Positive Approaches Journal, Volume 11, Issue 1
| Site: | My ODP |
| Course: | My ODP |
| Book: | Positive Approaches Journal, Volume 11, Issue 1 |
| Printed by: | |
| Date: | Sunday, July 26, 2026, 8:17 PM |
Positive Approaches Journal | 6

Volume 11 ► Issue 1 ► May 2022
Innovation & Best Practices in Supporting Autistic Adults
Introduction
The modern proverbial saying, “You’ve met a person with autism, so you’ve met a person with autism,” could not be truer. Autism Spectrum Disorder (ASD) is many things; frustrating, misunderstood, and hard to read, but also literal, observant, focused. As an adult with autism, I can’t offer solutions for everyone. Many will say I am a success story and in some regards that may well be true. I can speak to how I think, how I perceive, and what I’ve done. I wasn’t diagnosed with autism until I was an adult. Finding supports and services for myself has never been consistent or easy. My emotions and my outlook constantly see-saw and I am constantly in a state of flux balancing the life I have with the life I want. I am cognizant of the fact that autism is not a diagnosis with a one size fits all solution or treatment. But I’m also able to articulate what works (for me) and what doesn’t. Not all adults with autism are so fortunate.
The current prevalence of autistic births – 1 in 44 – has garnered much attention for children with autism. All kinds of services involving early intervention, neurofeedback, and applied behavior analysis are available and focused on children. The list is endless. And what works for some, may not work for all. But what happens as those individuals age out of the children’s service system? They are met with an uncertain future, and not one that can be clearly defined or predicted. Autism as an adult is an entirely different world than autism as a child. For instance – the meltdowns. What do you do for an adult with autism who is melting down? Not a simple solution or a simple answer. A child might be comforted by their parents or caregivers. An adult screaming and crying in public is more apt to be asked to leave an establishment or worse, have the police involved. Pair that with many of the co-occurring disorders that can manifest in tandem with autism including depression, anxiety, intellectual disability, or epilepsy and the future gets fuzzier still. How can we reconcile successful treatments for adults with autism with the myriad forms that ASD can take? More specifically, how can we assist adults with all forms of autism to be a part of the world around them, to be accepted, celebrated, and embraced?
This issue of Positive
Approaches seeks to shed some light on adults with autism. The issue features
six articles dealing with the many sides of the autism picture. An article on
transgender identity and gender dysphoria highlights ways that adults with
autism can be supported and accepted while defining who they are. An article on
the Temple University Community Participation Measure and its success in
showing areas where adults with autism are spending their time; thereby giving
a clearer picture of where supports and services may best be provided. An
article on an adult with autism’s journey from work into retirement and how he
perceived this milestone. An article discussing Pennsylvania’s continuing
development of forward-thinking autism supports and services. An article on the
ongoing development and expansion of the Pennsylvania Department of Corrections
Neurodevelopmental Residential Treatment Unit. An article on the reasoning,
development, and success of the University of Pittsburgh Medical Center’s
(UPMC) Western Behavioral Health Psychiatric Rehabilitation (PR) program
carve-out program to serve autistic adults.
Six different sides to an equation with a spectrum of solutions. This issue of Positive Approaches should offer ideas, clarity, and hope. In the end, those of us with an ASD and those that support us will continue to help define success, understanding, and acceptance.
Hope Pesner
Human
Services Analyst
Office
of Developmental Programs
Positive Approaches Journal | 8-13
Volume 11 ► Issue 1 ► May 2022
Data Discoveries
The goal of Data Discoveries is to present useful data using new methods and platforms that can be customized.
Data can be a critical element of storytelling. But it is not the only chapter of the book. Data, coupled with narrative, can paint a comprehensive picture of how one person’s experience reflects the larger context of how many people may be experiencing something. Utilizing data to inform areas of focus, and feedback from autistic individuals, the Life on the Spectrum workshop series was developed. With funding from the Eagles Autism Foundation, the virtual workshop series sought input from autistic individuals with various backgrounds and interests, to inform the format and content of the virtual workshop series. Based on their feedback and guidance, the Policy and Analytics Center (PAC) at the A.J. Drexel Autism Institute, supported and implemented five workshops focused on:
1. Self-Advocacy
2. Navigating Higher Education
3. Sex Education and Dating
4. Autism in Women
5. Mental Health & Self-Care
It is common for informational trainings and workshops to be led by neurotypical people, but it was paramount that the Life on the Spectrum workshop series be different. Autistic self-advocates were involved from the very beginning of development
through execution of the series, positioning their needs, interests, and perspectives at the center of content development and delivery. A self-advocate is an individual with a disability or disabilities who speaks or acts “on their own behalf or
on behalf of other people with disabilities, whether the issue is personal (e.g., housing, work, friends) or related to public policy. 1” While some individuals may identify as a self-advocate, others may not. Despite how individuals may
identify, a common theme that arose was the mutual support that speakers offered one another, even as they were meeting for the first time. This is not surprising though, as research has illustrated that autistic people felt better understood2,
more belonging2, and experience good rapport3 when interacting with other autistic individuals as opposed to neurotypical people.
The data dashboard below shows theme-specific feedback and satisfaction with each session of the workshop series, as measured by attendee evaluation surveys. The first tab on the live site (Figure 1 below), ‘Life on the Spectrum Workshop Topics and Resources’ shows relevant resources and links where you can obtain more information.
Conclusion
To see a recording of the past sessions of Life on the Spectrum (note: some sessions were not recorded per the request of the presenters), please visit https://www.phillyautismproject.org/spectrum/. The videos are available with closed captioning and with subtitles in Spanish, Chinese, French, and Russian. The Policy and Analytics Center has been funded again by the Eagles Autism Foundation to develop another workshop series this year, focused on Aging and Autism. This theme was chosen based on feedback from participant surveys as well as autistic individuals who reach out voicing this need. If you want to be involved or learn more, please reach out to the Philadelphia Autism Project at phillyap@drexel.edu.
References
1. Self-Advocacy Position Statement | The Arc. The Arc. Published April 7, 2019. https://thearc.org/position-statements/self-advocacy/.
2. Crompton CJ, Hallett S, Ropar D, Flynn E, Fletcher-Watson S. “I never realized everybody felt as happy as I do when I am around autistic people”: A thematic analysis of autistic adults’ relationships with autistic and neurotypical friends and family. Autism. 2020;24(6):136236132090897. doi:10.1177/1362361320908976
3. Crompton CJ, Ropar D, Evans-Williams CV, Flynn EG, Fletcher-Watson S. Autistic peer-to-peer information transfer is highly effective. Autism. 2020;24(7):1704-1712. doi:10.1177/1362361320919286
4.
Self-Advocacy and Leadership. www.aaidd.org. https://www.aaidd.org/news-policy/policy/position-statements/advocacy. Accessed August 10, 2020.
5. Healthy People 2020 |. www.healthypeople.gov. https://www.healthypeople.gov/2020/. Accessed August 10, 2020.
Conner, Randall, Conroy, Cramer, Lubetsky | 14-25
Volume 11 ► Issue 1 ► May 2022
Psychiatric
Rehabilitation for Autistic Adults: Pilot Program Development
Caitlin M. Conner,
Ph.D.; Honor E. Randall, LCSW; Heather Conroy, LCSW; Ryan D. Cramer, LSW; &
Martin Lubetsky, M.D.
Abstract
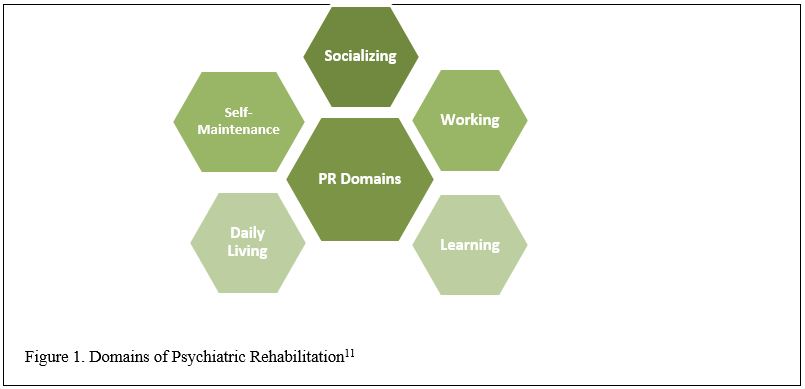
Beginning in 2013, the University of Pittsburgh Medical Center’s (UPMC) Western Behavioral Health Psychiatric Rehabilitation (PR) program began a carve-out program to serve autistic adults. PR is an approach developed for adults with severe and persistent mental illness that focuses on client-selected goals in Working, Learning, Social, Daily Living, and Self-Maintenance (Wellness) domains. This article will describe rationale for including autistic adults in PR and provide an overview of the PR carve-out.
Needs of Autistic Adults
Autism spectrum disorder (ASD) is defined as a neurodevelopmental diagnosis with social-communication impairments, the presence of restricted and repetitive behaviors and interests, and sensory differences.1 ASD is considered a lifelong
disability; however, most resources and research focus on childhood.2 Over a third of autistic people do not receive any support services after they complete high school.
3 The service needs of autistic adults have increasingly become a point of focus4, although each individual’s needs, just like autism itself, are quite variable.
Overall, studies show that autistic adults report a lower quality of life than non-autistic adults,5 although these traditional measures include independence and multiple social relationships, which may not be as important to all autistic adults. 6 Autistic adults are more likely to experience difficulties in obtaining higher education, finding and keeping employment, living independently and accomplishing daily living skills, and having successful social relationships. Compared to adults with other diagnoses, autistic adults are less likely to attend and complete post-high school education and vocational training.7 A national sample of adults 21-25 years old found that nearly half of autistic adults had never been employed.8 Many autistic adults have valuable work skills but struggle with the interpersonal skills needed to interview and keep their jobs. 9 Relatedly, a majority of young autistic adults do not live independently.10 Services that support autistic adults in these domains is desperately needed.
