Positive Approaches Journal, Volume 11, Issue 2
| Site: | My ODP |
| Course: | My ODP |
| Book: | Positive Approaches Journal, Volume 11, Issue 2 |
| Printed by: | |
| Date: | Wednesday, August 5, 2026, 8:45 PM |
Positive Approaches Journal | 6-8

Volume 11 ► Issue 2 ► August 2022
A Better Understanding of Mental Health to Improve Systems and Supports
Introduction
This issue seeks to shed light on and provide context to better understand the needs, experiences, and emerging treatment and support of people with mental health challenges including those with intellectual and developmental disabilities. We would like to specifically highlight the 988 Suicide and Crisis Lifeline. In 2020, Congress designated the new 988 dialing code to be operated through the existing National Suicide Prevention Lifeline. This option is the first step towards a transformed crisis care system in America. Pennsylvania’s 988 is live as of July 16, 2022, and should be considered a source of support for people in emotional distress or suicidal crisis.
Wolf Administration Marks National Launch of 988
Harrisburg, PA – Department of Human Services (DHS) Acting Secretary Meg Snead, Department of Health Acting Secretary Dr. Denise Johnson, and Representative Mike Schlossberg joined together today to highlight the national launch of the 988 Suicide and Crisis Lifeline that officially went live on July 16.
People who call, text, or chat with 988 are now directly connected to the same trained, compassionate crisis response counselors that were accessible through the 10-digit National Suicide Prevention Lifeline, now rebranded as the 988 Suicide & Crisis Lifeline.
“Pennsylvanians now have a new, easier way to connect to behavioral or mental health crisis services – a historic step to increase access to life-saving support when people need it most,” said DHS Acting Secretary Snead. “988 can be used by anyone, any time, at no cost, no matter what you are experiencing. Your life matters, so please know that this service is always here to help provide the support that you or your loved ones deserve.”
“As an OB-GYN physician, I’ve spent my career caring for people, especially during vulnerable times of their lives like the pregnancy and post-partum periods. Providing mental and emotional health assistance is just as important as taking care of a person’s physical health. I have seen firsthand how individuals and families can benefit when they receive help to address their mental and behavioral health needs. The new 988 number will help make that much easier to reach for any Pennsylvanian who is in crisis or who needs help for a loved one,” said DOH Acting Secretary Johnson.
In 2020, the United States Congress designated the new 988 dialing code to connected callers and texters to Lifeline call centers. Pennsylvania has 13 crisis call centers that collectively serve the entire state. With the national launch of 988, these call centers will continue to provide support for individuals considering suicide, self-harm, or any behavioral or mental health need crisis. While the majority of calls are triaged and de-escalated without deploying in-person services, in communities where mobile crisis mental health teams are available, the 988 counselor can dispatch the team to provide on-site support and interventions. They are also able to call out police or other emergency services if there is an immediate risk to life or safety. Callers to 988 can also connect with the Veterans Crisis Line or assistance in Spanish.
Lifeline services are
available 24 hours a day, seven days a week at no cost to the caller. To chat,
go to https://988lifeline.org/chat/.
While the intent of 988 is to ease access to and knowledge of life-saving
mental health crisis resources, the existing Lifeline phone number (1-800-273-8255)
will remain available, as well as 911 in the event the individual is experiencing
a life-threatening emergency.
To learn more visit, www.dhs.pa.gov.988
Stacy L. Nonnemacher, Ph.D. Editor-in-Chief
Clinical
Director
Office of Developmental Programs
Positive Approaches Journal | 9-14
Volume 11 ► Issue 2 ► August 2022
Data Discoveries
The goal of Data Discoveries is to present useful data using new methods and platforms that can be customized.
Research has identified high rates of co-occurring mental health diagnoses, like depression, anxiety, and obsessive-compulsive disorder (OCD), among individuals on the autism spectrum1 and individuals with intellectual disabilities (ID). 2 However, rates of how frequently mental health diagnoses occur in these populations often vary by study. Some studies show rates of co-occurring mental health as high as 79%3 in autism spectrum disorder (ASD) populations and some as low as 23.1%.4 Some studies show rates of co-occurring mental health conditions in ID populations as high as 67.2% (Bishop-Fitzpatrick, et al., 2019) in and some as low as 12.5%.4 The most common co-occurring diagnosis among the autistic population documented within this research base is attention-deficit/hyperactivity disorder (ADHD)5, which decreased with age6 and specific phobias among the ID populations.7 The presence of a psychiatric co-occurring diagnoses can have a host of impacts on individuals on the spectrum and individuals with ID and their families. Without intervention and treatment, mental health diagnoses can impact a range of life experiences, including employment and quality of life and can result in negative and unwanted outcomes like hospitalization and police contact.8,9 Ensuring awareness of and support for services for identifying and treating mental health diagnoses can prevent these outcomes or lessen their impact.8
In Pennsylvania, the Autism Services, Education, Resources, & Training Collaborative (ASERT) conducted the 2018
Pennsylvania Autism Needs Assessment (2018 PANA). More than 8,000 autistic individuals and their caregivers completed the 2018 PANA, providing information about demographic, clinical characteristics, and other service experiences. In this sample,
we found that 84% of autistic adults and caregivers of autistic individuals of all ages reported at least one mental health diagnosis. The most commonly reported mental health diagnosis in the entire sample was attention-deficit/hyperactivity disorder
(51%). In adults over age 18, both self-reported and caregiver-reported, anxiety disorder was the most commonly-reported mental health diagnosis (50%). In children under age 18 in the caregiver-reported 2018 PANA attention-deficit/hyperactivity disorder
was the most commonly reported mental health diagnosis (57%). For more information about the 2018 PANA and to view more data, visit: www.paautism.org/needsassessment.
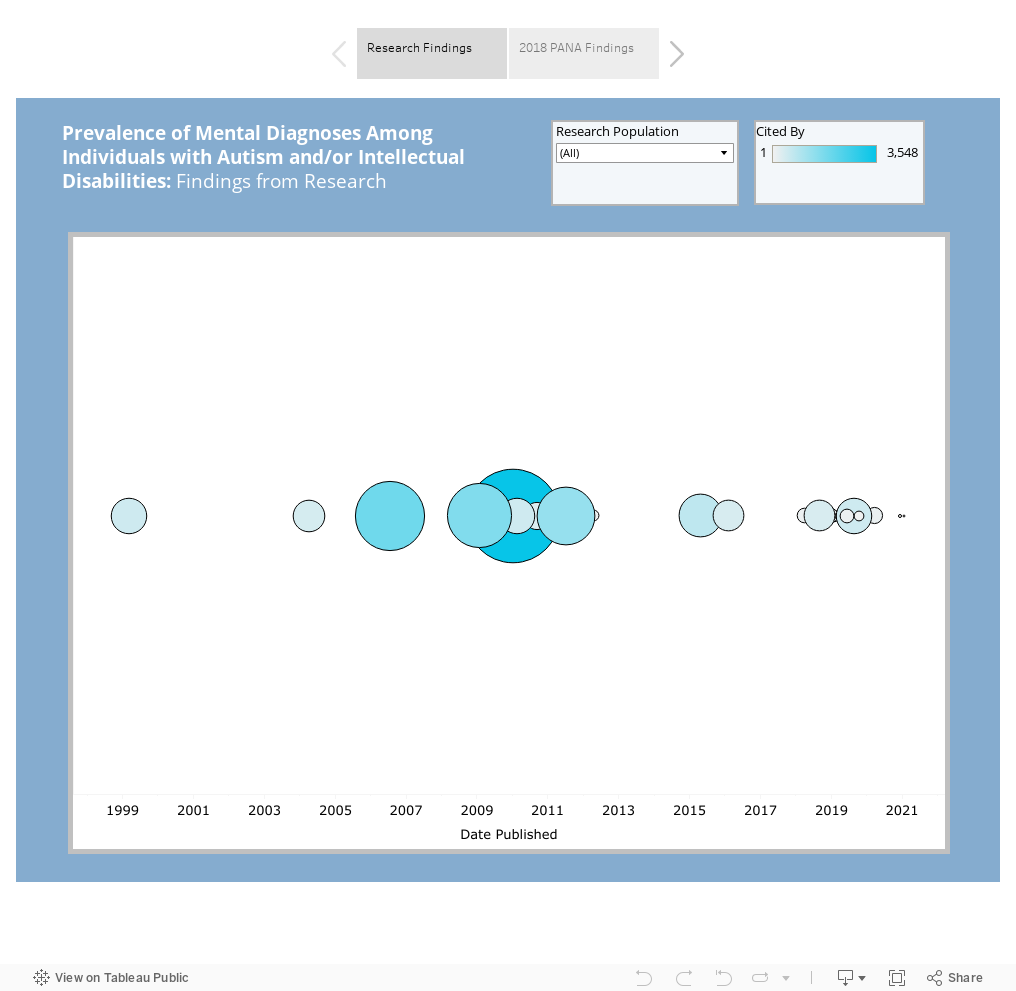
The data dashboard below shows information on the prevalence of mental health conditions among the ID and ASD populations from peer reviewed research studies. The visual displayed on the first tab of the dashboard shows a timeline of publications from all peer-reviewed research focused on identifying mental health diagnosis occurrence among autistic individuals and individuals with ID. Each circle represents a publication, with the size and color indicating how often the article was cited by other research, which is an indicator of the impact or reach of that publication. To read the text, click on a circle to be directed to the abstract for each article and potential access options. The second tab shows the frequency of mental health condition co-occurrences among the respondents to the 2018 PANA. Together, these visuals demonstrate how research outside of Pennsylvania and among autistic Pennsylvanians has pointed toward understanding co-occurring diagnoses and supports how progress toward services for mental health diagnoses need to be accessed and delivered.
