Digging Deeper - Trauma in Children and Youths with Multiple Disabilities
Trauma is a major factor in the lives of many of these children and youths – and maybe more than we know - who have been referred to the department. Their trauma generally began in early childhood and has persisted. It has often gone unrecognized as the cause of their problematic behavior. Despite descriptions of extensive trauma in their records, that trauma has – incredibly - often not been identified as a diagnosis at all, nor has it been factored into their treatment plan.
Trauma that occurs in childhood is known as “developmental trauma” or “complex trauma” or “neurodevelopmental trauma.” Developmental trauma differs considerably from post-traumatic stress disorder (PTSD). An adult who experiences trauma and then PTSD has, presumably, a “normal” childhood to fall back on, so to speak - a history of stability. But when the trauma happens during a child’s development, it severely undermines “the capacity of the child to form close and secure adult and peer relationships; experience, manage, and express a full range of emotions; and explore the environment and learn…”1 We often see the diagnosis “dysregulation” somewhere in the person’s chart. This refers to an inability to manage thoughts and emotions and therefore to difficulty in controlling impulses and behaviors: the early trauma has made learning to “manage” or “control” simply impossible.
In other words, how a child or teenager or young adult behaves, learns, and relates to people is rooted in their early childhood experiences. A child raised in the security of a loving environment will develop healthy relationships, will trust adults, and will learn from their environment. But a child who experiences serious neglect and abuse – trauma - will develop survival behaviors that may be functional in the environment where the trauma has occurred, but which are dysfunctional in other environments. Fight, flight, or freeze are the words used to describe a person’s response to trauma. Behaviors such as running away, hitting, or lying can be functional as survival strategies but do not work in non-traumatic environments.
Trauma can cause developmental disabilities. All forms of trauma affect brain development. Trauma to the head itself, which may be diagnosed as a concussion or traumatic brain injury, can damage the brain, so that the full range of cognitive functions and adaptive skills are compromised. Childhood trauma is often linked to developmental delay across a several domains including cognitive functioning, as well as language and motor development.2
Children born with a developmental disability are more likely to be victims of trauma and are affected even more profoundly by that trauma. “Maltreatment of children with disabilities is 1.5-to-10 times higher than of children without disabilities.”3 And the difficulty they have in understanding, problem solving, and communicating can intensify the experience and the impact of the trauma.
The behavior in traumatized children, teenagers and young adults with developmental disabilities is often not recognized as trauma-related but is instead interpreted as “negative behavior” that stems from their disability and which needs to be controlled and modified. But we must understand that instead of the typical behaviors we see from youth without developmental disabilities who are traumatized - i.e., elopement, drug use, stealing and self-cutting, etc. – traumatized individuals with developmental disabilities are more likely to engage in face slapping, head banging, feces smearing, and self-stimulating behaviors. Once we understand this, we are more able to identify the presence of trauma and develop appropriate supports and interventions. Self-abusive behaviors are not always the result of trauma. Particularly in neurodiverse children with ASD, the behavior may be a response to stress or anxiety or to communicate when the child does not have verbal communication. It is important to conduct a full functional assessment as well as a social history to determine the reason for the behavior.
Treatment modalities
utilized for adults with PTSD are often not effective with individuals with
developmental disabilities. Cognitive Behavioral Therapy (CBT), an intervention
frequently used for adults, requires a level of interaction that persons with
developmental disabilities can find difficult or impossible. But Eye Movement
Desensitization and Reprocessing (EMDR), an evidence-based therapy that does
not require cognition-based interaction, can be effective. Other models of
therapy widely used to treat Developmental Trauma include play therapy, art
therapy, therapies using animals, occupational therapy, neurofeedback, various
approaches of developmental psychotherapy, and group activities ranging from
peer discussion groups to sports or singing.
Fetal Alcohol Syndrome (FAS) and lead poisoning
Both Fetal Alcohol Syndrome (FAS) and lead poisoning are conditions that affect brain development and can result in poor reasoning and judgement, difficulty with attention, impaired memory, irritability, deficits in adaptive behavior, or problems with socialization or self-regulation. A child may have these conditions without having a developmental disability diagnosis...and yet the challenges are the same. Recognizing the presence of either of these conditions is important to securing the right physical health services and behavioral health supports.