Psychiatric Rehabilitation (PR)
PR models arose following the deinstitutionalization movement of individuals with mental health diagnoses in the United States and Europe. PR models include Clubhouse, Peer Support, and Boston Model; all models emphasize self-determination, community
inclusion, and are person-centered and strengths based.11 PR was originally intended for adults with severe and persistent mental illness (SPMI), with the goal of keeping individuals in the community whenever possible and assisting
them with their self-defined goals and progress. PR does not offer medication management or psychotherapy for SPMI; rather, PR is meant to accompany other treatments that are maintaining mental health and are recovery oriented. In Pennsylvania,
SPMI is defined as schizophrenia spectrum disorders (schizophrenia, schizoaffective disorder), major mood disorders such as bipolar disorder and major depressive disorder, and borderline personality disorder.
The Boston Model of PR, which is used at the Psychiatric Rehabilitation program at the UPMC, focuses on five daily living domains: Working, Learning, Social, Daily Living, and Self-Maintenance (Wellness). Each client selects and works towards goals within these domains with the support of a counselor. Working with a counselor can take place in a typical clinic environment or out in the community, depending on the goal. PR also offers counselor- and peer-led groups in a variety of domains, which clients can choose to participate in.
UPMC’s PR Pilot Program
Seeing the parallels between the domains targeted in PR and the needs of autistic adults, we identified PR as a promising program to adapt for use in ASD. PR is a long-standing and widespread program in the US and Europe, which also lends promise to widely disseminate the program to more autistic adults. At UPMC, we created an ASD-specific carve-out within the existing PR program. We added an ASD-specialist counselor to provide individual counseling, ASD-specific groups, and training to all of the PR counselors and staff. Additionally, all autistic clients also had access to all other PR skills-learning and social groups that were offered at the site. ASD specialist counselors provided regular training to other PR counselors and staff about ASD and working with autistic adults to aid integration into all PR groups. Autistic clients were admitted to the PR program either due to having a cooccurring diagnosis considered an SPMI, or another mental health diagnosis deemed “an exception to medically necessary criteria” by a licensed professional of the healing arts (LPHA), such as licensed psychologists, psychiatrists, and primary care physicians. ASD alone was not considered an accepted diagnosis for billing insurance. We accessed medical records of all of the autistic clients to assess the success of this pilot program.
The ASD pilot program began at UPMC in 2013, and we assessed the medical data from autistic adults who participated in the program from 2013-2019. In that time, 53 adults ages 18-64 years old participated in the PR carve out. Besides a cooccurring psychiatric diagnosis, participants had to reside in Allegheny County to qualify for PR. PR is free to all clients who qualify. Typically, participants are referred to Psychiatric Rehabilitation programs by what is known as a LHPA. The term is limited to a physician, physician’s assistant, certified registered nurse practitioner and psychologist. The referral must be a written recommendation for psychiatric rehabilitation. Of the 53 participants, eight identified as female (15%), the majority were White (83%; four/7.5% each identified as Black or Asian), eight had a co-occurring diagnosis of Intellectual Disability, four (7%) were students, 14 (26%) were unemployed, and 24 (45%) lived with their families and were financially dependent.
All clients were required to attend individual counseling sessions (45% only attended individual sessions); ASD groups and all other PR groups were optional. On average, clients attended the PR program for about two years (Mean time at PR= 2.03 years).
Of the 53 participants, many received outside services too: 40 (75%) had outside psychiatric medication management, 20 (38%) had outside therapy services, 21 (40%) were receiving vocational rehabilitation services, 24 (45%) received social security
income or social security disability income (SSDI), and six (11%) were autism waiver recipients. During their time in PR, four clients (7%) were admitted for psychiatric hospitalizations.
Below are descriptions of each domain and examples of goals from each of the PR domains.12
|
Socializing
|
Working
|
Learning
|
Living
|
Self-
Maintenance
|
|---|---|---|---|---|
|
• making/keeping friends or romantic relationships
• verbal/nonverbal social skills across contexts
• boundary setting
• increasing community inclusion
Example goal: make one close friend I can trust in emergencies
Steps:
• identify & attend 3 social activities a month
• initiate conversation with a coworker each week
• attend weekly PR group
• work through barriers to interactions with PR counselors each week
|
• identifying potential employment
• applying, interviewing, preparing for, & maintaining employment
• communication skills with coworkers, asking for accommodations or recovering from poor performance assessments
Example goal: obtain part-time employment
Steps:
• identify one job to apply to each week
• update resume
• identify social expectations throughout job search
• practice interview skills & work through social barriers with PR counselor each week
|
• identifying & applying for educational programs based on strengths and realistic expectations
• using problem solving, organization, & comprehension techniques
• meeting social expectations needed for success
Example goal: maintain 2.5 GPA or higher
Steps:
• maintain & review calendar daily
• establish routine for studying, completing assignments, & attending office hours as needed
• request accommodations through disability services
• problem solve barriers to understanding materials, managing time, communicating with classmates & professors with PR counselor
|
• acquiring & maintaining independent living skills like paying bills, money management, food shopping & cooking, laundry, home maintenance
• managing calendar & time
• using public transportation/obtaining driver's license
Example goal: increase independence at home to prepare to live independently
Steps:
• create & maintain a budget for living expenses & savings
• learn to do laundry, respond to mail, & do dishes
• manage calendar of appointments & other activities
• work through barriers with PR counselor weekly
|
• keeping up with physical health, taking medication, hygiene & other activities of daily living
• diet & exercise
• mental health management, including crisis planning & wellness recovery action plans
Example goal: improve physical health as a means of improving mental health
Steps:
• identify a dentist & PCP who take my insurance & schedule an appointment
• get 30 minutes of exercise 3-5 days a week by taking brisk walks or attending yoga
• take all medications as directed daily
• work through barriers to regular exercise & taking medications with PR counselor week
|
The most popular goal domain was Social, with 80% of clients gaining skills, and Living had 78% of clients gaining at least one skill. In the Work domain, 72% of clients gained at least one skill, in Learning 67% of clients gained at least one skill,
and in Self-Maintenance, 36% of clients gained at least one skill.
Outcomes and Future Directions
UPMC’s PR program continues to host a carve out to serve autistic adults, and referrals to the program continue. We created a written training guide for PR programs to adapt to serve autistic adults. This training guide has been distributed at statewide PR and ASD conferences and is available free upon request. We have also conducted trainings as requested for PRs and healthcare agencies that are interested in incorporating autistic adults into their existing PR program or are interested in creating a PR program specifically for autistic adults. Future work includes continuing to encourage PR programs to incorporate autistic adults into their programs.
References
1. American Psychiatric Association. The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition: DSM-5. American Psychiatric Association; 2013.
2. Office of Autism Research Coordination. 2016 IACC Autism Spectrum Disorder Research Portfolio Analysis Report.; 2016. Autism Spectrum Disorder Research Portfolio Analysis Report 2016 | IACC (hhs.gov).
3. Shattuck PT, Wagner M, Narendorf S, Sterzing P, Hensley M. Post–High School Service Use Among Young Adults With an Autism Spectrum Disorder. Arch Pediatr Adolesc Med. 2011;165(2):1043-1049. doi:10.1001/archpediatrics.2010.279
4. Interagency Autism Coordinating Committee (IACC). Interagency Autism Coordinating Committee (IACC) Strategic Plan for Autism Spectrum Disorder 2018-2019 Update.; 2020. 2019 IACC Strategic Plan for Autism Spectrum Disorder Research | IACC (hhs.gov).
5. Ayres M, Parr JR, Rodgers J, Mason D, Avery L, Flynn D. A systematic review of quality of life of adults on the autism spectrum. Autism. 2018;22(7):774-783. doi:10.1177/1362361317714988.
6. Bishop-Fitzpatrick L, Hong J, Smith LE, Makuch RA, Greenberg JS, Mailick MR. Characterizing Objective Quality of Life and Normative Outcomes in Adults with Autism Spectrum Disorder: An Exploratory Latent Class Analysis. J Autism Dev Disord. 2016;46(8):2707-2719. doi:10.1007/s10803-016-2816-3
7. Newman L, Wagner M, Cameto R, Knockey AM, Shaver D. The Post-High School Outcomes of Young Adults with Disabilities up to 6 Years after High School. In: Encyclopedia of Special Education (eds C.R. Reynolds, K.J. Vannest and E. Fletcher-Janzen); 2011. doi:10.1002/9781118660584.ese1672.
8. Roux AM, Shattuck PT, Cooper BP, Anderson KA, Wagner M, Narendorf SC. Postsecondary employment experiences among young adults with an autism spectrum disorder RH: Employment in young adults with autism. J Am Acad Child Adolesc Psyshiatry. 2013;52(9):931-939. doi:10.1016/j.jaac.2013.05.019.
9. Hendricks D. Employment and adults with autism spectrum disorders: Challenges and strategies for success. J Vocat Rehabil. 2010;32(2):125-134. doi:10.3233/JVR-2010-0502.
10. Anderson KA, Shattuck PT, Cooper BP, Roux AM, Wagner M. Prevalence and correlates of postsecondary residential status among young adults with an autism spectrum disorder. Autism. 2014;18(5):562-570. doi:http://doi.org/10.1002/cncr.27633.
11.