Conclusion
The ASERT Collaborative is home to an extensive library of resources focused on the intersection of autism, intellectual disability, and mental health. The Mental Health Resource Collection (www.paautism.org/MentalHealth) is a bundle of resources focused on varying aspects of mental health including psychopharmacology, crisis intervention, and behavior. The Be Well, Think Well Resource Collection ( www.paautism.org/BeWell) includes information for self-advocates, providers, and family members to help people understand the mental health challenges experienced by individuals on the autism spectrum. The Support Professional Resource Collection (www.paautism.org/DSP) has resources on a myriad of topics for direct support professionals working with individuals on the autism spectrum including mental health diagnoses.
References
1. Rast JE, Garfield T, Roux AM, et al. National Autism Indicators Report: Mental Health. 2021. https://drexel.edu/autismoutcomes/publications-and-reports/publications/NAIR-mentalhealth/
2. Crocker AG, Prokić A, Morin D, Reyes A. Intellectual disability and co-occurring mental health and physical disorders in aggressive behaviour. Journal of intellectual disability research. 2014;58(11):1032-1044. doi:10.1111/jir.12080
3. Lever AG, Geurts HM. Psychiatric Co-occurring Symptoms and Disorders in Young, Middle-Aged, and Older Adults with Autism Spectrum Disorder. J Autism Dev Disord. 06 2016;46(6):1916-30. doi:10.1007/s10803-016-2722-8
4. Nimmo-Smith V, Heuvelman H, Dalman C, et al. Anxiety Disorders in Adults with Autism Spectrum Disorder: A Population-Based Study. Journal of Autism and Developmental Disorders. 2019;50(1):308-318. doi:10.1007/s10803-019-04234-3
5. Lugo-Marín J, Magán-Maganto M, Rivero-Santana A, et al. Prevalence of psychiatric disorders in adults with autism spectrum disorder: A systematic review and meta-analysis. Research in autism spectrum disorders. 2019;59:22-33. doi:10.1016/j.rasd.2018.12.004
6. Fombonne E, Green Snyder L, Daniels A, Feliciano P, Chung W. Psychiatric and Medical Profiles of Autistic Adults in the SPARK Cohort. Journal of autism and developmental disorders. 2020;50(10):3679-3698. doi:10.1007/s10803-020-04414-6
7. Platt JM, Keyes KM, McLaughlin KA, Kaufman AS. Intellectual disability and mental disorders in a US population representative sample of adolescents. Psychological medicine. 2019;49(6):952-961. doi:10.1017/S0033291718001605
8.
Maddox BB, Gaus VL. Community Mental Health Services for Autistic Adults: Good News and Bad News. Autism in adulthood. 2019;1(1):15-19. doi:10.1089/aut.2018.0006
9. Turcotte P, Shea LL, Mandell D. School discipline, hospitalization, and police contact overlap among individuals with autism spectrum disorder. Journal of Autism and Developmental Disorders. Mar 2018;48(3):883-891. doi:10.1007/s10803-017-3359-y
Basci, Schwartz, Moffatt | 15-22
Volume 11 ► Issue 2 ► August 2022
The Intersection of
Mental Health First Aid and Intellectual and Developmental Disabilities
Lisa Basci, MA, LPC, Peg Schwartz, MSW, LCSW, and
Elspeth Moffatt, MBA
In a society that equips its community members at
all ages to recognize and respond to a variety of emergency situations, it is
becoming increasingly clear that we need to include education about mental
health emergencies as part of our standard practices and curriculum. Most of us
learn the basics of stop, drop, and roll and performing the Heimlich maneuver,
and we all likely know at least a handful of people certified in CPR first aid
who can recognize the signs and symptoms of a cardiac event. But how many
individuals do you know who can both recognize a mental health crisis and know
the basic mental health first aid response to support someone until help
arrives? That is the critical role that mental health first aid (MHFA) plays in
community education for all.
Like CPR first aid, any person can become certified in MHFA through participation in a one- to two-day course that equips a trainee with the basic first aid knowledge needed to recognize when someone is in crisis or needs immediate professional help. MHFA-certified individuals understand how to support that individual in life sustaining ways until that help arrives. MHFA is a standardized, evidence-based course that gives the learner an opportunity to acquire knowledge through virtual, in person, or hybrid learning situations. MHFA offers various curriculum including adult, youth, teen, higher education, fire and EMS, law enforcement, corrections and public safety, veterans, service members and their families, at work, older adults, and rural communities. Attendees who have completed the course become fully certified for three years and receive a comprehensive MHFA manual as an educational reference tool and resource guide and are then eligible to renew their certification through the National Council for Mental Wellbeing.
Mental Health First Aid was created in Australia in 2001 by Betty Kitchener, a nurse specializing in health education, and Anthony Jorm, a mental health literacy professor. The intent was to find ways to help someone who is experiencing a mental health challenge or mental health crisis. The idea of assisting people before a challenge becomes a crisis was paramount to the training. MHFA is administered by the National Council for Mental Wellbeing and delivered through discussion topics, exercises, videos, and a variety of activities designed to keep learners attentive and actively engaged in the course. The curriculum covers common signs and symptoms of mental health challenges, common signs and symptoms of substance use challenges, how to interact with a person in crisis, how to connect a person with help and has expanded content on trauma, substance use, and self-care. Providing people with skills to be more confident in recognizing changes, intervening early, and how to approach someone in need, make up the philosophical underpinnings of the course.
Historically, mental health and intellectual and developmental disabilities (IDD) have often been thought to be mutually exclusive. Professionals have been taught through the academic process and, to some extent, through the delivery of services that individuals must receive services in either one area or the other and one must be of primary interest. Most recently, it has become more apparent that this line of service delivery has left some individuals without the support that is necessary to enjoy an everyday life. Furthermore, since many individuals with MH/IDD often rely on their supporters to share and describe pertinent mental health information with their prescribers, it is crucial that supporters receive training and education in mental health and remember that symptoms of mental illness may lurk behind what seems like challenging behavior.
Individuals with IDD can experience the same mental disorders as the general population, as well as some disorders that are uncommon in the general population. Studies have indicated that psychiatric disorders in people with IDD are at a higher rate than in the neurotypical population 1. Although the exact prevalence of individuals with IDD who also have a mental illness is debated among researchers, estimates range from 14-70%. The National Association for the Dually Diagnosed, NADD, estimates that the prevalence is somewhere between 30 and 40% 2. Although we know the rate of diagnosed mental illness in IDD is higher than in the typical population, in 2021 in Pennsylvania alone 18.23% or 1,814,000 typical adult citizens have a mental illness diagnosis of some kind 3. What is without debate is the impact that a mental illness has on an individual with IDD. How a mental illness manifests in an individual with IDD can often be underappreciated and viewed as an expression of challenging behavior. Community members and direct service providers may struggle to identify what actions and behaviors stem from limits of the person’s functional capacity and what may result from an underlying mental illness. MHFA attendees are better prepared to identify mental health signs and symptoms which is crucial not only in supporting a dually diagnosed individual but also ensuring that accurate symptom information can be shared with the psychiatrist versus reporting challenging behavior.
Becoming
certified in MHFA is a benefit that reaches far beyond supporting the IDD
individual in services. MHFA teaches the learner how issues like stigma,
bias, lack of resources, lack of knowledge, and even not knowing what to say,
can all be significant barriers to wellness not only for the IDD individual but
to everyone that surrounds that person in their life. Mental illness does not
only affect the people we support, it can affect any of us at any point in time
in our lives.