Doing What Works
Not all children with problematic behavior have experienced trauma nor do they all have both mental health and developmental disability diagnoses. However, so many children and youths with problematic behavior do have multiple diagnoses and trauma that we should make sure that social histories are exhaustive so that we can rule out conditions before we make assumptions.
Whether we identify trauma or the presence of a developmental disability, the interventions that work best for children with these conditions are also effective for all children and youth with complex behavior support needs.
First, “Don’t ask what the child is doing, ask what has happened to the child.”4 This quote from Dr. Daniel Hughes Ph.D. lays out the road we need to follow. Asking what has happened, when it happened, and for how long will lead to an understanding of both behavior and the best method of support. Trauma is so prevalent among children and youth with complex behavioral support needs, it would be wise to presume trauma and search the child’s records and social history to establish the event or events that may have caused trauma.
What was the trauma experience? Who were the perpetrators? What was the location? The answers to these and other questions are critical to developing a treatment plan and creating a trauma-informed environment. Knowing and consistently sharing with direct support staff the trauma history builds empathy. It helps support staff understand behavior. And empathy and understanding can motivate support staff to “stick with it” even when progress is slow or there are relapses.
A positive, healing environment
To be open to treatment, a child or youth must be receptive. Receptivity is dependent on a sense of comfort and trust. The environment should not present him or her with difficult sounds, experiences, stressors, or interactions, but should calm the flight/fight/freeze response. Making sure that nothing triggers that trauma-response is a place to start. The number of people the individual lives with and their behaviors will affect recovery. Providing a living arrangement with a small number of other residents has been effective for many. In instances of extreme behavior, an individual home provided for a period of time has been effective.
Effective teaching, treatment, and support interventions
The specific diagnoses of each child, teenager, or young adult should be the basis for the type of teaching strategies, treatment, and support approaches that are used. There is an array of options that may be used simultaneously: Trauma Focused Cognitive Behavioral Therapy (TF-CBT); Applied Behavior Analysis (ABA); individual therapy; social stories; group therapy; peer counseling; Internal Family Systems Therapy (IFST); Intensive Systems Therapy (IST); sex education and counseling; education about the mind and body; mindfulness training; Neuro Affective Relational Model Therapy; Dyadic Developmental Psychotherapy4, sensory interventions that calm: e.g., breathing exercises, weighted blankets, warm baths, swinging; Eye movement desensitization and reprocessing (EMDR); Bio/Neurofeedback; Neuro- Entrainment; Play Therapy; Art Therapy; Music Therapy; Psychodrama; Animal Therapy; Movement therapy (Yoga, Tai Chi, exercise); and group activities that involve movement with others – drumming, dancing, singing.
Staffing is the most critical component in the environment
Staffing ratios must allow for spontaneous, frequent, and responsive interaction. Staff must also be well trained to understand the individual’s experiences, the reasons for the behavior, and how best to interact. Direct care staff must be full members of the interdisciplinary team because their observations are important: they are the ones who spend time with the individual and so have the opportunities to help with recovery from trauma and the learning of new behaviors. Emotionally responsive caregiving will lead to positive change.
Children in Foster Care or Adoptive Families
As stated above, a significant percentage (38%) of children and youths who present as having complex behavior to the Department of Human Services have been in foster care or adoptive families. This raises the question: Are we providing adequate training and support for alternate families to assure success for the family and the child? Children with trauma - and often a diagnosed Reaction Attachment Disorder as well - can be wonderfully compelling to be with but also very difficult to live with. Training, in-home supports, and adequate respite care can be determinant factors. If the individual feels that “no one wants me” or that “I am not good enough to have a family” – this will add to his/her trauma history.
Routines and meaningful activity create stability
Routines that are predictable and reliable can reduce uncertainty and build inner stability. Routines that consist of enjoyable activities foster feelings of competence and success. Building on strengths and preferences increases self-confidence and self-esteem.
More good food and less bad food
This can be a significant challenge with teenagers. However, studies in brain science (the gut-brain connection) have revealed a significant connection between what we eat and how the brain works. Too much caffeine, sugar, and highly processed foods can trigger enzyme and hormonal reactions that interfere with thought processes, sleep, and self-control.