Anthony W, Farkas M. A Primer on the
Psychiatric Rehabilitation Process. Accessed April 24, 2022. https://cpr.bu.edu/wp-content/uploads/2011/11/Primer-on-the-Psychiatric-Rehabilitation-Process.pdf.
12. Randall H, Conner CM, Z. Psychiatric Rehabilitation for Adults on the Autism Spectrum (guide/manual). ASERT Western Region, PA Department of Health and Human Services. 2019. Available upon request.
Biographies
Dr. Caitlin M. Conner, Ph.D., is a licensed clinical psychologist and researcher in the Department of Psychiatry at the University of Pittsburgh School of Medicine. Her work specializes in understanding and treating co-occurring mental health diagnoses in individuals with autism.
Heather Conroy, LCSW is a Licensed Clinical Social Worker and Executive Director/Co-Founder of Evolve Coaching, LLC, which focuses on providing specialized coaching support for education and employment for neurodiverse adults. She has expertise in working with autistic adults and served as one of the specialist autism counselors in the Psychiatric Rehabilitation project.
Ryan D. Cramer, LSW is the Program Director for Community Services within the Center for Autism and Developmental Disorders at UPMC Western Behavioral Health. He is also coordinator for the ASERT, Western Region. He is a Licensed Social Worker and has provided services and support to neurodiverse children, adolescents and adults and their families for the last twenty-eight years.
Martin J. Lubetsky, M.D., is Professor of Psychiatry at the University of Pittsburgh School of Medicine, and Senior Advisor of Child and Adolescent Psychiatry and Center for Autism and Developmental Disorders at UPMC Western Psychiatric Hospital. Dr. Lubetsky has worked in the clinical, training, administrative, and research areas of autism, developmental disabilities and child and adolescent psychiatry for over thirty-eight years. He provided diagnostic and clinical services to children, adolescents and adults with autism spectrum disorder, and intellectual disabilities with mental health issues. He has been active in developing awareness and support for the growth of community-based services. He is co-editor of the book Autism Spectrum Disorder, Oxford University Press, Inc.
Honor E. Randall, LCSW .is a Licensed Clinical Social Worker. She has expertise in working with autistic adults and served as one of the specialist autism counselors in the Psychiatric Rehabilitation project.
Contact Information
Caitlin M. Conner, Ph.D.
Research Assistant Professor
University of Pittsburgh School of Medicine
(412) 246- 5975
Heather Conroy, LCSW
Evolve Coaching, LLC
Executive Director/Co-Founder
Ryan D. Cramer, LSW
Program Director
University of Pittsburgh Medical Center
Martin Lubetsky, MD
University of Pittsburgh School of Medicine
University of Pittsburgh Medical Center, Western Psychiatric Hospital
Professor of Psychiatry; Senior Advisor, Child & Adolescent Psychiatry and the Center for Autism and Developmental Disorders; Director, Autism Services, Education, Resources and Training (ASERT), Western PA Region
Honor E. Randall, LCSW
Fraser | 26-38
Volume 11 ► Issue 1 ► May 2022
Autistic and
Transgender: Support at the Intersection
Cori L. Fraser, LSW
Abstract
It has been known for
at least the last decade that gender dysphoria seems to be more prevalent among
autistic people than in the general population.1 While
this has led to a great deal of speculation about the potential for shared
etiologies in the literature2,3, until recently, there has been very
little published regarding the support of individuals who are both autistic and
transgender. This manuscript attempts to begin to correct this dearth by
addressing the needs of autistic and transgender individuals through a novel
combination of evidence-based intervention for both autistic and transgender
individuals, clinical experience, and the lived experience of the author, an
autistic and transgender social worker working primarily with autistic and
transgender adults in Pittsburgh, Pennsylvania.
A Note on Language
This document uses identity-first language to refer to autistic and disabled people per the American Psychological Association’s 2021 guidance4 as well as author preference. Additionally, transgender identity and diagnosis of gender dysphoria are used interchangeably herein despite the fact that, some individuals with gender dysphoria may eschew the transgender label or choose not to pursue gender transition.
Background
Since the early 2010s, a number of studies have found that autism is many times more prevalent in populations being treated for gender dysphoria1 and that gender variance is much more common among autistic people.2 This data, as well as the widespread experience of individuals living at this intersection and their networks of support, reflect an urgent need for tools for our supporters, both formal and informal, and a roadmap that individuals in need of support can use to advocate for the implementation of a best practice model to meet their needs. This call-to-action is especially urgent given extant research on the intersection of disability and transgender identity which shows that disabled transgender individuals are more likely to face discrimination when attempting to access mental health centers (17.3% v. 6.2% of transgender people without disabilities), drug treatment programs (4.7% v. 2.0%), rape crisis centers (7.8% v. 3.3%), and domestic violence shelters (9.9% v. 3.5%).5 Further, there is overwhelming data reflecting that transgender individuals are much more vulnerable to suicidal ideation and completed suicide than cisgender peers and suicide risk is vastly decreased by having a supportive family or, in the case of youth, a single supportive adult.6,7
Supporting Autistic
Transgender Individuals
Identify and treat gender dysphoria
The standards of care for gender dysphoria are published by the World Professional Association for Transgender Health. Clinicians working with transgender individuals, regardless of neurotype, should be at least passingly familiar with the most current Standards of Care for the Health of Transsexual, Transgender, and Gender Nonconforming People. As of the seventh version of this document, published in 2012, WPATH recommends a largely informed consent approach to treating gender dysphoria, including among disabled people.8 That is, it advocates that individuals who express gender dysphoria and who are able to meaningfully consent to the risks of intervention to have access to those interventions. An important note here, while “gender dysphoria intervention” often means irreversible interventions such as surgery or hormone therapy, interventions also include fully reversible steps such as using a different name or pronouns, experimenting with wardrobe and hairstyle, and socially embodying the individual’s target gender.
Hormone therapy and surgery
Often discussions around
transgender identity delve into the particulars around gender affirming hormone
replacement therapy (HRT) and gender confirmation surgery (GCS) as well as
puberty suppression for adolescents. This discussion is particularly important
as these interventions carry significant weight as the only long-term,
evidence-based interventions for gender dysphoria, and later regret associated
with these interventions is exceedingly rare.9 There is evidence
that these interventions are literally lifesaving for many transgender
individuals, as they greatly reduce suicidality in this population.10,11
Further, puberty suppression is fully reversible12 and there is
significant evidence that puberty suppression leads to radically lower odds of
lifetime suicidal ideation and attempts.13
While many parents and providers present concerns that HRT and GCS are irreversible and individuals may later come to regret these decisions, supporters of Autistic transgender individuals must critically consider the evidence that these interventions increase wellbeing and decrease severe depression and suicidality in the vast majority of individuals who receive them.
Autism and gender identity
While it is well established that transgender identity is more prevalent among autistic individuals, that does not mean that this overlap is always simple or easily identified.14 Transgender identity can be easily dismissed as a trait of autism by family or clinicians without transgender or autism expertise. Further, due to the propensity for autistic people to have more rigid patterns of thinking (“black-and-white thinking”), autistic people may struggle to identify their gender struggles, and cognitive flexibility issues may make it difficult for them to understand gender as potentially fluid or changeable. Executive function difficulties and struggles with future thinking may also make it difficult to assess for understanding and informed consent associated with interventions. Impairments of verbal speech can also add a confounding factor. While these issues may mean that some autistic individuals recognize their gender differences later in development than non-autistic peers, they should not be understood as limiting access to identity or intervention, especially when interest in gender transition/exploration or expression of gender dysphoria is enduring over time.
Recognize minority stress
The minority stress model proposes that stigma, discrimination, and hostile social environments produce the higher rates of distress and mental health disorders seen among minority populations.15 This model can be applied to both autistic people16 as well as transgender individuals. In fact, transgender autistic individuals often report a high degree of alienation from both the autistic and Lesbian, Gay, Bisexual, Transgender and Questioning+ (LGBTQ+) communities, where the autistic community and autism supports do not understand their transgender identity and the LGBTQ+ community has misconceptions about their autistic identity.17 Moreover, there is evidence that individuals living at the intersection of autism and disability experience a higher degree of discrimination5 and violence18 across contexts.
Naming the structures
Psychoeducation is a central aspect of support for any population, but for autistic individuals, this can be of additional importance due to the prevalence of social isolation and the tendency for cognitive rigidity.19 For many, access to the language to describe their internal experience of gender may be entirely novel. Additionally, by helping individuals locate internalized oppression (ableism, transphobia) as a problem with society rather than a problem within themselves, supporters can help individuals understand their struggle in the context of an unjust society, improving their self-concept and helping them build the internal model required for self-advocacy.20 When support is built on a foundation of anti-oppressive practice, individuals are enabled to build a self-image independent from a societal narrative that frames disabled and transgender people as broken, inferior, or deviant.
Address Disability Needs
While gender dysphoria is often deeply distressing and urgent to address for individuals, disability supports must be maintained for individuals as they transition. Executive function, social skills, and emotional support are particularly important during gender transition.20 Gender transition may mean managing new medications, grooming routines, medical appointments, and relationships with doctors, therapists, and peers, as well as managing new or previously suppressed feelings around the body, sexuality, and the experience of moving through the world in a new social role. Further, while not reflected in the literature, individuals may find themselves ready to process trauma that was previously unexplored when their gender dysphoria is adequately controlled, and they are able to establish safety in their body. This means that support around disability needs must be maintained through gender transition. However, stability should not be a limiting factor in access to transition, as the alleviation of gender dysphoria may actually improve overall wellbeing and reduce behaviors associated with distress.
