Positive Approaches Journal, Volume 11, Issue 4
| Site: | My ODP |
| Course: | My ODP |
| Book: | Positive Approaches Journal, Volume 11, Issue 4 |
| Printed by: | |
| Date: | Tuesday, July 14, 2026, 5:24 PM |
Positive Approaches Journal | 6-7

Volume 11 ► Issue 4 ► February 2023
Access, Empowerment, Experience: Driving Voice Behind Change
Introduction
Everyone advocates in their everyday lives, but for people with disabilities, advocacy can look different. From autism advocacy to peer-to-peer advocacy, family advocacy and more, advocacy means supporting someone in the way that works for them before it becomes a crisis and to enhance their life.
This issue of Positive Approaches focuses on the importance of advocacy through multiple perspectives and voices. It is important to teach all people about advocacy because advocacy connects people to their community and helps them navigate different service systems and everyday life. It is important to have access to advocacy resources to support people with activities such as going to the doctors, talking to police, and more. Advocacy includes the words people use, how they speak about disabilities, and how they speak about people with disabilities. Let advocates use their words freely. Let them choose the words and labels for themselves that work for them. Just because we do not share the same values, does not make someone’s chosen words and labels wrong. Everyone has a voice and deserves to be heard, and to live “my life, my way.” This can be accomplished through advocacy.
The first thought when someone needs support should not be to put someone in an institution or residential setting. We need to do a better job of looking at the things we do that keep people from self-advocating, and how we can encourage self-advocacy instead. We need to create more ways to enhance self-advocacy skills in all people. When being an advocate for someone else, it is important to be respectful of their life experiences and choices. It is important to consider the advocates preferences on how they want their family to be involved in their life.
The biggest barrier for me when I first started speaking up for myself was getting connected to people who would listen. I continued to speak up until someone listened and believed in me. Once I had that one person, I was able to get connected with other people who would listen. My life is different because I spoke up and advocated. Just look at me now: I’m one of the founders of Self Advocates United as 1 (SAU1) and was the president for 10 years. After serving as president, I became a mentor to our next president. I was then asked to become a member of SAU1’s staff because they did not want to lose my voice. As part of SAU1’s staff, I am still a leader in the organization today as the lead Power Coach and Ambassador.
The best people who support me to speak up are the people that I choose. These people are people that care, but also people who take time to listen and make sure they understand what I am saying. They help me get my words out instead of pretending they know what I said when they don’t.
The one piece of advice I would give to supporters of people with disabilities is to care about the job you do. If a supporter cannot demonstrate they care about the person’s voice, they cannot be successful in advocating for them. If the person cannot demonstrate they care, this job may not be a good fit for them. It is important to have caring support because people with disabilities need to be able to speak up about what they want and need and know that they are being heard and respected.
This issue will give readers an understanding of these parts of advocacy and more.
Oscar Drummond
Lead Power Coach and Ambassador
Founder and Past President of Self Advocates United as 1
Positive Approaches Journal | 8-13
Volume 11 ► Issue 4 ► February 2023
Data Discoveries
The goal of Data Discoveries is to present useful data using new methods and platforms that can be customized.