Making sure the individual has someone in his/her life who cares about them
Studies on resiliency have established that having an adult who cares is key. While treatment professionals and direct support staff can fulfil this role to an extent, it will be time limited. A treatment plan should include the identification of any permanent relationship and the strategies needed to nurture and support this relationship, such as: access to the internet, a phone for calling or texting, transportation, etc. The adult or adults who have this permanent relationship should be considered primary members of the interdisciplinary team.5
Individualizing rates
If the provider is to be responsive and to customize their program for a child or youth with complex behaviors, they must have support. We must also recognize that their costs may be greater than the standard reimbursement rate allows. An individually negotiated rate, based on the needs of the child or youth, which can be altered as those needs change, is essential.
And
to end: Recognize that you are in this for the long term
Older youth and young adults who have been in
numerous out-of-home living arrangements and treatment programs often have no
family to go back to and are not eligible for a medical facility. For those in
this situation, it makes sense to accept that: 1) work toward recovery may be
life-long and will require on-going supports and 2) a living arrangement that
will carry the youth into his/her adult years should be part of the planning
process. Temporary placements make for a feeling of homelessness and
hopelessness.
References
1. Zero to Three Website. ZERO TO THREE. Accessed November 21, 2021.
2. Van der Kolk BA. Developmental Trauma Disorder. Traumatic Stress Institute website. vanderkolk.indd (traumaticstressinstitute.org). Accessed November 21, 2021
3. Facts on Traumatic Stress and Children with Developmental Disabilities. National Child Traumatic Stress Network website. Microsoft Word - Traumatic Stress and Developmental Disabilities_final.doc (nctsn.org). Accessed November 21, 2021.
4. Hughes PhD D. Building Trust with Children who have been hurt in Relationships. PA Cares Partnership website. Daniel Hughes, Ph.D., Relations Between Complex Trauma and Attachment: How to build relationships | PA Care Partnership. Published June 2021. Accessed November 21, 2021.
5. Minnesota Longitudinal Study of Risk and Adaptation. University of Minnesota website. Minnesota Longitudinal Study of Risk and Adaptation. Accessed November 21, 2021.
Biography
Ms. Nancy Thaler served as the Executive Director of the National Association of State Directors of Developmental Disabilities Services (NASDDDS), as the Deputy Secretary for Pennsylvania’s Office of Developmental Programs and is currently serving as Senior Policy Advisor to the Administrator of the US Administration for Community Living. She has a master’s degree in Human Organization Science from Villanova University.
Contact Information
Nancy Thaler
Senior Policy Advisor
Administration for Community Living, U.S. Department of Human Services
Wong | 75-85
Volume 10 ► Issue 3► November 2021
Peer Support:
Innovative Models Across Systems and Populations
Mi-Yeet Wong
Abstract
Peer support utilizes the transformative power of lived experience to make an impact in people’s lives. This article provides brief background information on peer support services, emerging peer support models, and the future of peer support.
___
Introduction
A self-advocate once poignantly said during a conference session, that effective systems change happens when people who have the most to lose, are also the ones making the decisions. While the aim of that talk may have been focused on how effective systems change for racial equity should proceed, he was also conveying that lived experiences and stories are not only important, but powerful in creating change. The model of peer support services, which is based upon the value of lived experiences, and the philosophy for supporting individuals through shared understanding, are critical for systems change. In this article, background information on peer support services, emerging peer support models, and the future of peer support will be discussed.
Background of Peer Support
Peer support workers are “people who have been successful in the recovery process who help others experiencing similar situations. Through shared understanding, respect, and mutual empowerment, peer support workers help people become and stay engaged in the recovery process and reduce the likelihood of relapse.”1 Peer support workers engage in a myriad of activities in supporting others, including advocacy, sharing resources, building skills, fostering community and relationships, leading recovery groups, and mentorship and goal setting.1 There are foundational principles that guide the practice of peer support, including the philosophy that practice should be recovery-oriented, person-centered, voluntary, relationship-focused, and trauma-informed.1 These principles carry themselves across systems as well. For example, some of the very same values of the Everyday Lives Values in Action mirror these principles – person-centered decision making; the promotion of health, wellness, and safety; being able to trust the people that support you to honor and respect your right to make your own informed decisions.2
The history of peer support can be found in writings from the late 18th century when hospitals were hiring former patients to work in a psychiatric hospital as they were “…usually more gentle, honest and humane.”3 Since then, peer support has expanded to serve diverse populations, within a variety of treatment settings, and is recognized as an evidence-based practice that is Medicaid reimbursable.4 While peer support has its history in the mental health field, it has rapidly crossed systems, populations, and disciplines. In Pennsylvania, peer support has been used as a model to serve family systems, the criminal justice system, older adults, and individuals with developmental differences.