This is where a
certification in MHFA can help. MHFA is a tool we can use to view any
individual with an additional lens, expand our helping skills and engage from a
place of confidence. The curriculum delivers instruction on topics including
anxiety, depression, trauma, psychosis, substance use, how to recognize changes
in mental health, and what steps to take to help. It does not replace any
current tool or knowledge, it enhances the supporter’s personal toolkit and
opens the door to encourage even further skill and knowledge building. MHFA
presents a platform to learn how mental illness symptoms manifest and provides
a concrete action plan that can be used by any person, with any person, in any
environment, at any time, to guide a situation to a safer resolution and become
the warm handoff for formal mental health treatment when
needed.
The
collaborative efforts of Pennsylvania’s Office of Mental Health and Substance
Abuse Services (OMHSAS) and the Office of Developmental Programs (ODP) through
the Money Follows the Person grant allowed the MHFA training to be delivered
throughout much of Pennsylvania. OMHSAS and ODP reached out to Community
Services Group (CSG) for MHFA training support, as CSG has an established group
of master’s level trainers dating back to the inception of MHFA in the US over
13 years ago. MHFA instructors have taught the skill-based curriculum in a
variety of locations such as state centers, state hospitals, community mental
health settings, community and state ID/D settings, county government offices,
support coordination organizations, provider agencies, and the community at
large.
As the MHFA curriculum continues to evolve and address the changing needs of our communities across the United States, what remains steadfast is MHFA’s commitment to providing people with an opportunity to learn how to help someone who is developing a mental health problem or experiencing a mental health crisis. Learners develop a set of skills to Assess for the risk of suicide or harm, Listen non-judgmentally, Give Reassurance and Information, Encourage Appropriate Professional help and Encourage Self Help and other support strategies (A.L.G.E.E.). Across the United States, MHFA training has reached more than 2.5 million people. Globally, over four million people have been trained, and over 25 countries have adopted MHFA. Perhaps you can be certified too.
References
1. Fletcher,R., Barnhill, J., Cooper, S. Diagnostic Manual - Intellectual Disability 2, Kingston NY.
2. Bradley, V.
People with I/DD Who are Dual Diagnosed with Mental Illness: Characteristics
and Outcomes. https://www.google.com/url?q=https://www.nationalcoreindicators.org/upload/presentation/NCI_slides_Dual_Diagnosis_webinar_final.pdf&sa
=D&source=docs&ust=1656522842487880&usg=AOvVaw1XPbyKb6_Y1LkMFHuvxRO3 Accessed June
6, 2022.
3. Mental Health America Website https://www.mhanational.org/issues/2021/mental-health-america-prevalence-data#one.
Biographies
Lisa Basci is a Licensed Professional Counselor with over 35 years working in Mental Health. She has worked in partial hospitalization, residential settings for both mental health and intellectual developmental disabilities, and crisis management. She has worked with adolescents, adults, and geriatric populations. She is a nationally certified instructor in Adult, Youth and teen Mental Health First Aid through National Council for Mental Wellbeing She has been recognized as a top 100 instructor nationally. She has been part of the first national training for Youth and part of the national pilot for teen mental health first aid. She has been instructor since 2009. She is also an adjunct faculty member at a local community college teaching, General, Developmental, and Abnormal Psychology.
Elspeth Moffatt, MBA is the Communications Director for Community Services Group in Lancaster, Pennsylvania, where she has worked since 2007. She earned her Bachelor of Science in Psychology from Virginia Commonwealth University in Richmond, Virginia and a Master of Business Administration from the Kellogg School of Management at Northwestern University. Elspeth currently lives in Lancaster with her two daughters. She recently completed a term as Board Chair for the Arc of Lancaster Lebanon and now serves on their Development Committee. She is also a member of the WITF Community Advisory Board and volunteers with Junior Achievement.
Peg Schwartz, MSW, LCSW is a Licensed Clinical Social Worker and the Director of Behavior Services for Community Services Group, Inc. She has been working with people with MH/IDD for over 27 years and has expertise in supporting individuals and families throughout the lifespan who are challenged by complex mental health disorders, fetal alcohol syndrome, autism, trauma, and significant behavioral challenges. She is a nationally certified Adult and Youth Mental Health First Aid Instructor and a Scientific Advisor for Advanced Metrics. She has spoken at local, state, national, and international conferences on topics including psychiatric and behavioral challenges, integrated care, and positive behavioral supports. She received her Master of Social Work from Marywood University.
Contact Information
Lisa Basci, MA, LPC
Community Services Group, Inc.
Director of Peer Support and Mental Health First Aid
570-931-4095
Elspeth Moffatt, MBA
Communications Director
Community Services Group
717-794-6097
Peg Schwartz, MSW, LCSW
Director of Behavioral Services
Community Services Group, Inc.
610-866-7600 ext 4001
Bulkoski | 23-36
Volume 11 ► Issue 2 ► August 2022
Pennsylvania Office of Developmental Programs, Office
of Mental Health and Substance Abuse Services, and Allegheny Department of
Human Services START Pilot Partnership
Brenda Bulkoski
Pennsylvania’s human services have long struggled with the challenges associated with the needs of individuals with intellectual disability and/or autism (ID/A) and acute behavioral health (BH) issues. In response to that need, the Systemic, Therapeutic, Assessment, Resources, and Treatment Model (START) is being explored as a viable option to address the complexities of this population. Pennsylvania’s Department of Human Services on Dual Diagnosis received expert feedback that identified there needed to be network development for diversionary services and crisis response to optimize the coordinated planned crisis response and diversion strategies from state facilities. It was suggested that implementation of model programs such as START would optimize proactive crisis prevention strategies and coordinated crisis response through the expansion of these services and activities.
START is:
- Treatment-focused and specifically designed to serve those with
intellectual disability and/or autism and behavioral health needs.
- Person-centered, trauma-informed, and evidence-informed,
recognizing that this particular population has suffered various levels of
trauma in the form of multiple hospitalizations, medication changes, and
residential placements.
- Emphasizes the central importance of building linkages. START begins with the focus on the persons existing supports/resources. Then in partnership with those supports/resources, the person begins identifying strategies all team members will utilize in an integrated approach. 1
START is not a habilitative service, rather, it is a treatment service and a behavioral health response to better serve individuals with ID/A and behavioral health challenges. The START model is designed for anyone ages six and up with ID/A and Behavioral Health issues. The model is flexible and can be stylized for many different sub-populations within these parameters.
At an operational level,
START uses a Tiered or Tertiary Approach.2
- The Primary Intervention level focuses on outreach and
relationship building, training/education, partnerships and linkages, building
capacity of skill and competency. This is the least restrictive level of
intervention and can meet the needs of the most individuals.
- The Secondary Intervention level is prevention focused.
This involves more resources and increased focus on planning strategies for
individuals when supporting and serving them.
- The Tertiary level is that of direct crisis response,
intervention, and stabilization. There is always a debrief with the serving
team following any significant crisis event.
What we hope to accomplish
In the spring of 2021, Pennsylvania’s Office of Developmental Programs (ODP) along with the Office of Mental Health and Substance Abuse (OMHSAS) approached Allegheny County Office of Developmental Supports (ODS) and Office of Behavioral Health (OBH), asking if Allegheny County Department of Human Services would be interested in partnering on piloting the implementation of the START model. This pilot will last three years. This approach is very appealing to Allegheny. The opportunity to invest the time in building capacity through education and partnerships is very exciting. The results associated with responding to the need versus reacting to a situation will be a true cultural shift, yet one that is vital. Allegheny County DHS has made a commitment to provide services that are accessible, culturally competent, integrated, and comprehensive. To assure that all perspectives are considered, Allegheny County wants to have a diverse group of individuals. Through exploration of the START model, Allegheny County aims to learn better ways to address service and support needs for those individuals with the most complex ID/A and behavioral health conditions. One way to accomplish this is by providing the opportunity – as well as have the expectation – that those systems work together to identify gaps and needs and then collaborate and plan to address the needs of those more effectively. One of the goals of this pilot is to strengthen our current provider network by building competency and confidence and capability in serving persons with ID/A and BH needs. By assisting providers in meeting the needs of these complex individuals, results should indicate an increase in the stability of the persons current life and reduce the frequency of discharges and placement in restrictive settings. Furthermore, there should be evidence of less unnecessary contact with hospital emergency rooms or encounters with law enforcement. By contrast, when such encounters cannot or should not be avoided, the outcome to better support the person’s needs and reduce the likelihood of additional encounters. It’s important to acknowledge the current struggle providers have in recruiting and retaining staff. Allegheny County hopes to see a connection between staff who are trained, supported, and encouraged, and a more stable workforce. One final goal to have the ability to offer enhanced support to families who live with and support individuals with complex issues. Part of the START model aims to equip our families with resources so their experiences with their loved ones are more enjoyable and they are more confident in knowing where to go, what to do, and who to call for help when needs arise. According to the University of New Hampshire Center for START Services Annual Report 2021, the START approach has seen some positive outcomes. Of the crisis calls received in 2021, 85% of those calls resulted in the person remaining in their community setting and an additional 9% returning home following a brief emergency department visit. Seventy-one percent of individuals had a reduction in mental health symptoms as measured by the ABC.