Connect with
Community
Chosen family has long been a central aspect of LGBTQ+ community. Historically, LGBTQ+ people formed chosen families as a survival strategy in the face of rejection from their families of origin. However, as familial rejection has become rarer in most communities, chosen familial has served a complementary role to the family of origin.20 These constructed families are particularly important to the community due to their roles in providing help navigating systems, providing emotional support, and providing mutual aid. By connecting individuals with autistic and transgender community, supporters give individuals access to social connection, mutual support, and shared experience that can help individuals understand their own journeys.14
Support the
Supporters
Both formal and
informal supporters must also have supportive spaces to learn, share, and seek
advice. Ideally, this includes teaching on a range of topics associated with
the intersection of autism and transgender identity, the sharing of medical and
legal resources, and spaces where supporters can consult others supporting
individuals navigating similar identities.14 This is especially
important for families of individuals who are living in their family home or
who are under legal guardianship.
When family is not supportive
There is a fundamental
challenge when an individual is under the age of majority, financially
dependent, or under guardianship of family members who are not supportive of
their transgender identity. This is made especially complex given the high
rates of severe depression and suicidality seen in autistic and transgender
people without access to transition. Education remains the most effective tool
in these situations, as many families simply lack information about diverse
gender identities.22 However, some families may experience a strong
negative reaction to this information about their children, up to and including
mourning as if the transgender individual had died. These families may need
time to process their grief for the future they envisioned for their child as
they learn more about what it means to be transgender. Other families may
experience difficulty reconciling their child’s identity with an ideology or
religious belief, and in some cases, the families can be connected with
affirming communities within their faith.
Over time, many, but not all, families will
develop the cognitive flexibility, understanding, and connections they need to
gain comfort with their child’s identity. For families that are not able to
adapt in this way, it can be important for the individual’s wellbeing to
maintain affirming contact with them to the extent possible. That is,
supporting the individual in exploring and expressing their gender identity to
the extent that is safe while they are in an environment that is not affirming.
Continuing education
For formal supporters, continuing education and training is indispensable. It has only been in the past two decades that research and standards regarding transgender health have rapidly developed and in the last five years that the intersection of transgender and autistic experience has received attention. While there remains a dearth of information, there has been a rapid proliferation of research regarding this population—organizations such as the Academic Autism Spectrum Partnership in Research and Education and the Autism Intervention Research Network on Physical Health are utilizing community based participatory research to work with autistic and transgender individuals to develop supports for this underserved population.
Direct support workers and intersectionality
This discussion would not be complete without an acknowledgement that direct support workers (DSPs) in Pennsylvania are disproportionately women, disproportionately Black and Brown, and disproportionately live in poverty and rely on public assistance.23 In order for these supporters to be able to implement these recommendations in their day-to-day work with autistic transgender individuals, they must, themselves, have the tools they need to thrive. This means that dismantling structural racism, ableism, and transphobia in direct support organizations, legislating fair wages and benefits DSPs, and creating more affordable, high-quality childcare, are indispensable parts of supporting autistic and transgender individuals.
Conclusion
Individuals living at the intersection of transgender identity and autism face a number of challenges, compounded by oppression, familial and community rejection, and mental health complications. Through access to affirming care, education, disability supports, authentic community, and chosen family, and continuing education and support for their support workers, autistic transgender people can build the support they need to thrive.
References
1. de Vries ALC, Noens ILJ, Cohen-Kettenis PT, van Berckelaer-Onnes IA, Doreleijers TA. Autism Spectrum Disorders in Gender Dysphoric Children and Adolescents. Journal of Autism and Developmental Disorders. 2010;40(8):930-936. doi:10.1007/s10803-010-0935-9.
2. Jones RM, Wheelwright S, Farrell K, et al. Brief Report: Female-To-Male Transsexual People and Autistic Traits. Journal of Autism and Developmental Disorders. 2011;42(2):301-306. doi:10.1007/s10803-011-1227-8.
3. Strang JF, Kenworthy L, Dominska A, et al. Increased Gender Variance in Autism Spectrum Disorders and Attention Deficit Hyperactivity Disorder. Archives of Sexual Behavior. 2014;43(8):1525-1533. doi:10.1007/s10508-014-0285-3.
4. Disability. https://apastyle.apa.org. https://apastyle.apa.org/style-grammar-guidelines/bias-free-language/disability. Accessed April 1, 2022.
5. Kattari SK, Walls NE, Speer SR. Differences in Experiences of Discrimination in Accessing Social Services Among Transgender/Gender Nonconforming Individuals by (Dis)Ability. Journal of Social Work in Disability & Rehabilitation. 2017;16(2):116-140. doi:10.1080/1536710x.2017.1299661
6. Ryan C, Russell ST, Huebner D, Diaz R, Sanchez J. Family Acceptance in Adolescence and the Health of LGBT Young Adults. Journal of Child and Adolescent Psychiatric Nursing. 2010;23(4):205-213. doi:10.1111/j.1744-6171.2010.00246.x.
7. The Trevor Project. National Survey on LGBTQ Mental Health. New York, New York: The Trevor Project, 2019.
8. World Professional Association For Transgender Health. Standards of Care for the Health of Transsexual, Transgender, and Gender-Nonconforming People. World Professional Association For Transgender Health; 2012.
9. CM W, NM N, CJM de B, et al. The Amsterdam Cohort of Gender Dysphoria Study (1972-2015): Trends in Prevalence, Treatment, and Regrets. Yearbook of Paediatric Endocrinology. Published online September 11, 2018. doi:10.1530/ey.15.6.4
10. Akhavan AA, Sandhu S, Ndem I, Ogunleye AA. A review of gender affirmation surgery: What we know, and what we need to know. Surgery. 2021;170(1):336-340. doi:10.1016/j.surg.2021.02.013.
11. Green AE, DeChants JP, Price MN, Davis CK. Association of Gender-Affirming Hormone Therapy With Depression, Thoughts of Suicide, and Attempted Suicide Among Transgender and Nonbinary Youth. Journal of Adolescent Health. 2021;70(4). doi:10.1016/j.jadohealth.2021.10.036.
12. Hembree WC, Cohen-Kettenis PT, Gooren L, et al. Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society* Clinical Practice Guideline. The Journal of Clinical Endocrinology & Metabolism. 2017;102(11):3869-3903. doi:10.1210/jc.2017-01658.
13. Turban JL, King D, Carswell JM, Keuroghlian AS. Pubertal Suppression for Transgender Youth and Risk of Suicidal Ideation. Pediatrics. 2020;145(2). doi:10.1542/peds.2019-1725.
14. Strang JF, Knauss M, van der Miesen A, et al. A Clinical Program for Transgender and Gender-Diverse Neurodiverse/Autistic Adolescents Developed through Community-Based Participatory Design. Journal of Clinical Child & Adolescent Psychology. Published online May 6, 2020:1-16. doi:10.1080/15374416.2020.1731817.
15. Meyer IH. Prejudice, Social stress, and Mental Health in lesbian, gay, and Bisexual populations: Conceptual Issues and Research evidence. Psychological Bulletin. 2003;129(5):674-697. doi:10.1037/0033-2909.129.5.674.
16. Botha M, Frost DM. Extending the minority stress model to understand mental health problems experienced by the autistic population. Society and Mental Health. 2018;10(1):215686931880429. doi:10.1177/2156869318804297.
17. Hillier A, Gallop N, Mendes E, et al. LGBTQ + and autism spectrum disorder: Experiences and challenges. International Journal of Transgender Health. 2019;21(1):98-110. doi:10.1080/15532739.2019.1594484.
18. Messinger AM, Guadalupe-Diaz XL, Kurdyla V. Transgender Polyvictimization in the U.S. Transgender Survey. Journal of Interpersonal Violence. Published online August 31, 2021:088626052110392. doi:10.1177/08862605211039250.
19. Strang JF, Meagher H, Kenworthy L, et al. Initial Clinical Guidelines for Co-Occurring Autism Spectrum Disorder and Gender Dysphoria or Incongruence in Adolescents. Journal of Clinical Child & Adolescent Psychology. 2016;47(1):105-115. doi:10.1080/15374416.2016.1228462.
20. Baines D. Beyond the Social Model of Disability. In Doing anti-oppressive practice: Social Justice Social Work. Fernwood Publishing; 2017: 153–171.
21. Jackson Levin N, Kattari SK, Piellusch EK, Watson E. “We Just Take Care of Each Other”: Navigating “Chosen Family” in the Context of Health, Illness, and the Mutual Provision of Care amongst Queer and Transgender Young Adults. International Journal of Environmental Research and Public Health. 2020;17(19):7346. doi:10.3390/ijerph17197346.
22. Abreu RL, Rosenkrantz DE, Ryser-Oatman JT, Rostosky SS, Riggle EDB. Parental reactions to transgender and gender diverse children: A literature review. Journal of GLBT Family Studies. 2019;15(5):461-485. doi:10.1080/1550428x.2019.1656132.
23. Pennsylvania Long-Term Care Council. A blueprint for strengthening Pennsylvania’s direct care workforce. Retrieved from: https://www.aging.pa.gov/organization/PennsylvaniaLongTermCareCouncil/Documents/Reports/LTCC_Blueprint%20for%20Strengthening%20Pennsylvania%E2%80%99s%20Direct%20Care%20Workforce_April2019.pdf. Accessed April 1, 2022.
Biography
Cori Frazer is a multiply disabled, nonbinary licensed social worker (LSW) and activist. Having worked in progressive organizing since they were a teen, they have spent the last decade working to help build strong, vibrant queer and disabled communities. Co-founder of the Pittsburgh Center for Autistic Advocacy (PCAA), Cori’s work is reflective of their deep belief in interdependence and liberatory praxis. Under Cori’s leadership and practice of innovative models of community support and mutual aid, PCAA has served hundreds of disabled adults in western and central Pennsylvania.