Family System
Family Peer Support Specialists use their lived experience as caregivers of children, youth or young adults experiencing emotional, behavioral, or co-occurring challenges.5 They support other parents or family members through activities such as empathetic listening and emotional support, navigating systems, providing information about systems or community resources, providing advocacy and support, and encouraging self-care activities, to name a few.5 When we talk about cross-systems successes, the importance of having Family Peer Support Specialists cannot be emphasized enough. Not only are Family Peer Support Specialists navigating family systems and dynamics, but they are also navigating community systems and resources. Family Peer Support Specialists are integral to service provision because they serve as a model for what successful collaboration can look like between systems and families, they can ease the demand placed on systems, and above all else, serve as a support for which families can turn to so that they know they are not the only ones navigating the challenges and that they too, can learn skills to care for themselves, advocate for their family members and even change the very systems that are not serving them.
Criminal Justice System
Peer Specialists can also be found within the justice system context. Forensic Peer Specialists are individuals with a history of mental health diagnosis and/or incarceration, who provide individualized support to others with psychiatric disabilities and criminal justice involvements.6 Forensic Peer Specialists create change by supporting people throughout their involvement in the criminal justice system, promote recovery principles including self-advocacy, advocate for their recipients, educate people about Mental Health Recovery and inspire hope by sharing their life experiences.6 Forensic Peer Specialists work in various settings including crisis intervention teams, state hospitals, emergency rooms, jails/prisons, community settings, and many other places that their recipients are. 6 They support individuals in understanding and navigating the criminal justice system, obtaining employment and housing, completing parole/probation requirements, reducing the time individuals stay in jail due to lack of community supports or basic needs, and identifying positive supports.7 As an example, the PA Statewide Forensic Peer Support Specialist Program is a project funded by the Pennsylvania Commission on Crime and Delinquency (PCCD) in cooperation with the Office of Mental Health and Substance Abuse Services (OMHSAS).8 Their collaborative efforts have included several entities, including Drexel University, and have thus far completed three 3-day forensic trainings for current peer specialists and a train-the-trainer workshop.8
Older Adults
Peer specialists also work with older adults with behavioral health issues on activities such as crisis support, development of community roles and natural supports, individual advocacy, self-help and self-improvement.9 The Certified Older Adult Peer Specialist (COAPS) Program is a partnership between the Center for Mental Health Policy at the University of Pennsylvania, the Office of Mental Health and Substance Abuse (OMHSAS) and the Pennsylvania Department of Aging (PDA).9 COAPS work with older adults in various settings including senior centers, senior housing units, and health clinics.9 COAPS teaches Certified Peer Specialists to support older adults on a variety of issues including physical and mental health, normal aging, cultural competence, anxiety, depression, trauma, substance use, stages of change and more.9
Developmental Differences
Peer support is a fundamental service of Centers for Independent Living, which are federally funded programs across the United States that offer community living supports for all individuals with disabilities.10 Additionally, with the peer support model being embedded across multiple systems and serving a variety of populations, it has also made its way to an innovative program called the Community Autism Peer Specialist (CAPS) Program which serves individuals on the Autism Spectrum.11 CAPS provides 75-hours of training (aligning with the Certified Peer Specialist model in the mental health system) which provides a foundation for the individual to become a peer support professional who also has the personal lived experience as individuals on the Spectrum. CAPS is the culmination of a partnership between many stakeholders and entities, including self-advocates, caregivers, peer specialists, provider, state, local, and university partners. CAPS works with participants on goals that the participant identifies as important to them, which may include community, employment, education, or advocacy goals. Beyond these goals though, is the impact of having someone with lived experience who works with a participant to build a mutual relationship, which can alleviate isolation and promote connection, communication, and goal development.