Currently in Allegheny County
As of May 2022, in Allegheny County, there are 6,238 individuals active with the Office of Developmental Supports (ODS). 244 of them (or 4%) are also active in our Office of Behavioral Health (OBH).
Figure 1: Age breakdown of those active in Allegheny DHS, ODS and OBH
|
Age |
Number of Individuals |
% of total (N=244) |
|
21 and younger |
102 |
42% |
|
22 and older |
142 |
58% |
Figure 2: Gender breakdown of those active in Allegheny DHS, ODS and OBH
|
Gender |
Number of Individuals |
|
Male |
147 |
|
Female |
97 |
Data from the Allegheny County ODS for FY 21/22
These individuals are well known to both the intellectual disability/autism and behavioral health systems. Many of them experience a pattern of rotating hospital stays and multiple residential placements. In addition, these individuals experience trauma related to inconsistent staff who are not familiar with their personal history. For years, the systems responsible for meeting the needs of those with intellectual disability (ID), developmental disabilities, autism, and behavioral health needs have recognized support gaps and uncoordinated care. Some of the challenges for the service delivery system have rested in regulatory and statutory rulings and uncoordinated funding. In addition, professionals serving from each of these systems have often reported feeling ill-equipped to serve the more comprehensive needs of persons they were supporting, which resulted in a reliance toward the ‘other system’ to serve the more ‘primary’ need. Though many dedicated professionals have tried to bridge this gap through collaboration, something was still missing.
Allegheny DHS Target Groups
Allegheny County has identified a target group who could best benefit from this model. This cohort includes individuals between the ages of 12 – 35 with either ID or autism and significant behavioral health needs. This age range has experienced some of the longest hospital stays, highest cost of services, and highest turnover in residential placements.
For the initial phase of the pilot, 70 individuals have been targeted as “first referrals” to START.
For the most recent FY (21/22), key elements related to this grouping included whether or not individuals are receiving services and funding (Figure 4).
Figure 3: Race and Gender breakdown for 70 “First Referrals”
|
Race |
Gender |
|
|
42 Black |
24 Male |
18 Female |
|
22 White |
17 Males |
5 Females |
|
2 other |
|
2 Females |
|
1 Asian |
|
1 Female |
|
1 Hispanic |
1 Male |
|
Data from the Allegheny County ODS for FY 21/22
Figure 4: Funding of 70: “First Referrals”
|
Total Unique Individuals Identified |
70 |
% of total |
|
Individuals with ODS Funding |
34 |
48.6% |
|
Individuals without ODS Funding |
36 |
51.4% |
|
Individuals with OBH Funding |
59 |
84.3% |
|
Individuals without OBH Funding |
11 |
15.7% |
|
Individuals with either ODS/OBH Funding |
62 |
88.6% |
|
Individuals with No Funding |
8 |
11.4% |
Data from the Allegheny County ODS for FY 21/22
Figures 5 and 6 highlight
the top 5 services received through each office. The following considerations
should be noted when looking at this data:
- The authorization amounts reflect duplicative individual counts
considering individuals cross different services and can receive multiple
service combinations simultaneously as needed.
- The utilization amounts and authorization averages may appear lower than expected due to individuals not being placed for a full year, interrupted placements, discharges, and/or COVID.
Figure 5: Top 5 most frequently authorized services from Office of Developmental Supports
|
ODS Service Subgroup |
Auths |
Amt Utilized |
Amt Auth |
Auth Amt Avg |
|
Res Hab - Licensed |
62 |
$3,262,305 |
$4,857,653 |
$78,349 |
|
In-Home & Community Supports |
36 |
$374,876 |
$627,065 |
$17,418 |
|
INELIGIBLE Costs |
41 |
$260,136 |
$372,104 |
$9,076 |
|
Supplemental Habilitation |
10 |
$144,448 |
$229,924 |
$22,992 |
|
SUPPORTS COORDINATION Services |
64 |
$133,187 |
$227,644 |
$3,557 |
Figure 6: Top 5 most frequently authorized services from Office of Behavioral Health
|
OBH Cost Center |
Total Cost |
|
Psychiatric Inpatient Hospital |
$1,443,872 |
|
Community Residential Services |
$802,555 |
|
Outpatient |
$345,978 |
|
Not yet define in DW |
$87,775 |
|
Targeted Case Management |
$86,670 |
Data from the Allegheny County Analytics for FY 21/22
When considering all available
services associated and expensed across these 70 individuals, the total annualized
cost was $7,471,687 (Figure 7).
Figure 7: Annualized estimates for the 70 “First Referrals”
|
Estimated Annual ODS Funding for the group |
|
$4,391,355 |
|
Estimated Annual OBH Funding for the group |
|
$3,080,332 |
|
|
|
$7,471,687 |
Data from the Allegheny County ODS for FY 21/22
Partnerships
Allegheny County is pleased to be working with so many of our system partners both within and outside of DHS. The Executive Committee and various subcommittees include representation of Allegheny County DHS program offices, Community Care Behavioral Health Organization (our Behavioral Health Managed Care Organization), Pennsylvania’s DHS Office of Developmental Programs (including the Bureau of Autism Supports and Special Populations) and the Office of Mental Health and Substance Abuse Services.
System Analysis
One advantage to a project such as this is the opportunity to collaborate across offices within Allegheny County DHS. There is a chance to discuss how this project is to be implemented. Through these conversations, the planning team came to consensus on some key concepts:
- Look to broaden the ability to collaborate across stakeholders and within the same framework.
- Agree in our joint need to enhance our planning potential, by providing technical assistance to both service providers and supports coordinators.
- Uphold the commitment to equal participation in the Interagency
Team meeting process.
It is imperative to make connections across leadership that result in enhanced system knowledge and improved facilitation of complex case reviews. Ultimately, these connections will equip us as a county to provide enhanced responsiveness to crisis situations. Conversely, there are gaps in our interdisciplinary process around shared accountability, shared outcomes, and universal expectations around behavior supports. Related to workforce development, there is an acknowledgment that currently providers do not have an abundance of skilled and confident staff to support complex needs. There is also agreement in that being in a constant state of crisis response only allows for reaction not planning. Individuals who are active in the START model are the same as those who get stuck in highly restrictive settings, in part due to the lack of flexibility of the community setting or state regulations. Currently, there is no early involvement of clinical supports when there is NOT a crisis. Additionally, there tends to be no early learning about the individual, their history, or triggers. This learning could contribute to the development of a better response when a crisis is occurring. This is not only an educational need of providers, but for families as well. Finally, it is apparent that there are still silos across and between ID/A and BH services. This makes communicating individual needs and coordinating supports difficult. It also makes it difficult to recognize success when systems gauge success differently. The team will need to be able to address these gaps over the course of the pilot. If not to solve them, to address and include them in our future planning.
Outcomes and Business Questions
Pennsylvania’s ODP, OMHSAS, and Allegheny County will be exchanging data and reports as part of the pilot with the University of New Hampshire Center for Start Services. Allegheny County is working to ensure that the data being collected is representing an accurate depiction as to whether or not an impact is being made on the lives of those being served.
Through analyzing and monitoring of outcomes, Allegheny County hopes to demonstrate an overall improved quality of life has been achieved - whatever that life may include for each person. Everyone deserves the opportunity to be employed or experience some other form of meaningful day activity. All of us deserve and seek out friendships and other social connections. Meaningful activity, social connectedness, and support – however defined for and by an individual – is important to happiness, fulfillment, and well-being.
Currently, Allegheny County has an enormous amount of data, much of which is aimed at measuring service effectiveness. However, as part of this pilot, there will be measurements of other elements, including the following:
- Pre and post services and costs – this may determine if individuals are getting an enhanced or a different combination of services with better result.
- Direct
feedback and input from individuals, their families, and providers involved in
serving our target groups. Are their experiences and quality of life
improving?
- Incident reports, by person, and by reason. There will be a special
focus on the number of times law enforcement may have been called to assist
with a crisis. Is this number decreasing with the support of the START
team?