Contact Information
Cori L. Fraser, LSW
Pittsburgh Center for Autistic Advocacy
Executive Director
Knauss | 39-44
Volume 11 ► Issue 1 ► May 2022
A Reflection on Retirement from Someone on the Autism Spectrum
Dave Knauss
In October 2019 at my last job with the Commonwealth of Pennsylvania (COPA), I was asked to write an article on my office’s recognition of Breast Cancer Awareness Month (October), for the Department of Human Services’(DHS) website. Given that I was already quite involved in this awareness activity and that I liked to write, and that my own biological mother, Marion, died from breast cancer in 1963, this was a natural assignment for me. Whether this task for me was paid or unpaid, it was for a cause that I believed in. It was work – work toward helping others and contributing.
In April 2021, I retired from my career of 29 years with the State. I am still doing work to help others, albeit unpaid and part-time. Retirement for me was not a transition from full-time work to a life of total leisure. It was a transition to a new period of my life that combines work, relaxing, family time, some travel, and more writing.
In this essay, let me examine my transition into retirement, why I am still doing volunteer work, how I feel about work, and how I balance the above elements in my life.
First, the basics. I am 67 and have been married to my wife, Connie, for 36 years. We have three married daughters, and seven grandchildren. From 2007 to 2019, I served as the volunteer leader of a support group for adults with autism spectrum disorder (ASD), Spectrum Friends of Lebanon County. I ventured into this support group because in 2003 I was diagnosed with Asperger’s Syndrome.
As most people know who have been around individuals with ASD, anxiety is a constant companion for many. It is certainly true for me. Part of my anxiety is that I am a high energy person. I like to work as an outlet for that energy. Consequently, I have always put in that “extra effort” on my jobs. I like doing a good quality job, I like helping others and I like to produce good results.
Work for me is also an outlet for my creativity. I am an idea person, and I am a self-starter. Sharing my ideas at work and in community organizations has been good, and not so good. Not everyone in organizational life likes a person who is somewhat outspoken and looks at life from a critical angle, like I do – perhaps like many individuals with ASD do. As a result, I have found that I do my best work when I have a lot of freedom. Freedom to be creative. I like being the hands-on person in charge of the project or program. Consequently, I have done quite a bit of good work as a volunteer in the community in the last 42 years, since it is easier to be a volunteer than a paid employee. No one needs to pay me.
Bottom line, I have always liked to work, whether it was paid or unpaid.
I first started thinking about retirement in 2012, when I was not very fulfilled at my job with the State. I was 57 at the time, and I knew that 60 is the normal retirement age for State employees. I got to thinking, is there a better way to use my time? Are my wife Connie and I okay financially for me to retire at age 60?
Fortunately, in 2014 I was able to transfer to another agency within the DHS, thanks to a good State contact within DHS, someone who came to meetings I did staff work on and who was later promoted to Supervisor. He had an opening, let me know, and hired me. I am forever grateful. That move made me postpone retirement.
I have to admit something – about eight years ago, I had a nightmare that originated from a fear I had of retirement. It was a little scary, the thought that retirement and I might not be a good match. I have always remembered that. But, as a way to get me ready for the inevitable, I started reading articles about retirement. I tried to do planning on what I would do with my time. I knew I had to keep doing work of some kind, whether or not I was compensated.
Years ago, I came across an article about retirement that said, new retirees have a lot of time on their hands. Perhaps TOO much time. The article said some retirees suffer from depression. I did not want to encounter mental or emotional difficulties after I retired. There was one State employee who retired from the State but then came back to State service – in my office around 2012. In retirement, he said, he attempted unsuccessfully to launch a new career in the private sector; but he became depressed. So, he came back to the State, and after about a year and a half, he retired a second time.
His experience prompted me to do more planning for retirement. One concept I had is that, with retirement, I could branch out with the ASD support group I led, do more activities, spend more time helping various individuals with ASD one on one. That was a good concept. Actually, I have not planned and led any support group activities since COVID started interrupting our lives in March of 2020.
However, in retirement, I am still involved on a continuous basis with two autism-related organizations – this Positive Approaches journal as a member of the editorial board, and the annual Pennsylvania Autism Training Conference (PATC). In addition, following retirement I served as a panelist for discussions at three autism-related events in 2021, and I was a participant on another panel discussion this past March 30 for the Autism in the Courts Taskforce Summit (sponsored by the Supreme Court of Pennsylvania).
I have also continued volunteer work with my church. And, at the request of their single mother, I am an adult mentor – somewhat of a father figure – to two teen-aged girls and their 20-year-old sister who apparently haven’t seen their biological father in about 10 years. Additionally, I am trying to obtain a volunteer position on the Parks and Recreation Board of my township. And my wife, Connie, and I are quite involved with our seven grandchildren, doing more field trips with them and, sometimes, their mothers.
These volunteer activities are important to me, not just because I enjoy them but also because they fulfill in me that sense of pursuing social justice – which is something that many individuals with ASD feel, according to my research. I also want to serve and love God by serving and loving others; I want to do evangelism. I believe I have a purpose in life, a reason to get out of bed in the morning.
These activities, along with spending more time with my wife, Connie, and our seven grandchildren, are keeping me busy. Some people will ask, when are you going to … just relax? After all, you’re retired. Well, I don’t want to just read books or watch (infamous) Jerry Springer all day or play golf. On the other hand, I have to watch that I don’t get overextended. My first priority has to be my wife and my family. Unless I have a prior commitment, I never turn down opportunities for family time with our children and grandchildren. Connie and I do a lot of things together, such as taking a walk every day and doing more errands together. She does some volunteer work with me.
Why do some people retire from paid (and possibly unpaid) work by age 49, like my friend Tim in Colorado, while others work into their 70’s, 80’s or even 90’s? Some enjoy working, some want to keep making a difference in the lives of others, some do it to make more money. Some want to make an impact before their time is up.
I think retirement is all an individual thing. I tell myself this – Work may be four letters long, but it is NOT a “four-letter word” in the negative sense that SOME words are.
When I was working full-time, I remember a time when my former coworker, Amber, and I picked up another coworker, also named Dave, for a lunch at a Harrisburg restaurant. He was retired and said, smiling broadly, “every day is like a Saturday.” Personally, I do NOT hate work. I actually envy people who have jobs they love.
I believe this is the essential question – how do you want
to use your time?
For me, work is still an important part of how I want to use MY time. I am only 67, am healthy and have lots of experience and skills, so why waste them? I also realize that I’m not a very relaxed person. Whether that’s good or bad, I don’t know. But that is my personality, which has been shaped in part by my ASD. So, it means that, in retirement, I need to keep working on projects and programs. For my own sake and hopefully to help other people as well.
Biography
Dave Knauss is retired following a career of 29 years in Pennsylvania State Government. He served as an Income Maintenance Caseworker for 12 years at the Berks County Assistance Office. He also served as a Human Services Program Specialist doing policy work at the Office of Medical Assistance Programs and doing quality assurance work at the Office of Long-Term Living. His career also includes ten years as a reporter and editor at three newspaper organizations in central Pennsylvania. He has a Bachelor of Arts degree in American Studies from Dickinson College. From 2007 to 2019 he served as the volunteer leader of a support group for adults with ASD, Spectrum Friends of Lebanon County. He was diagnosed with Asperger Syndrome in 2003. While his ASD is just a small part of his identity, he believes his ASD is a gift.
Malishchak | 45-54
Volume 11 ► Issue 1 ► May 2022
Enhancements of Identification and Service Delivery to Individuals with Neurodevelopmental Needs within the Pennsylvania Department of Corrections (DOC)
Lucas D. Malishchak,
DBA
Abstract
The Pennsylvania DOC’s Psychology Office recently broadened its system’s process of identifying and treating neurodevelopmental disorders beyond intellectual disabilities, to include those individuals living with autism spectrum disorder (ASD). This improvement is reflective of the Psychology Office’s more comprehensive clinical operational plan of augmenting identification efforts and enhancing service delivery. This article will outline additional components of the DOC’s statewide clinical operational plan, which includes an overview of the ongoing development of a Neurodevelopmental Residential Treatment Unit.
___
To ensure incarcerated people have adequate access to mental health care, the American Correctional Association indicates that correctional mental health care systems must, at a minimum (i.e., among many other processes and assurances), ensure that each incarcerated person receives appropriate mental health care to assist with the restoration, recovery, and maintenance of each person’s mental wellbeing during their period of incarceration.1 In light of this standard of care, the PA DOC’s Psychology Office annually reviews internal correctional mental health care policies. During a recent annual policy review, which included a field survey of the DOC’s more than 300 front line psychology staff on their knowledge, experience, and skills working with patients diagnosed with neurodevelopmental needs, the Psychology Office leadership team identified the need to enhance systemic identification and treatment efforts of people who may be living with neurodevelopmental needs, beyond intellectual disabilities. Additionally, the team identified that training efforts of clinical staff in these areas were also needed. As a result, the Psychology Office leadership team developed a plan of action to guide these focused enhancements. The following paragraphs will briefly outline several components of this plan and describe the systemic efforts aimed at enhancing access to care for this population.