The Future
While the programs highlighted are only a few of the many models to support a variety of populations, they are nonetheless exciting to consider when we think about the transformative impact that peer support has had on people and systems. As we look to the future, these peer support models continue to meet a much-needed gap in service for individuals, employment opportunities that emphasize lived experience, and an asset to alleviate the workforce shortage crises in human services. With people reassessing what it is they want out of their employment, and with a poor unemployment rate among the disability population,12 peer support can create employment opportunities for people with lived experience while alleviating the demand placed upon systems. Some of these programs will work towards certification, others will work towards program expansion, and still others will work towards developing the capacity to measure outcomes and the impact of peer support. There is no doubt that as the importance of lived experience becomes increasingly salient, the evolution of peer support will continue to expand in dynamic ways across systems and environments.
References
1. Peers. SAMHSA Substance Abuse and Mental Health Services Administration website. https://www.samhsa.gov/brss-tacs/recovery-support-tools/peers. Last Updated: 09/29/2021. Accessed October 15, 2021
2. Pennsylvania Department of Human Services, Office of Developmental Programs. Everyday Lives: Values in Action. 2021. https://www.dhs.pa.gov/Services/Disabilities-Aging/Documents/Everyday%20Lives/Everyday%20Lives%CB%90%20Values%20In%20Action%20(c_241391).pdf. Accessed October 15, 2021.
3. Davidson L, Bellamy C, Guy K, Miller R. Peer support among persons with severe mental illnesses: a review of evidence and experience. World Psychiatry. 2012;11(2):123-128. doi:10.1016/j.wpsyc.2012.05.009.
4. Philadelphia Dept. of Behavioral Health and Intellectual Disabilities Services and Achara Consulting Inc. Peer Support Toolkit. http://dbhids.org/wp-content/uploads/1970/01/PCCI_Peer-Support-Toolkit.pdf. 2017. Accessed October 15, 2021.
5. PA Care Partnership County Collaborative monthly call. Family Peer Support Specialist a Pennsylvania Overview. https://www.pacarepartnership.org/uploads/County_Collaborative_Family_Peer_PowerPoint_11-27-18.pdf. Published November 27, 2018. Accessed October 15, 2021.
6. Baron R. Forensic Peer Specialists: An Emerging Workforce. Policy Brief June 11 Forensic Peers. http://www.pacenterofexcellence.pitt.edu/documents/Policy_Brief_Jun_2011%20Forensic%20Peers.pdf. Published June 2011. Accessed October 15, 2021.
7. Forensic Peer Support Project. Pennsylvania Mental Health Consumers' Association. https://www.pmhca.org/Forensic-Peer-Support Accessed October 15, 2021.
8. Statewide Forensic Peer Support Specialist Program. PMHCA. Pennsylvania Mental Health & Justice Center of Excellence. Drexel University. http://www.pacenterofexcellence.pitt.edu/documents/About%20FPS%20--%205_09_11.pdf. Accessed October 15, 2021.
9. COAPS Certified Older Adult Peer Specialists. http://olderadultpeerspecialists.org/why-coaps. Accessed October 15, 2021.
10. Salzer MS, Rogers J, Salandra N, et al. Effectiveness of peer-delivered Center for Independent Living supports for individuals with psychiatric disabilities: A randomized, controlled trial. Psychiatr Rehabil J. 2016;39(3):239-247. doi:10.1037/prj0000220.
11. Community
Autism Peer Specialist (CAPS) Program. Philadelphia Autism Project. https://www.phillyautismproject.org/peer/.
Accessed October 15, 2021.
12. Persons with a Disability: Labor Force
Characteristics - 2020. News Release. Bureau of Labor Statistics. U. S.
Department of Labor. https://www.bls.gov/news.release/pdf/disabl.pdf.
Published February 24, 2021. Accessed October 15, 2021.
Biography
TMi-Yeet Wong, LCSW works at the Policy and Analytics Center at the A.J. Drexel Autism Institute. Ms. Wong uses her prior experience as a Case Manager for adults with developmental differences to contribute to her current work in supporting individuals, their family members, and the community through program development and resource navigation.
Contact Information
Mi Yeet Wong,
Policy and Analytics Center (PAC), A.J. Drexel Autism Institute, Drexel University
3020
Market Street, Suite 560, Philadelphia, PA 19104
Phone Number: 215-571-3209