Finally, there will be activities related to tracking satisfaction of both individuals and families involved and getting support of the START team.
Early Challenges
There are some
challenges that have already been encountered through the initial phases of
this pilot. The first involves the multitudes of plans each system has. In ID/A
it’s the ISP (or Individual Support Plan). In Behavioral Health, every provider
and in some cases, every level of service or type of care, has its own service
and/or treatment plan. The START model has both a treatment and crisis plan.
How do the various service systems combine and reflect the START plans in the
ISP and BH Treatment plans? What are the best practices that assure information
is represented and used to guide services and supports needs? Secondly,
following a hospitalization, individuals and teams often need time to re-group.
Maybe the community home needs to add modifications or staff need a different
training than what was originally planned for. What service options need
planned for in order to support individuals between hospitalization and return
to the community/private home? Allegheny County is currently looking at gaps in
our housing continuum. There are limited “transition” or “step down” options
for individuals leaving highly restrictive settings prior to a full-time return
to the community setting. The feasibility of offering these types of settings
will be part of our work throughout the pilot. Finally, there will be focus on
determining the sustainability of the START model as part of the continuum of
treatment. Analysis of our data and outcome measures will be important in
making this determination.
Allegheny County is excited and humbled at the opportunity to contribute to system development and enhancement. With the support of everyone in the system – families, advocates, government officials, and service providers – individuals with disabilities can and should decide how to live their best life.3
References
1. Dr. Jill Hinton, The START Model: Mental Health and Crisis Intervention for People with IDD. Center for START Services – University of New Hampshire Institute on Disability/UCED, 2018
2.
Dr. Jill Hinton, The START Model:
Mental Health and Crisis Intervention for People with IDD. Center for START
Services – University of New Hampshire Institute on Disability/UCED, 2018
3. Pennsylvania Department of Human Services, Everyday Lives, 2016.
Biography
Brenda L. Bulkoski, M. Ed. has been the deputy director of the DHS Office of Developmental Supports since September 2019. As deputy director, Brenda L. Bulkoski oversees the daily operations of the Office of Developmental Supports. This includes assuring compliance with the Pennsylvania AE Operating Agreement, development of best practices, and maintenance of a strong and varied network of programs. Ms. Bulkoski has been active as an advocate for individuals living with intellectual disability and/or developmental delays since she started working as a DHS program specialist in May 1994. Ms. Bulkoski received her bachelor’s degree in Child Development from the University of Pittsburgh and her master’s in Special Education from Duquesne University.
Contact Information
Brenda L. Bulkoski
Deputy Director, Office of Developmental Supports
Allegheny County Department of Human Services
phone - 412-436-2804
fax - 412-271-1392 2020
K, Koffer Miller | 37-47
Volume 11 ► Issue 2 ► August 2022
A Conversation about Mental Health and Autism
Alice K, BS, CAPS
& Kaitlin H. Koffer Miller, MPH
The following article is an interview between Alice K, a peer support professional with lived experience as an Autistic person in mental health and substance use recovery, and Kaitlin Koffer Miller, a researcher and regional manager of the Autism Services, Education, Resources, & Training Collaborative (ASERT) Eastern Region, discussing the gaps, challenges, and opportunities of supporting someone with an autism spectrum diagnosis as well as co-occurring mental health diagnoses.
Kaitlin Koffer Miller (K): What are some misconceptions about mental health conditions among autistic individuals?
Alice K (A): One of the most challenging misconceptions is that autism, mental health, and other co-occurring conditions could be understood as separate entities and therefore treated by separate providers and systems. Although each diagnosis can create a unique experience, I find that it is nearly always the case that one needs to be addressed within the context of the other. The multifactorial nature of human experience may seem like commonplace understanding in our field; however, the challenge lies within the fragmentation between our service systems. When seeking services, as autistic individuals with mental health challenges, we are then put in a position to attempt to split ourselves into fragments as well, with few options of providers that have the expertise to understand and treat us as a whole person.
Sometimes a misconception in developmental disability services is that presenting behaviors have only to do with autism. On the mental health side, challenges may be perceived as strictly due to mental illnesses. This can be damaging, because it leads to an erasure of one’s true lived experience and can sometimes feel very invalidating. The truth is that it is usually a mixture of both. Anxiety or depression symptoms can be present, but the ways in which they operate in the autistic brain can be different, which means different approaches are needed. Without addressing both at once, mental health interventions are often like putting a bandage on the symptoms without addressing the root cause.
For example, when addressing a history of social difficulties in therapy, I have often been met with a cookie-cutter approach focusing on challenging negative beliefs and calming anxiety symptoms, overlooking much of what was driving the challenges to happen repeatedly. However, when understood in the context of autism, these seemingly negative beliefs and anxiety are often valid reflections of our experience and dismissing them can cause us to be put into situations where we may be misunderstood, manipulated, or bullied, which then exacerbates the existing anxiety. This may be a case where anxiety would be best addressed by understanding the underlying autism-related experiences and needs. Along with stress reduction, some helpful approaches could include learning some interpersonal skills and scripts for self-advocacy, implementing boundaries, and working through complex trauma.
On the other hand, it is sometimes helpful to understand the difference between autistic differences and mental health symptoms. For example, when we talk about neurodiversity, we are advocating for an understanding that every mind is unique and valuable, and promoting acceptance of different ways of feeling, thinking, and behaving with no one way being inherently better than another. This can be complex when supporting people who are facing mental health challenges. Many times, there are true diagnoses that need psychological and psychiatric intervention. At the same time, so much of the distress often comes from marginalization and oppression, which can be best alleviated through acceptance, accommodation, inclusion, and human rights. In the service system, it is important to, as much as possible, avoid re-creating this traumatic experience for an autistic person, especially for those with multiply marginalized identities.
I have often witnessed people’s autistic differences be misunderstood and pathologized as mental health symptoms. For example, some individuals need to move their bodies frequently or speak to themselves to pay attention, process information, or regulate their nervous system. This does not necessarily mean that they are experiencing psychosis or need to be medicated for an anxiety disorder. Some other people may have a strong need for structure, order, or repetition. This may just be how their brain optimally processes information, and not necessarily indicative of obsessive-compulsive disorder (OCD). In fact, many people on the spectrum feel at their happiest when they can freely rock, fidget, spin, repeat words, or fixate on a topic. And we have the right to do what makes us feel happy and safe, even if it may seem strange or inconvenient for the conventional world. Of course, many times mental health conditions do exist, and deserve to be treated. I find that the best way to go about untangling this is to let the individual lead the way. If something is causing them distress, then listen to that and find solutions together. However, if it is not currently a problem for them, then it's not a problem for me. I believe in granting individuals the dignity of risk. This means that as much as we want to protect people from harm, we must weigh these risks against those that come with diminishing the individual’s sense of empowerment to make their own decisions. This often requires time and patience for both parties, so keeping an open mind, not jumping to diagnoses and solutions, and respecting individual autonomy are key.
There are also a couple of autism-specific phenomena that mimic mental health issues, which can cause confusion for both autistic people and their supporters. Language and understanding for these are newly emerging, largely from the autistic community online. One example is autistic burnout. Autistic burnout occurs when external expectations, like long hours of socializing, working, being overstimulated, and the like, don’t match one’s internal capacities and resources for an extended period. It can result in symptoms like chronic exhaustion and hypersomnia, social withdrawal, inability to communicate, and difficulties functioning in other areas. Sometimes this is mistaken for depression, and one is encouraged to be more active and social, when usually rest and alone time can be most helpful. The autistic stress response to change in routines or environments is another example. This is not a simple anxiety issue. In addition to traditional coping skills, it is helpful for mental health providers to recognize the need for and explore with the autistic individual what kinds of concrete support they might need to ease into the change.
Another thing that comes to mind is the conversation about high and low functioning. First, I believe it’s just not accurate or useful to categorize someone’s level of functioning in a generalized and static fashion. People will start out with higher or lower abilities in different domains. From there, these functioning abilities can fluctuate often based on internal and external factors, including mental health symptoms. The great impact mental health has on autism-related functioning can be confusing for supporters. It may appear that the individual is not making progress or perhaps resisting treatment, supports, and becoming antisocial or antagonistic. The truth is that if or when someone’s mood is very dysregulated, they cannot access the skills and functionality that they may have been able to access at another time when their mental health is in a better state. There is a need for services to be very individualized and flexible to address these fluctuations. For example, there may be weeks when an individual is willing and able to focus on community participation. But then there are other weeks when mental health struggles may be more paramount, and telehealth could be helpful to meet them where they are. It’s also important to presume competence. Just because there are days that I struggle to do a task, does not mean that I am never capable at all.