To best understand the progress made by the DOC over the past few years, it is essential to understand historical clinical processes used to identify and treat neurodevelopmental disorders within the Pennsylvania DOC. In January of 2015, the DOC signed a landmark settlement agreement with Disability Rights Pennsylvania2. The core issue of this settlement agreement included but was not limited to the identification of individuals with serious mental illnesses and other vulnerabilities, including intellectual disabilities, and their diversion from restrictive housing, among numerous other relevant clinical and operational safeguards for this population. The original group of individuals identified to benefit from the new safeguards, while progressive and sizeable, did not specifically include individuals living with other neurodevelopmental disorders like ASD. As a result, two recent revisions that occurred in 2020 included the mandatory training of all DOC psychology staff on the identification and treatment of individuals with neurodevelopmental needs and the inclusion of patients diagnosed with ASD into the known classification of mental health patients that receive the highest clinical and operational safeguards within the DOC.
Mandating annual training on neurodevelopmental disorders and reclassifying individuals with ASD were two straightforward revisions. However, training would need to continue, and the reclassification merely ensured identified patients would be afforded the above referenced safeguards. Unfortunately, at that point in time, the DOC had less than 15 patients (i.e., out of approximately 40,000) diagnosed with ASD or less than .05% of their population. In light of the known prevalence of ASD reaching approximately 1%3, the Psychology Office needed a more comprehensive internal screening and diagnostic process responsive to both the varied intercepts of reception into the DOC and responsive to those patients already living within the system. From early 2020, the Psychology Office continued incorporating additional clinical advancements beyond the original safeguards outlined in DOC policy. Initially, the team identified the need to augment the initial reception screening process (i.e., of all new receptions into the DOC) to include the Autism Quotient-104, a neurodevelopmental screening tool sensitive to identifying signs and symptoms of ASD. By incorporating the Autism Quotient-10 (AQ-10)4 at initial reception, the DOC ensured new and future receptions into the DOC were screened for ASD, thereby enhancing the ability to identify neurodevelopmental needs of the incoming population. However, adding a brief neurodevelopmental screen to the initial reception process could not be introduced without a more thorough and complementary diagnostic process to address those who screened high on the AQ-104. Consequently, as part of their comprehensive approach to improving the identification of ASD, the Psychology Office developed an internal ASD diagnostic protocol, as well. This protocol was developed through the guidance and leadership of the Psychology Office’s four Regional Licensed Psychologist Managers and Administrative Officer, with input and feedback from Licensed Psychologist Managers (LPMs), Psychological Services Specialists (PSSs), and Psychological Services Associates (PSAs) throughout the DOC. The initial screening protocol and differential diagnosis protocol also required integration into the DOC’s electronic health record, as well. Once integrated into the electronic health record’s practice and testing environment, field clinical staff were able to experiment with these tools and provide feedback to developers and clinical leaders for the purpose of enhancing user-friendliness, clinical utility, etc. This information was then used to further improve documentation processes before the new protocols went operationally live.
Once developed and tested, the initial screening and follow up diagnostic process still could not begin without first ensuring DOC clinical staff were adequately trained. To accomplish this task, all 277 master’s level Psychology staff members and their Licensed Psychologist clinical supervisors required training on the AQ-104 and the diagnostic interview protocol. Here, the Psychology Office’s four Regional LPMs trained the DOC’s 27 LPMs on the utilization of the AQ-104 and the diagnostic protocol. Once trained, the LPMs trained their 277 front-line PSAs and PSSs. Including these new initial reception products together into existing DOC mental health care processes, advanced the organization’s ability to identify neurodevelopmental needs of the incoming population. However, despite this early work, these new processes merely ensured that all newly arriving receptions were screened for ASD, and that, if clinically indicated, a follow up diagnostic and clinical interview process would occur. Following the promulgation of the enhanced reception product, the Psychology Office brainstormed the most efficient and effective method of screening and identifying individuals currently living in the DOC who may have undiagnosed neurodevelopmental needs.
Screening the entire DOC population for ASD was neither practical nor clinically appropriate. Instead, the Psychology Office clinical team identified smaller groups of people that had diagnoses known to frequently cooccur with ASD (e.g., Intellectual Disability) or known to be mistakenly diagnosed instead of ASD (e.g., Schizophrenia). As frontline psychology staff at the DOC’s 24 State Correctional Institutions (SCI) continue to screen through patients diagnosed with an intellectual disability, the Psychology Office leadership team recognized the need for additional community partnerships and resources beyond the DOC. The purpose of seeking to develop such partnerships was to not only enhance the DOC’s knowledge base with community expert’s insights into the identification and treatment of incarcerated people living with neurodevelopmental disorders, but also in an effort to enhance identification efforts of neurodevelopmental needs among individuals currently involved in the criminal justice system (i.e., a Pennsylvania county jail) who may eventually be transferred to DOC custody. Rather quickly, the Psychology Office established relationships with the Pennsylvania Department of Human Services’(PA DHS) Office of Developmental Programs (ODP) and the Autism Connection of Pennsylvania.
Given the novelty of this work and the identified clinical experience of staff, establishing partnerships with community neurodevelopmental advocates and experts was central to the DOC’s plan of action and subsequent clinical advancements. Under the leadership and insight of former Secretary of Corrections, John Wetzel, a new treatment unit specializing in meeting patient neurodevelopmental needs was proposed within the DOC. The development of this unit represented a unique opportunity for the DOC to lean into their collaboration with community partners even further and to include these external stakeholders into the administrative and clinical brainstorming process guiding the development of the unit. One of the more innovative contributions from the PA DHS’s ODP was to consider integrating a Positive Behavioral Support (PBS) model of care and treatment into this unit5. In response, ODP and the Psychology Office conducted numerous joint planning sessions aimed at introducing PBS to DOC psychology leadership staff, reviewing relevant PBS research, and evaluating the appropriateness of integrating elements of PBS into a correctional milieu for adults. This collaboration culminated with ODP delivering two separate but intuitive and focused PBS trainings to DOC psychology leadership staff and the clinical and administrative leadership teams at SCI-Albion. Additionally, while the development of this unit remains ongoing, the Psychology Office recognizes the importance of attempting to incorporate as many of the essential elements of PBS into the development of this unit as is safely possible, including support team involvement, assessment of contexts and functions, behavior support plan design, data-based decision making, and focus on lifestyle change. An early promising practice that the Psychology Office and ODP are exploring together for integration into this unit is the understanding of the benefits of DOC staff being proactive in identifying patients that are “doing well” and bringing this positive behavior to the attention of the neurodiverse patient, in an effort at influencing future positive behavioral outcomes within the correctional and community settings (i.e., following the person’s reentry to the community).
As the new unit continues to be collaboratively developed, the DOC is optimistic about the future of the individuals that will live in this unit, thankful for the expertise and guidance from ODP and the Autism Connection of Pennsylvania, and forever grateful and proud of the DOC staff at SCI-Albion that are responsible for the overall operations, management, and oversight of this new unit. The SCI-Albion team is the best of the best.
A final systemic
enhancement worth briefly discussing that appears to have the greatest
potential for the most change into the DOC’s ability to identify and support
individuals with neurodevelopmental needs beyond intellectual disabilities is
Pre-reception Case Identification at the county jail level. Pre-Reception
Case Identification refers to the DOC’s efforts to identify people
currently incarcerated at a Pennsylvania county jail who have known
neurodevelopmental needs and have been sentenced to serve time within the DOC.
Case identification occurs by the above-mentioned community organizations
(i.e., as a result of providing previous service and support to the family and
individual), and with the permission of the families and patients themselves,
are communicated to the attention of the DOC Psychology Office. Once identified
and shared, the Psychology Office opens the lines of communication with County
Jail Administrators and the DOC’s Office of Population Management for the
purpose of expediting transfer to DOC, if clinically indicated, or for
diverting cases away from the traditional DOC initial reception process to a
more protected, safeguarded, and clinically enhanced reception process that
affords a more individualized assessment and initial period of observation and
adjustment for the individual with known neurodevelopmental needs. These
enhancements would not be possible if not for the aforementioned relationships
forged between the DOC Psychology Office and the identified community stakeholders,
families, and organizations. These
relationships afford the DOC a much greater opportunity at retrieving valuable
patient health care records from not only community health care providers but
also from supportive family members. Pre-Reception Case Identification has
ignited the DOC Psychology Office to pursue additional transformational
enhancements aimed at supporting individuals with neurodevelopmental needs who
are preparing for transfer to the DOC. In response, the DOC Psychology Office has
dedicated centralized clinical resources to meet with patients, face to face,
who are currently housed in a Pennsylvania county jail and are awaiting
transfer to the DOC. Pre-Reception Case Identification visits afford lead
Regional LPMs in the DOC the ability to prepare a patient with known
neurodevelopmental needs for initial transfer to the DOC by answering
questions, explaining the transfer, assessment, and classification processes,
and other experiences to expect, which can be an intimidating experience for
anyone let alone an individual living with neurodevelopmental needs. Although
infrequent, this innovative practice has afforded the DOC the ability to
individually support vulnerable patients at an intercept of the criminal
justice system not previously explored for these purposes.
The DOC Psychology Office is greatly appreciative of the relationships established with ODP and the Autism Connection of Pennsylvania, as these bonds have not only facilitated the enhanced and necessary linkages to occur between existing criminal justice organizations and their clinical mental health authorities but have also greatly contributed to the DOC’s efforts of realizing continued improvement of patient access to care.
*Special thanks to
the DOC Central Office Psychology Office staff whose work and contributions are
highlighted in this article, including Dr. Cynthia Wright, Richard Goss, Dr. Brian
Schneider, Dr. Elaine Everding, James Harrington, Angel Jenrette-McDowell, and
Nicole Yesser.
References
1. American Correctional Association, On C, American. Performance-Based Expected Practices for Adult Correctional Institutions. American Correctional Association; 2018.