There have been tremendous movements in the autistic community focused on self-advocacy and neurodiversity shifting away from previously parent-dominated spaces.1,2 Self-advocacy groups are a platform for individuals with many disabilities and diagnoses, including autism, to gather, learn from the lived experiences of others, share resources and information, or to advocate for issues impacting the community in online or in-person settings.3 While both parent-led and autistic-led groups are important and have a place in the autism community, they serve different purposes and it is critical that autistic individuals have peer-driven spaces, not only groups that are created by parents or neurotypical professionals.4 A primary benefit of autistic-led environments is that it affords participants the ability to strip the “mask” that is often needed for neurotypical-centered environments, allowing for a more comfortable setting where the focus can be on the activity, not on hiding autistic characteristics.5
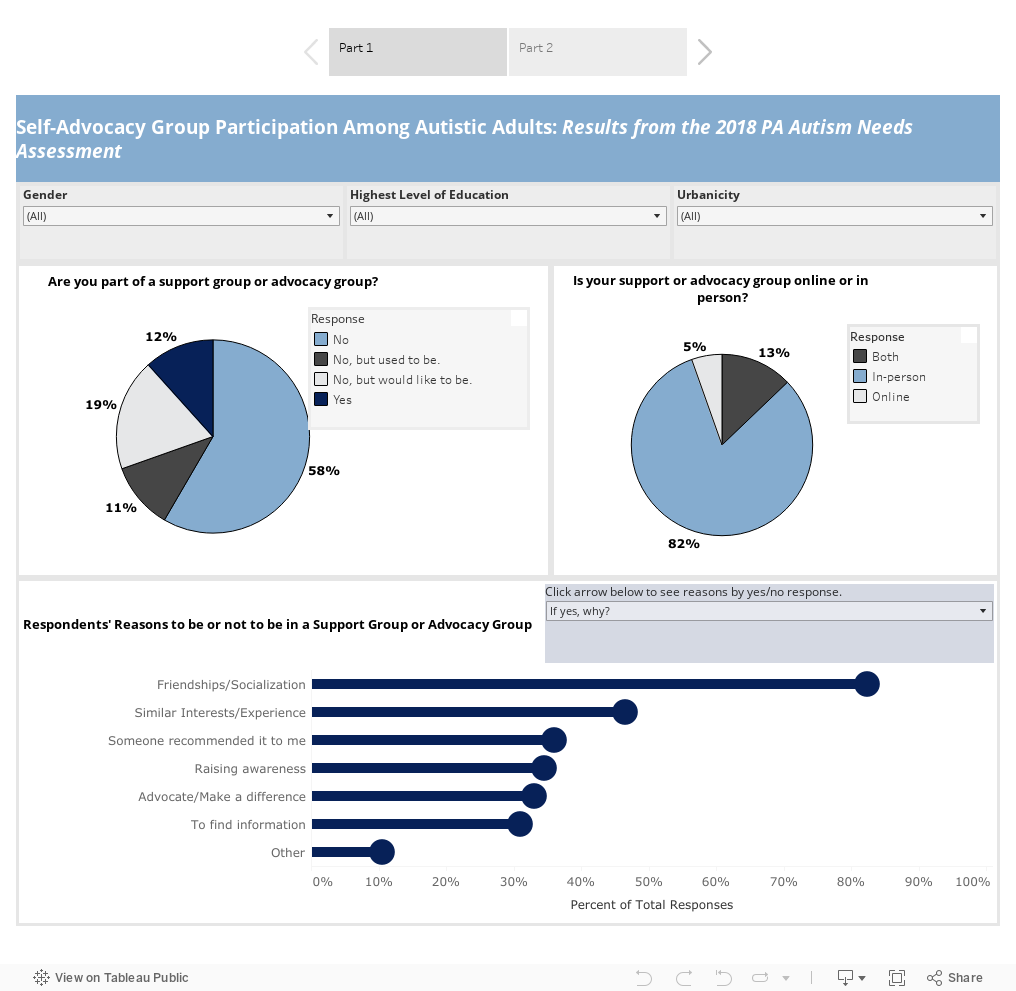
In Pennsylvania, the Autism Services, Education, Resources, & Training Collaborative (ASERT) conducted the 2018 Pennsylvania Autism Needs Assessment (2018 PANA). More than 8,000 autistic individuals and their caregivers completed the 2018 PANA providing information about demographic, clinical characteristics, and other service experiences. For more information about the 2018 PANA and to view more data, visit: www.paautism.org/needsassessment. For the purposes of this data dashboard, only responses related to self-advocacy group participation from autistic adults over the age of 18 were included. In this sample, we found that 58% of autistic adults participated in a self-advocacy or support groups. To view more details about the reasons for participating or not participating in self-advocacy groups and the format, please visit the data dashboard below. In another set of questions, autistic adults were asked if they were satisfied with the amount of time spent involved in a self-advocate run group. The majority of respondents (69%) indicated that they do not spend enough time participating in this activity, though only some respondents (25%) indicated that participating in self-advocate-run groups was important them.