K: What do you think about autism masking, anxiety, social situations, and the impact on mental health?
A: For me, I believe that masking and the lack of understanding of how autism presents in women in particular are a reason why I got diagnosed so much later in life. After years of unsuccessful therapy, I suspected I was on the spectrum, but I felt invalidated by those I tried to share these feelings with. I remember telling a psychotherapist about things I was experiencing that seemed to go beyond mental health to me, like differences in executive functioning, processing, and social skills and he insisted that they were due to depression. He said I was the most depressed person he had ever met but couldn’t come up with an explanation as to why it was so difficult to treat. He even said “Maybe that sounds like autism, but you don’t look like any of my Asperger’s clients that I have. You can make eye contact and hold a back-and-forth conversation. I don’t think you are autistic.” He then skipped over my concerns and did not recommend me for even an evaluation or follow-up with an expert.
The thing that many people don’t understand, is that just because I can do things like make eye contact, make small talk, quickly adapt to changes in routines, and the like, doesn’t mean these things are natural for me. I don’t necessarily have these functions as much as I perform them. This is called masking, which expends so much energy that it can take quite a toll on mental health. When that is compromised, I can’t mask as well and suffer social consequences that fuel further anxiety and depression. I feel that expecting individuals to mask and adapt to neuro-normative standards, which are present even in the structures of service systems, can negatively interfere with outcomes.
I understand the goal of psychotherapy as developing a deep understanding and relationship with oneself, which then leads to healthy relationships with the outside world. When forced to mask my autistic traits, I am in a constant state of trying to change who I am to appeal to what others need. It diminishes the ability to have a positive self-image and feel seen and valued in relationships with others. Masking is not something you can turn off; it’s a deeply ingrained way of being. So, how can you implement therapy with someone who is masking? When a person is not showing their true self? Or they don’t know who that self is? And how can we be expected to work on accepting ourselves when we feel like society doesn’t accept us?
Sometimes, with help, people can get to a point to where they can separate themselves from the mask, but often still intentionally must do so to get along in social situations, hold a job, or generally be treated well. But it can be exhausting. Draining that social battery can make it harder to engage in things that are good for mental health, like participating in activities, fostering relationships, and maintaining good physical health. Interestingly, I have observed that when autistic people interact with one another, whether it’s in a professional, peer relationship, or in a safe autistic community, they have much more energy and enjoyment in the experience. I’ve heard time and again, that it’s because the pressure to mask isn’t expected. For example, being able to stim, move around, talk about special interests, or take breaks without the need to explain ourselves, this can free up the mental space to be present and experience positive emotions. It boils down to being able to do things in a way that fits us and not feeling judged for it. Autistic peer relationships can result in much greater feelings of self-acceptance. Providers can also seek to adapt to some of the autistic person’s needs and preferences, and this sort of accepting relationship goes a long way in building trust enough to drop the mask and be truly seen, heard, and supported.
K: From your perspective in peer support and as someone with lived experience, what is most helpful in supporting those who have co-occurring mental health challenges?
A: First of all, connecting on a human level is of ultimate importance. This means stepping away from the medical model and allowing the individual to be the expert on themselves. It is helpful, especially in the beginning, to get to know someone while dropping assumptions, ideas about pathology, symptoms, and diagnoses for a while to fully understand the individual and the way they experience the world. Autism and mental health issues are very complicated and very intertwined. Focusing too much on labeling at first is not entirely possible and can often lead to confusion and misdiagnosis. Often, autistic people have gone through the world being told that who they are, how they think and behave are wrong. Providers can be more effective if they focus on undoing this negative bias, rather than reinforcing it.
Flexibility in the way we deliver services and supports is also key. I’m often asked how I think a service or training should be changed for autistic populations. I always say, there is no one cookie-cutter approach, as we all experience autism uniquely. While there are some predictable accommodations that may suit most autistic individuals, like a sensory-friendly environment, the most important changes will have to be in terms of flexibility. Preparing for extra time is often helpful for autistic individuals. This can range from longer appointment sessions to allow for information processing and breaks, to longer timeframes for goals and service duration. It could also mean lowering the expectations for time spent on socially and mentally draining tasks. Thinking about the rapport building stage in the peer support model is a good example. While in a traditional peer support service, the general expectation is that it could take 1-3 months to make progress on a goal. I have seen it take 2 to 3 times longer in autistic people, with the first few months just building a rapport and getting to know one another’s communication styles before implementing action steps. Sessions spent on assessments and treatment planning often also must be broken up into smaller chunks.
The structure and environment of services can also really impact how autistic individuals respond. For example, sitting in an office for an hour talking face to face with a therapist may not work for everyone. It may feel uncomfortable and unnatural to
a lot of people and prevent them from being able to engage and
open up, whereas having opportunity for movement, periods of silence, or doing an activity could be more beneficial. The way to find out what works is to ask the person or help them communicate their needs in whatever fashion
works for them.
Supporting autistic people and their related mental health can often feel challenging for providers. I promise you; it can be that much more challenging to live with. Although the task may seem daunting, I do also believe that effective supports led by and for the population they serve can bring about significant change. It can often require completely shifting one’s mindset and being open to thinking divergently with us. It can mean asking where our internalized ableism exists, and how to undo some of the oppression within our systems. I can also promise you that it can be well worth the time, energy, and patience required from all parties. I have seen amazing transformations occur when autistic people are treated with inherent dignity, worthiness, and value for who they are. I believe that by embracing neurodiversity, we help not only those with disabilities, but every human to accept themselves and slowly chip away at our masks, making us all a little bit more free.
Biography
Alice K is a project coordinator at the Policy and Analytics Center at the A.J. Drexel Autism institute. Alice is also a Certified Peer Specialist, Community Autism Peer Specialist, and spent five years providing direct support services. She is
also a neurodiversity advocate, speaker, and trainer. She has served as a consultant, content developer, and training facilitator for the novel Community Autism Peer Specialist initiative in Philadelphia and has also facilitated several mental health-focused
Certified Peer Specialist continuing education programs. She holds a bachelor’s degree in Behavioral Health Counseling from Drexel University.
Kaitlin Koffer Miller is the Regional Director of the Autism Services, Education, Resources, & Training Collaborative (ASERT) Eastern Region at the AJ Drexel Autism Institute. Ms. Koffer Miller’s work focuses in policy research as well as qualitative data analyses. Ms. Koffer Miller holds a master’s degree in Public Health from the Dornsife School of Public Health at Drexel University and is a doctoral candidate in Health Policy at the Dornsife School of Public Health at Drexel University.
Contact Information
Alice K, BS, CAPS
Project Coordinator
A.J. Drexel Autism Institute
Drexel University
ak3356@drexel.eduKaitlin Koffer Miller, MPH
Regional Director, ASERT Eastern Region
A.J. Drexel Autism Institute
Drexel University
Koffer Miller, Ardeleanu, Shea | 48-57
Volume 11 ► Issue 2 ► August 2022
The Importance of Measuring Changes among Individuals Leaving Institution-Based Care: An Example from the Field
Kaitlin H. Koffer Miller, MPH, Katherine Ardeleanu, MS, LGPC, &
Lindsay L. Shea, DrPH, MS
Introduction
In 1999, the United States Supreme Court ruled in favor of the respondents in the watershed disability rights case Olmstead v. L.C. Jonathan Zimring argued the case on behalf of plaintiffs L.C. and E.W. against the state of Georgia for undue institutionalization of persons1 with disabilities in direct violation of Title II of the Americans with Disabilities Act (ADA) of 1990 (Olmstead v. L.C., 1999). Title II of the ADA states that, “[s]ubject to the provisions of this subchapter, no…individual with a disability shall, by reason of such disability, be excluded from participation in or be denied the benefits of the services, programs, or activities of a public entity, or be subjected to discrimination by any such entity”.2 The Supreme Court’s interpretation of Title II of the ADA, the precedent set in the Olmstead decision, and the legal actions that have occurred since 1999 are only pieces of a larger deinstitutionalization movement that has been ongoing since the late 1960’s.3
As deinstitutionalization proceeded, adverse outcomes among individuals who transitioned from institutional settings into communities have been documented. Increases in the reliance upon community-based sources of services and support for mental health
and other care needs coupled with increases in the rates of homelessness and criminal justice system interactions have yielded widespread calls to action for improved transitions and system capacity building.4,5 Studies have found that
transitioning to community-based care has positive effects on quality of life, including more choice and access to activities.6,7 Emerging research continues to point toward improved outcomes among individuals with disabilities in communities,
when compared to institution-based settings, which further underscores the need to identify options for supporting community-based service delivery.