2. Wetzel Settlement Agreement. Disability Rights Pennsylvania.. https://www.disabilityrightspa.org/wp-content/uploads/2019/12/Web-Copy-Wetzel-Cover-Letter.pdf. Accessed April 7, 2022.
3. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. American Psychiatric Association; 2013.
4.
Allison C, Auyeung B,
Baron-Cohen S. Toward Brief “Red Flags” for Autism Screening: The Short Autism
Spectrum Quotient and the Short Quantitative Checklist in 1,000 Cases and 3,000
Controls. Journal of the American Academy of Child & Adolescent
Psychiatry. 2012;51(2):202-212.e7. doi:10.1016/j.jaac.2011.11.003.
5. Sugai G, Horner RH. Introduction to the Special Series on Positive Behavior Support in Schools. Journal of Emotional and Behavioral Disorders. 2002;10(3):130-135. doi:10.1177/10634266020100030101.
Biography
Dr. Lucas D. Malishchak has been the Director of the Psychology Office for the Pennsylvania Department of Corrections since 2017. In this role, Lucas oversees a team of four Regional Licensed Psychologist Managers, who are together responsible for the clinical oversight of the mental health care system of Pennsylvania’s 24 State Correctional Institutions, which includes an infrastructure that supports more than 35,000 incarcerated people and more than 300 mental health care professionals. Lucas’ Doctor of Business Administration degree includes a specialization in Criminal Justice. His dissertation was titled, “Alternatives to Segregation and Seriously Mentally Ill Inmates in Pennsylvania State Prisons: A Case Study of Employee Perceptions.”
Contact Information
Lucas D. Malishchak
Pennsylvania Department of Corrections
717-728-2093
Shea & Wall | 55-60
Volume 11 ► Issue 1 ► May 2022
What Comes Next? Creating Programs and Understanding Priorities for Autistic Adults as They Age
Lindsay Shea and Nina
Wall
The first prevalence of autism spectrum disorder was generated more than 50 years ago. Studies to determine how often autism occurred were conducted among children in the 1960s and the 1970s and found a range of 2 to 4 cases per 10,000 children at sites in Europe and in the US.1,2 The most recent data published by the Centers for Disease Control and Prevention (CDC) in the United States (US) identified that 1 in 44 children met criteria for an autism diagnosis in 2018.3
As the prevalence of autism has increased rapidly, research focused on autism has grown as well. Summaries of research spending have reported that almost $300 million was allocated by the National Institutes of Health (NIH) for autism research in 2019 alone. Across NIH, most funding routed through the National Institute of Mental Health (60%), the Eunice Kennedy Shriver National Institute of Child Health and Human Development (13.8%), and the National Institute of Neurological Disorders and Stroke (10.3%).4
Understanding how often autism occurs and conducting research on interventions to support individuals and families are critically important priorities. These efforts inform future programs and planning, as well as next steps for research activities. Neither, however, provide a roadmap for how to support individuals on the autism spectrum who are living and aging today.
Pennsylvania has created new models and mechanisms to work toward understanding and addressing the needs of autistic adults. The Pennsylvania Bureau of Supports for Autism and Special Populations (BSASP, formerly known as the Bureau of Autism Services) housed within the Office of Developmental Programs (ODP), Department of Human Services (DHS) was the first to put into place programs to support autistic individuals specifically focused on adults in 2008. Driven by the voice of the Pennsylvania autism community, convened through a statewide Autism Taskforce, two new Medicaid programs were launched – the Adult Autism Waiver (AAW) and the Adult Community Autism Program (ACAP). AAW and ACAP represented distinctly innovative program options for autistic adults because they were designed to address the unique and varied needs of adults on the autism spectrum, irrespective of a co-occurring Intellectual Disability (ID) diagnosis, which is a requirement of many child and adult Medicaid programs in the US. AAW and ACAP also provide a traditional, fee-for-service 1915(c) waiver (AAW) and a managed care model (ACAP), where both physical and mental or behavioral supports are coordinated. The emphasis on services to support employment, skill building, and on the integration of Applied Behavior Analysis (ABA) and Positive Behavior Supports (PBS) are nation-leading in prioritizing and deploying these service elements to an adult autistic population.
In 2017, ODP announced new eligibility criteria for waiver programs that allowed enrollment for autistic individuals who do not have intellectual disability (ID). The same programs also created a new option for enrollment if a younger child (under the age of 8) is experiencing developmental delays and is likely to be diagnosed with a developmental disability (including ID or autism). ODP supports more than 55,000 individuals, resulting in an expanded reach of these eligibility changes for autistic individuals and children with developmental delays.
Other states have sought to learn about and replicate the Pennsylvania models for adult services as innovative shifts beyond the needs of children. The work to build and sustain these programs has proved daunting as both research and practice have not kept pace. Without evidence-based information to guide providers, ODP’s BSASP has sought to build expertise from key team components, including a Clinical Team, to generate resources and supports based on their own experiences in communities, in residential facilities, and otherwise in the field. Active engagement with the Pennsylvania autism stakeholder community and monitoring of emerging research to inform training and outreach efforts has been a primary support for ongoing ODP BSASP program activities. Building and disseminating this information is a daunting task in the large geographic spread of Pennsylvania, but new methods for communicating, training, and connecting have been spurred forward by continuing need and a lack of robust evidence to inform practice on-the-ground from research. ODP’s BSASP supports the Autism Services, Education, Resources, and Training Collaborative (ASERT) in providing additional linkages to service development opportunities, informed by new projects and research. ASERT represents partnerships at 3 sites across Pennsylvania based at academic institutions and medical hospitals. ASERT generates resources, supports autistic individuals and their caregivers, and conducts programmatic initiatives.
Across the US, the
development of new waivers to serve autistic individuals is growing and states
are using other mechanisms leveraged in Pennsylvania, such as expanding
eligibility of existing programs to include autistic individuals. There have
been calls to action from the autistic adult community, including
self-advocates, and their families to ensure that there are programs available
and research underway that extend beyond early adulthood but also throughout
the lifespan. In the last round of funding, the CDC added a mechanism for
examining autism prevalence among 16-year-olds, in addition to their surveillance
work focused on 4- and 8-year-olds. A new journal, “Autism in Adulthood”, has
launched recently and has featured research that includes and is led by
autistic adults and autistic researchers to ensure their lived experience
informs the work emerging from the peer-reviewed studies that it publishes. A
recent search of the list of Medicaid waivers yields several new
autism-specific or autism-inclusive waivers in other states, including two in
Maine.
The voices of autistic individuals and their families have drawn increasing attention to the needs of the autistic community and to challenge the systems of care to prepare to meet the needs of this group as it ages. In alignment with national dialogue focused on understanding and addressing the needs of individuals from diverse racial and ethnic groups and across socioeconomic status, examining these differences among autistic individuals and their families will be key to working toward equity in access to needed care.
References
1. Lotter V. Epidemiology of autistic conditions in young children. Social Psychiatry. 1966;1(3):124-135. doi:10.1007/bf00584048.
2. Treffert DA. Epidemiology of Infantile Autism. Archives of General Psychiatry. 1970;22(5):431. doi:10.1001/archpsyc.1970.01740290047006.
3.
Shaw KA, Maenner MJ,
Bakian AV, et al. Early Identification of Autism Spectrum Disorder Among
Children Aged 4 Years — Autism and Developmental Disabilities Monitoring
Network, 11 Sites, United States, 2018. MMWR Surveillance Summaries.
2021;70(10):1-14. doi:10.15585/mmwr.ss7010a1
4. Funding for autism research, explained. Spectrum | Autism Research News. Published May 25, 2020. Accessed April 12, 2022. http://www.spectrumnews.org/news/funding-for-autism-research-explained/
Biographies
Lindsay Shea is a Senior Healthcare Analyst supporting data and policy efforts in ODP’s BSASP. She is also an Associate Professor at Drexel University, and holds a master’s degree in social policy from the University of Pennsylvania and a doctoral degree in health policy from Drexel University.
Nina Wall serves as the Director of the BSASP in the ODP, DHS. She completed her graduate studies at Bryn Mawr College's Graduate School of Social Work and Social Research and is a Licensed Social Worker. She is the parent of a young man with ASD.
Contact Information
Lindsay Shea
Office of Developmental Programs, Bureau of Supports for Autism and Special Populations
Senior Healthcare Analyst
570-850-2948
Nina Wall
Office of Developmental Programs, Bureau of Supports for Autism and Special Populations
Director
717 265-8960
Song, Salzer, Nonnemacher
& Shea | 61-68
Volume 11 ► Issue 1 ► May 2022
Reliability of the Temple University
Community Participation Measure with Adults with Autism
Wei Song, Mark S. Salzer, Stacy L. Nonnemacher, & Lindsay L. Shea
Abstract
This study examined
test-retest reliability of the Temple University Community Participation (TUCP)
measures among a group of autistic adults. The sample consisted of 17 autistic
adults from the Adult Autism Waiver (AAW) and Adult Community Autism Program
(ACAP). At 2-3 days follow-up, TUCP was completed by the same participants
again. Results revealed high test-retest reliability coefficients for the
measure. No significant differences in the participation outcomes were found
over the 2-3 days. These results suggest that TUCP is a reliable tool in the
context of community services and supports.