The data dashboard below shows responses to the 2018 PANA questions about support and self-advocacy group participation. The first tab shows a visualization of whether respondents participate in support or self-advocacy groups and whether the group is online. There is also a bar chart that can be filtered to show the reasons for participating or not participating in a support or self-advocacy group. The second tab shows two questions related to participation in self-advocate-run groups including the frequency of participation in the activity and whether the activity is important. There are filters on both tabs to explore the data by gender, education level, and urbanicity (living in an urban, rural, or suburban location).
Conclusion
The ASERT Collaborative website has a plethora of resources focused on support groups and self-advocacy groups for autistic individuals. One of ASERT’s hallmark resources is a clickable map with online and in-person support and self-advocacy groups by county. ASERT also has a resource to provide step-by-step guide on starting a self-advocacy group. The ASERT Collaborative supports the PA Gatherings: Critical Topics in Autism which are virtual events hosted by two self-advocates from the Central Region of PA with a focus on increasing knowledge and awareness of resources about issues that are important to the autism community. One PA Gathering in January 2022 focused on self-advocacy stories, experiences, and resources. The Philadelphia Autism Project highlights, among other initiatives, self-advocacy and support groups that are funded by seed awards, a small start-up capital for initiatives in Philadelphia that support autistic individuals and their families.
References
1. Leadbitter K, Buckle KL, Ellis C, Dekker M. Autistic Self-Advocacy and the Neurodiversity Movement: Implications for Autism Early Intervention Research and Practice. Frontiers in psychology. 2021;12:635690-635690. doi:10.3389/fpsyg.2021.635690
2. Ne'eman A, Bascom J. Autistic Self Advocacy in the Developmental Disability Movement. American journal of bioethics. 2020;20(4):25-27. doi:10.1080/15265161.2020.1730507
3. The ASERT Collaborative. Starting an Autism Support/Self-Advocacy Group. Accessed 9 January 2023, https://paautism.org/resource/support-self-advocacy-group/
4. Crane L, Hearst C, Ashworth M, Davies J, Hill EL. Supporting Newly Identified or Diagnosed Autistic Adults: An Initial Evaluation of an Autistic-Led Programme. Journal of autism and developmental disorders. 2021;51(3):892-905. doi:10.1007/s10803-020-04486-4
5. Belek B. ‘A Smaller Mask’: Freedom and Authenticity in Autistic Space. Culture, medicine and psychiatry. 2022:1-21. doi:10.1007/s11013-022-09794-1
Chvasta | 14-22
Volume 11 ► Issue 4 ► February 2023
What Are the Barriers to Becoming a Self-advocate: How Do We Perpetuate Them and How Can We Lower Them?
Kyle Chvasta, MSW
What is self-advocacy?
Advocacy is generally defined as the act or process of supporting a cause. For those of us in the disability community, the causes can vary. This includes reducing barriers to programs like Medicaid, to guaranteeing other programs like home and community-based
services are well-funded, and to making sure community amenities, like sidewalks and buses are accommodating and accessible. Advocacy is the process to achieve an effective and transformative policy decision through education, direct action, lobbying,
and other forms of influence. The goal of an advocacy campaign may be creating a policy decision or to raise awareness of a specific subject. Advocacy can be fluid because it links to shifting priorities for both the advocate and the decision maker.1
And as the built environment, society, and the disability rights zeitgeist are always in flux, as are advocacy priorities. Ideally, the architects of advocacy movements should be those with lived experiences, situated at the intersections and avenues
being advocated for. That is self-advocacy. The self-advocacy movement is constructed to ensure that the work to influence policy and practice gets done while reflecting the expressed needs and desires of those in the disability community.
What can self-advocacy look like?
The 1977 Section 504 Sit-in 2 & the American Coalition of Citizens with Disabilities is a clear and seminal example of protest and advocacy in action from within the disability community. The Sit-in was a disability rights protest that began on April 5, 1977. The disability community at large occupied federal buildings in the United States to push the issuance of long-delayed regulations regarding Section 504 of the Rehabilitation Act of 1973. Prior to the 1990 Americans with Disabilities Act, the Rehabilitation Act was the most important disability rights legislation in the United States.3 Their coordinated campaigning, lobbying, and direct actions ensured that for the first-time, disabled people had federal civil rights protection. Since then, we have seen the self-advocacy movement grow and expand.
Why is self-advocacy important?