Pennsylvania has put in place multiple efforts to transition individuals from institutional-based settings into community-based care. The Bureau of Supports for Autism and Special Populations (BSASP) within the Office of Developmental Programs (ODP) has been supporting the transition of autistic individuals leaving Pennsylvania institutional settings, such as State Hospitals and State Centers, into one of the two BSASP adult autism programs: the Adult Autism Waiver (AAW) and the Adult Community Autism Program (ACAP). AAW and ACAP provide an array of home-and community-based services including assistive technology, behavioral supports, community supports supported employment, and more.8,9 For ACAP, as a managed care model, in addition to the previously described home-and community-based services, participants also receive their physical health services including doctor’s and dentist’s visits.9 The change in living circumstances, as well as service delivery and utilization coming from an institutional setting into a community, can be a tumultuous transition for an individual and their family and tracking changes in skills and adaptive functioning is critical. To that end, the ODP Clinical Team has implemented the ABAS-3 Adaptive Behavior Assessment System 3rd Edition (ABAS-3)10 to measure the skills associated with daily living among a sample of individuals entering the programs. The purpose of this paper is to determine the proof of concept for measuring differences across ABAS-3 scores among a sample of autistic adults who transitioned from an institutional setting into one of the two BSASP adult autism programs.
___
Methods
ODP Clinical Team members completed the ABAS-3 with State Center and State Hospital residents who were identified for transition into AAW or ACAP between August of 2017 and December of 2019. The ABAS-3 was administered before and after individuals transitioned from State Hospitals and State Centers into the programs. The ODP Clinical Team members administering the ABAS-3 included doctoral and master’s level clinicians with extensive experience administering assessment tools and overseeing service delivery to autistic adults. The timeline for completion of the ABAS-3 prior to discharge varied and the administration of the ABAS-3 following discharge occurred within 3 months after the transition from the institution to the community.
The ABAS-3 is a commonly used measurement tool among individuals with intellectual and developmental disabilities (IDD), autism spectrum disorder (ASD), learning differences, and other neurodevelopmental and psychological diagnoses across the lifespan
(birth-89 years old).10 Utilizing a tool like the ABAS-3 provides a formalized approach to measuring the successes and challenges experienced by an individual overtime and can be integrated into effective service planning.10 The ABAS-3 is an adaptive behavior rating scale that measures adaptive behavior at a global level (General Adaptive Composite, or GAC); domain level (Conceptual, Social, and Practical); and 11 individual skill area levels.10 The Conceptual
domain measures communication skills, including verbal and nonverbal skills, as well as academic capabilities across a range of subject areas.10 This domain also assesses several executive functioning skills, including decision making and
impulse control.
10 The Social domain measures social skills and respondents’ ability to successfully engage in community and social activities.10 Lastly, the Practical domain captures the ability to complete daily tasks and self-care activities,
such as shopping, bathing, and eating. Scores from this domain also indicate how well a person is able to take care of their health.10 Within the overarching adaptive domains, there are 11 measured skill areas including communication, community
use, functional academics, health and safety, home living, leisure, motor, self-care, self-direction, social, and work.10 ABAS-3 raters provide an ability rating, a frequency rating (i.e., 1 = never or almost never, 2 = sometimes, and 3
= always or almost always), and whether guessing was involved in the response.10 For each skill area, the respondent answers 20 to 26 items with higher scores indicating higher functioning in each area.10 The standardized
mean score for the GAC and each of the three domains is 100, with a standard deviation of 15. Data were entered into a secure platform for analysis.
Descriptive data were compiled to generate an understanding of the ABAS-3 scores across administrations and across reporters. Overall scores, adaptive score domains and skill area scores were generated for each administration.
Results
A total of nine individuals transitioned from a State Hospital or a State Center to either AAW or ACAP during the time period of this examination. The average age of individuals transitioning was 36 years old. Two individuals only had ABAS-3 measures
completed at one timepoint. Most individuals with two ABAS-3 measures completed before and after a transition from a State Hospital or State Center into a AAW or ACAP had a two-year period between their first ABAS-3 and the second ABAS-3. One individual
had eight days from their first ABAS-3 to their second ABAS-3.
Among the seven individuals who had ABAS-3 measures completed while in a State Hospital or State Center, there was an average score increase of 1.33, or a slight improvement or increase across the timepoints. Increases in averaged scores across all three
adaptive domains were observed. The average conceptual skill area increased by 2 points, the average social skill area increased an average of 2.67 points, and the practical skill area increased an average of 0.44 points. Although overall average
scores increased, there was variation across ABAS-3 GAC scores among individuals. Of the seven individuals with ABAS-3 measures at more than one timepoint, ABAS-3 GAC scores did not change for three individuals and ABAS-3 GAC scores changed for four
individuals. Among these four individuals, the score changed from below average (score range 80-89) to low (score range 70-79) for one individual and from average (score range 90-109) to below average (score range 80-89) for a second individual. Among
individuals with GAC score increases, the score range shifted from low (score range 70-79) to below average/average (score around 90) and from extremely low (scores below 70) to low (score range 70-79).
Discussion
ABAS-3 measures were successfully completed on a small sample of autistic individuals who transitioned from a State Hospital or a State Center to AAW or ACAP. It is noteworthy that this process was implemented through collaborative efforts of the leadership and staff at the State Hospitals and State Centers and at ODP. The forethought and planning to put in places measures of the transition should be applauded, since it represents a step forward in bridging the gap from institution-based care to community-based case.
Overall, there were improvements in overall ABAS-3 GAC score and in skill area scores as well. Although these findings warrant further study and replication, they point toward reinforcing the deinstitutionalization of individuals with disabilities. Further linking these findings to the services and supports received by these individuals during their time spent in a State Hospital or State Center, their transition services, and the services received in community-based programs is a critical next step for this work. Documenting the demographic and clinical characteristics of this group also warrant additional attention, as there may be important differences that point toward documented health inequities across populations and critical markers for needed clinical services and supports.
Limitations of this analysis include a small sample for observing changes in ABAS-3 scores and some variability in the duration between ABAS-3 administrations. ABAS-3 scores were generated pre-and post-a transition out of a State Hospital or State Center
and the transition served as the index event. However, the length of time between the ABAS-3 scores before and after the index event varied, especially for one exceptionally short difference (8 days) in time between the first and second ABAS-3 administration.
The utility of the ABAS-3 for the intended purpose has not, to our knowledge, been replicated in other research or program practices and continued efforts to assess optimal measures should be considered. Another limitation would be that what services
the individuals received when they transitioned into either AAW or ACAP from the State Centers was not analyzed for the purpose of this study. Therefore, it is not known what level of services and supports the individual is receiving which could impact
their ABAS-3 score.
Proactive and intentional efforts to understand and document the experiences of individuals who transition from institutional settings into community-based programs should be a priority across the US. Identifying optimal outcomes could point toward promising transition planning and processes and the observation of suboptimal outcomes serves an indicator for areas for focus and improvement in implementing needed services and supports.
References
1. Musumeci M, Claypool H. Olmstead’s role in community integration for people with disabilities under Medicaid: 15 years after the supreme court’s Olmstead decision. 2014.
2. Americans with Disabilities Act of 1990. In: 1990 AwDAo, editor. Pub L No 101-336, 104 Stat 3281990.
3. Larson S, Ryan A, Salmi P, Smith D, Wuorio A. Residential Services for Persons with Developmental Disabilities: Status and Trends Through 2010. 2011.
4. Franklin MS, Bush C, Jones KA, et al. Inequities in Receipt of the North Carolina Medicaid Waiver Among Individuals with Intellectual Disability or Autism Spectrum Disorder. Journal of developmental and behavioral pediatrics. 2022;doi:10.1097/DBP.0000000000001075
5. Beadle-Brown J, Mansell J, Kozma A. Deinstitutionalization in intellectual disabilities. Current opinion in psychiatry. 2007;20(5):437-442. doi:10.1097/YCO.0b013e32827b14ab
6. Chowdhury M, Benson BA. Deinstitutionalization and Quality of Life of Individuals With Intellectual Disability: A Review of the International Literature: Deinstitutionalization and Quality of Life. Journal of policy and practice in intellectual disabilities. 2011;8(4):256-265. doi:10.1111/j.1741-1130.2011.00325.x
7. Larson S, Lakin C, Hill S. Behavioral Outcomes of Moving from Institutional to Community Living for People with Intellectual and Developmental Disabilities: U.S. Studies from 1977 to 2010. Research and practice for persons with severe disabilities. 2012;37(4):235-246. doi:10.2511/027494813805327287
8. Pennsylvania Department of Human Services (DHS). Adult Autism Waiver. Accessed 4 August 2022, https://www.dhs.pa.gov/Services/Disabilities-Aging/Pages/Adult%20Autism%20Waiver.aspx
9. Pennsylvania Department of Human Services (DHS). Adult Community Autism Program (ACAP). 4 August 2022. https://www.dhs.pa.gov/Services/Disabilities-Aging/Pages/ACAP.aspx
10. Harrison PL, Oakland T. Adaptive Behavior Assessment System, Third Edition (ABAS-3). Western Psychological Services; 2015.