Background
The Pennsylvania Bureau of Supports for Autism and Special Populations (BSASP) and the Pennsylvania Autism Services, Education, Resources, and Training Collaborative (ASERT) aim to support community participation and inclusion of people on the autism spectrum across the lifespan. Due to few, if any, outcome measures available to autistic adults, BSASP and ASERT strive to identify valid measures that could advance our understanding of autistic individuals’ participation experience. This is essential considering existing evidence showing that participation in community-based activities, including social and recreational activities of autistic people, is associated with lower levels of depression and stress 1 and improved quality of life. 2,3
The Temple University Community Participation (TUCP) measure 4 captures individuals’ participation experiences and preferences across a wide range of community activities. It was first designed for adults with serious mental illnesses. Among adults with psychiatric disabilities, the TUCP has shown robust test-retest reliability 4 and achieved good inter-method reliability by showing consistent results with those obtained using the diary checklist approach.5
Research
has consistently demonstrated that autistic adults participate less and in
fewer areas that are meaningful to them compared to adults in the general
population and adults with other disabilities 1,6,7. A previous study also reported a significant decrease
of social and community participation in transition from adolescence to
adulthood 8. However, the
measures of community participation and the categories of activities
encompassed in the different types of participation are poorly defined in the
ASD literature. Many studies either used national surveys7 or author-constructed measures.1 The TUCP captures a full range of
participation in multiple areas, including employment, education, leisure,
faith, and interactions with friends and family. It also goes beyond measuring
the quantitative scales of participation (i.e., frequency and diversity) and
provides information about individual preferences and sufficiency of
participation.
The existing reliability (or how consistently something is measured) of the TUCP established for people with mental illness gives practitioners and service providers some confidence that the TUCP scores represent useful information about community participation. Nonetheless, it is vital to assess the reliability of the TUCP among autistic people. The main aim of this project is to support the BSASP clinical and quality improvement efforts as they consider possible assessment tools for use with autistic adults they serve. Specifically, this study examined the utility of the TUCP by assessing its test-retest reliability (i.e., the consistency of individual responses) among autistic adults in the Pennsylvania service system.
What
Is TUCP
The TUCP measure assesses independent participation (without the support of staff) in a wide range of areas. For each item, the respondent is asked the number of days they participated in an activity in the last 30 days, the importance of an activity, and whether they did the activity enough. Based on the responses, the following participation outcomes were generated, which were used to test test-retest reliability:
1. Participation days = the total number of days of participation across the 24 activities.
2. Breadth ratio= the ratio of the
number of important activities with at least one day of participation by the
number of important activities.
3. Sufficiency ratio= the ratio of the number of important activities in which participants indicated doing enough by the number of important activities
Data Collection Method
In
collaboration with the Bureau of Supports for Autism and Special Populations
(BSASP), participants from the AAW and ACAP were asked to complete the TUCP.
All autistic individuals had a formal autism spectrum disorder (ASD) diagnosis.
Support Coordinators (SCs) identified individuals who were able to self-report
or complete the TUCP for themselves. A total of 21 autistic adults completed
the TUCP and completed TUCP information for 17 individuals was included.
Completed TUCPs were collected between March to May 2021 using Qualtrics, a web-based survey software that allows the user to create surveys and generate reports. Links to Qualtrics surveys were sent to SCs. SCs explained how to complete the TUCP to the individuals and determined whether assistance was needed to complete the measure. An interview script was created for the SCs to facilitate their conversations with participants. Based on the levels of support individuals needed, the TUCP was completed independently, with SC assistance (e.g., read aloud, recording answers), or were interviewed by SCs. After the first administration, individuals were asked to complete the TUCP and again within 2-3 days of the first TUCP being completed. The methods of completion (independently or via interview) had to be consistent across the two administrations. Among the 17 individuals with completed TUCPs, seven (41%) completed the survey by themselves, six (35%) completed with help, and 4 (24%) were interviewed by SCs.
Main Findings
The average age was 33.5 years (SD=7.9). All individuals had at least a high school degree. About 77% (n=13) had an annual income of less than $10,000.
For the results of test-retest reliability:
· Participation days: Pearson correlations between Time 1 and 2 was 0.90 (p<0.01). The total number of participation days were similar across the two administrations (p>0.05). The high correlation between the two timepoints indicated great consistency in reporting participation days.
· Breadth ratio: Pearson correlations between
Time 1 and 2 was 0.88 (p<0.01). The percentages of participating in
important activities were not significantly different across the two
administrations (p>0.05). This indicated that the test–retest reliability
for breadth ration was excellent.
· Sufficiency ratio:
Pearson correlations between Time 1 and 2 was 0.79 (p<0.01). The levels of sufficiency were not significantly different across the
two administrations (p>0.05). As the other two outcomes, the high
correlation indicated good test-retest reliability for sufficiency ratio.
Conclusion and Potential Use
The results from this effort suggest that the TUCP has good-to-excellent test-retest reliability. Thus, the TUCP can be used to reliably measure the community participation of adults on the autism spectrum in BSASP programs. This combined with findings related to the validity of the measure 9,10, supports its potential use in a range of community-based settings and provides a tool for planning and providing supports and services as well as provide insights into service quality and personal outcomes across service programs.
Acknowledgment
This project was fully supported by the Autism Services, Education,
Resources, & Training Collaborative (ASERT), Bureau of Supports for Autism
and Special Populations (BSASP).
References
1. Stacey T-L, Froude EH, Trollor J, Foley K-R. Leisure participation and satisfaction in autistic adults and neurotypical adults. Autism. 2019/05/01 2019;23(4):993-1004. doi:10.1177/1362361318791275.
2. Billstedt E, Gillberg I, Gillberg C. Aspects of quality of life in adults diagnosed with autism in childhood. Autism. 2011;15(1):7-20. doi:10.1177/1362361309346066.
3. Bishop-Fitzpatrick L, Smith DaWalt L, Greenberg JS, Mailick MR. Participation in recreational activities buffers the impact of perceived stress on quality of life in adults with autism spectrum disorder. https://doi.org/10.1002/aur.1753. Autism Research. 2017/05/01 2017;10(5):973-982. doi:https://doi.org/10.1002/aur.1753.
4. Salzer MS, Brusilovskiy E, Prvu-Bettger J, Kottsieper P. Measuring community participation of adults with psychiatric disabilities: Reliability of two modes of data collection. Rehabilitation psychology. 2014;59(2):211-219. doi:10.1037/a0036002.
5. Salzer MS, Kottsieper P, Brusilovskiy E. Intermethod reliability and factors affecting recall with the Temple University Community Participation measure. Journal of Mental Health. 2015/07/04 2015;24(4):189-195. doi:10.3109/09638237.2015.1036976.
6. Song W, Shea L, Nonnemacher S, Brusilovskiy E, Townley G, Salzer M. Community Participation Comparison Between Adults on the Autism Spectrum and Adults in the General Population. Journal of Autism and Developmental Disorders. 2021;52, 1610–1621. doi:10.1007/s10803-021-05059-9.
7. Orsmond GI, Shattuck PT, Cooper BP, Sterzing PR, Anderson KA. Social Participation Among Young Adults with an Autism Spectrum Disorder. Journal of Autism and Developmental Disorders. 2013/11/01 2013;43(11):2710-2719. doi:10.1007/s10803-013-1833-8.
8. Myers E, Davis BE, Stobbe G, Bjornson K. Community and Social Participation Among Individuals with Autism Spectrum Disorder Transitioning to Adulthood. Journal of Autism and Developmental Disorders. 2015;45(8):2373-2381. doi:10.1007/s10803-015-2403-z.
9.
Shea
LL, Verstreate K, Nonnemacher S, Song W, Salzer MS. Self-reported community
participation experiences and preferences of autistic adults. Autism. 2021;25(5):1295-1306. doi:10.1177/1362361320987682.
10. Song W, Salzer MS, Nonnemacher SL, Shea LL. Community participation patterns among autistic adults and associated characteristics: A latent class analysis. Research in Autism Spectrum Disorders. 2021;89:101884. doi:https://doi.org/10.1016/j.rasd.2021.101884.
Biographies
Dr. Wei Song is a postdoctoral fellow in the College of Public Health at Temple University and works with the Temple University Collaborative on Community Inclusion to examine community participation among adults on the autism spectrum. She received funding from the Eagles Autism Challenge Fellowship to conduct this research.
Mark Salzer, Ph.D. is a psychologist and Professor of Social and Behavioral Sciences in the College of Public Health at Temple University. He is also the Principal Investigator and Director of the Temple University Collaborative on Community Inclusion of Individuals with Psychiatric Disabilities, a rehabilitation research and training center funded by the National Institute on Disability, Independent Living, and Rehabilitation Research since 2003. Dr. Salzer’s research focuses on community inclusion and participation.
Stacy L. Nonnemacher received her Ph.D. from Lehigh University. She is currently the Clinical Director for the Bureau of Supports for Autism and Special Populations in the Office of Developmental Programs in Pennsylvania's Department of Human Services. Stacy is the Editor in Chief of the Positive Approaches Journal. She has been involved in the field of disabilities for over twenty-five years supporting children, adolescents, and adults in home, community, and school settings. Dr. Nonnemacher has conducted applied research and training on Positive Behavioral Support, fostering self-determination, Functional Behavioral Assessment, and the needs of and support for individuals with autism.
Lindsay Shea is a Senior Healthcare Analyst supporting data and policy efforts in ODP’s BSASP. She is also an Associate Professor at Drexel University, and holds a master’s degree in social policy from the University of Pennsylvania and a doctoral degree in health policy from Drexel University.
Contact Information
Dr. Wei Song
College of Public Health, Temple University
Post-doc Fellow
wei.song0001@temple.edu
Mark Salzer:
570-850-2948
Stacy Nonnemacher
Office of Developmental Programs, Bureau of Supports for Autism and Special Populations
Clinical Director
Lindsay Shea
Office of Developmental Programs, Bureau of Supports for Autism and Special Populations
Senior Healthcare Analyst