Biography
Kaitlin Koffer Miller is the Regional Director of the Autism Services, Education, Resources, & Training Collaborative (ASERT) Eastern Region at the AJ Drexel Autism Institute. Ms. Koffer Miller’s work focuses in policy research as well as qualitative data analyses. Ms. Koffer Miller holds a master’s degree in Public Health from the Dornsife School of Public Health at Drexel University and is a doctoral candidate in Health Policy at the Dornsife School of Public Health at Drexel University
Katherine Ardeleanu, is a PhD student at Drexel University’s Dornsife School of Public Health. She is also a licensed graduate professional counselor and holds a master’s degree in mental health counseling from Johns Hopkins University. Her
work focuses on improving access to and quality of mental health services for underserved populations.
Lindsay Shea is a Senior Healthcare Analyst supporting data and policy efforts in ODP’s BSASP. She is also an Associate Professor at Drexel University, and holds a master’s degree in social policy from the University of Pennsylvania and a doctoral degree in health policy from Drexel University.
Contact Information
Kaitlin Koffer Miller, MPH
Regional Director, ASERT Eastern Region
A.J. Drexel Autism Institute
Drexel University
Katherine Ardeleanu, MS, LGPC
PhD Student, Health Services Research & Policy
Dornsife School of Public Health
Drexel University
Lindsay L. Shea, DrPH, MS
Senior Healthcare Analyst
Office of Developmental Programs, Bureau of Supports for Autism and Special Populations
Morgan | 58-63
Volume 11 ► Issue 2 ► August 2022
Exploring Misconceptions about Co-occurring Mental Health Conditions in Autistic People
Lisa
Morgan, M.Ed., CAS
Among the various myths and misconceptions about autism is the idea that autism causes co-occurring mental health conditions. While it’s true that there are many autistic people living with anxiety, depression, suicidal ideation, and other co-occurring mental health conditions, the root cause is not autism. According to the lived experience of autistic people, there’s another explanation.
As an autistic adult diagnosed later in life at 48 years old, and a suicide loss and attempt survivor who lives with post-traumatic stress disorder (PTSD) and high anxiety, I believe the biggest misconception about co-occurring mental health conditions among autistic adults is that they are caused by having autism.
They are not.
I submit that co-occurring mental health conditions are caused by living with autism in our society.
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) explains autism as a neurodevelopmental spectrum condition with or without intellectual disability in the areas of social communication and interactions, and restricted, repetitive behaviors. My belief, along with many other autistic people, is that autism is a different way of being.
It is a culture.
A culture of people who, over time, can and do develop co-occurring mental health conditions related to living as an autistic person. Indeed, a research study from Denmark found more than 90% of autistic people who attempted or died by suicide had at least one co-occurring mental health condition of which anxiety was most prevalent.1 A different study discovered that 66% of newly diagnosed autistic people had contemplated suicide, compared to 17% in the general population.2,3
I’m convinced, through my own lived experience, supplemented by research findings and the experiences of other autistic people, that the reason why there is a high incidence of co-occurring mental health disorders among autistic people is that professionals, families, and even friends do not accept autistic people as autistic people. The message autistic people receive is that it is not ok to be themselves, and that starts at a disturbingly early age. Knowing I was different, but not knowing why. Understanding that I did not fit in, but also not knowing how to fit in. And finally, being the brunt of bullying and rejection over and over again while growing up due to my peers sensing something different about me, resulted in me getting the message that it was not ok to be me. That in itself had an extremely negative impact on my mental health and had nothing to do with my autism, except for it not being accepted.
As autistic people work through all the misunderstandings, thwarted belonging, invalidation, masking, and anxiety of attempting to find a place in society, our mental health is negatively affected. To be honest, I enjoy the way my autistic mind works. I love the out-of-the-box problem solving, visual thinking, creativity, and being non-conventional. Also, to be honest, it seems like most people in society want me to be someone I’m not, as long as it fits within the accepted social parameters set up by society.
For instance, we must mask our autism to be accepted in today’s society. Masking is a social strategy autistic people use to fit in, be accepted, and not “look autistic.” In order to mask successfully, we have to suppress all sensory onslaught and stimulation, while determining the emotions of the people we are with to know if we have to put on a smile or a sad face, while keeping track of the conversation, figuring out what to say next in enough time to participate, stand the correct distance apart, be more vocal than we are comfortable being, laughing at innuendos and figurative language we do not understand, refusing to stim, while trying to pay attention to what we are communicating non-verbally, and finally—make it all look simple and natural.
It is beyond exhausting and leaves autistic people feeling isolated because we know if we did not mask, we would not be accepted. So, while masking helps us to socialize and to fit in, it also leaves autistic people feeling lonely and unknown for who they truly are as a person.
Many times, autistic people are also left with a weak to non-existent sense of self. Autistic people diagnosed later in life like me have been masking for so long that we never developed a sense of self. We need to take the time to figure out who we really are, not spend time trying to emulate who we need to be to fit in.
It’s important to know masking is a unique risk factor for suicide for autistic people.2
Not accepting autistic people as autistic people may put them at risk for suicidal thoughts and behaviors, which has a negative impact on their mental health.
In my work with autistic adults, I have found the most helpful, valuable, and meaningful interaction we have is when they realize I understand them. Understanding has a healing effect on autistic people who have rarely been understood. Being able to be themselves with no judgment, no explanation, and no misunderstandings is a balm on their wounded souls. I watch as they smile, feel more confident, and rest in the knowledge that who they are is enough and that I’d actually prefer their autistic self over their masked self.
The co-occurring mental health challenges autistic people face are mostly due to not being accepted for who they inherently are as autistic people, so they have to mask. They have to hide their stimming, which leads to higher anxiety because stimming helps autistic people to regulate. They have to be someone else, talk in a way that feels unnatural, put the ‘right’ face on, and fight against what feels natural for them whenever they are with other people who do not or cannot accept their autism.
To support autistic people with co-occurring mental health conditions, let them know it’s ok to be themselves. It’s ok for them to stim, to not make eye contact, to ask for a conversation to slow down so they can participate, and to make the environment
comfortable for them as well.
Let autistic people know it’s ok to clarify meanings of figurative language, to talk about things they want to talk about, to be rule-based. Support autistic people with co-occurring mental health challenges by letting them know it is ok to be themselves, whatever that looks like, and learn as much as you can about the autism culture from authentically autistic people. Once you know and understand the culture of autistic people, join them. I’m sure the co-occurring mental health challenges will dissipate along with the misconceptions about co-occurring mental health challenges.
References
1. Kõlves K, Fitzgerald C, Nordentoft M, Wood SJ, Erlangsen A. Assessment of Suicidal Behaviors Among Individuals With Autism Spectrum Disorder in Denmark. JAMA network open. 2021;4(1):e2033565-e2033565. doi:10.1001/jamanetworkopen.2020.33565
2. Cassidy S, Bradley L, Shaw R, Baron-Cohen S. Risk markers for suicidality in autistic adults. Molecular autism. 2018;9(1):42-42. doi:10.1186/s13229-018-0226-4
3. Cassidy S, Bradley P, Robinson J, Allison C, McHugh M, Baron-Cohen S. Suicidal ideation and suicide plans or attempts in adults with Asperger's syndrome attending a specialist diagnostic clinic: a clinical cohort study. Lancet Psychiatry. Jul 2014;1(2):142-7. doi:10.1016/S2215-0366(14)70248-2
Biography
Lisa Morgan, founder and co-chair of the Autism and Suicide committee of the American Association of Suicidology, is an autistic self-advocate in crisis supports for autistic people. Lisa has a master’s degree in Special Education and is a certified autism specialist. Owner of Lisa Morgan Consulting LLC, Lisa helps autistic people utilize their autistic strengths to have a better quality of life. Lisa’s books, articles, and resources can be found at http://www.autismcrisissupport.com.
Contact Information
Lisa Morgan M.Ed. CAS
Co-chair Autism and Suicide Committee of AAS
Lisa Morgan Consulting, LLC
Board Certified Autism Specialist
lisamorganconsulting@gmail.com