Self-advocacy is needed to advance the rights of disabled people, like the 504 Sit-in and subsequent advocacy initiatives did. Self-advocacy is a direct response to being overlooked in policy planning and implementation. We have seen the self-advocacy movement and the disability rights movement at large emerge in every region of the world, and self-advocates are calling for a recognition of their human rights and campaigning for a central role in determining those rights. 4
How do we create healthy self-advocacy spaces?
It is critical for those of us who call ourselves self-advocates to investigate our own work and whether there are access points to those who want to join us. Are the inroads into the world of self-advocacy clear and accessible? Does internalized ableism, racism, and classism impact the spaces we want to create? Are there obvious access points to our advocacy work or does suboptimal messaging close any open doors? Are we missing overlooked corners of our community? Are some needs and desires expressed above others?
Outreach
There is power in numbers. When we work together, we can direct policy and practice into a more just and equitable direction.
How can we increase our coalition? The effective, efficient, clear, and accessible use of various outreach modes is a vital component and the cornerstone of community and advocacy engagement. A suboptimal outreach plan is akin to the thought experiment of “the tree falling in the woods:” If no one knows what our movement is about or that it is even happening, is there a movement? We can form internal committees, host meetings, or write a manifesto. But when a movement consists of a small, insular group of people, it raises questions about viability and success.
It is crucial to conduct regular, accessible, and clear outreach. This means that, on a regular and consistent basis, we are disseminating outreach materials. Sporadic bursts of dissemination do not create or hold an audience. A good example of a group conducting consistent and transparent outreach is the Autistic Self Advocacy Network. Through a dedicated Twitter feed, newsletters, and press releases, they alert their large audience about advocacy opportunities, policy changes, and ways to get involved.
Material accessibility is also a key factor. If outreach messaging is highly academic language, filled with jargon and acronyms, or is difficult to read, it will only court a small group and can alienate others. Prospective participants should be able to easily understand what an advocacy movement is about from a few sentences on outreach materials.
Mode also matters. Digital outreach may seem ubiquitous in 2023, but organizers should consider all options. According to the United States Census Bureau, more than 40 million people in the United States have a disability. But even as most Americans report having certain technology, the digital divide between those who have a disability and those who do not remains. 62% of adults with a disability say they own a desktop or laptop computer, compared with 81% of those without a disability. As for smartphone ownership, there is a 16% gap between those with a disability and those without one (72% vs. 88%).5 While social media and other digital forms of outreach can bridge vast geographic divides, these modes may not be as accessible as we think.
Sometimes meeting people “where they are” is also not enough. We should meet people where they live and congregate. This means venturing out to the places and spaces people reside, where people share space, or are taken care of. This may be identifying community centers, as well as trusted community members and leaders who can connect us with the groups and individuals who may be left in the digital chasm of “tech-inequity.” These are the moments where “old-fashioned” portable printed materials could be ideal. Language and cultural considerations are also important. Are we considering people using assistive reading devices? When we conduct outreach through a homogeneous framework and ignore intersectionality, we run the risk of isolating potential advocacy partners. Consider developing outreach materials in multiple languages and working with trusted local advocates who can connect us with communities of various languages.
Welcoming spaces
To build an advocacy movement is to build community. Welcoming and hospitality are parts of a healthy and successful community. The success of movement membership acquisition and retention are deeply rooted in how we build, share, and uphold space with one another. To do this, we must ask ourselves: are the spaces where we host meetings not just accessible to everyone, but are they comfortable, warm, and safe? Accessibility does not simply mean a space meets the most basic accommodation standards for someone with a disability; there are other factors to consider. How is the lighting? Is there enough accommodating space at the table for someone using a wheelchair? Is it a private space for those who may want anonymity? How is the temperature for those with hypersensitivity? Are we prepared to share space with those using assistive communicating technology? Are we amenable enough to make changes if requested? Is there a hybrid or online meeting space option? And if there is, have we exhausted all the accessibility options at our digital meeting space?
Community building also means building relationships and showing curiosity in new members. Social interactions can present unique factors for some of us to navigate and striking up a conversation may not be ideal for all organizers in the disability community. Having a built-in mechanism to “break the ice” can ease nervous energy for those seeking to enter a community or movement. An example of this can be a habitual icebreaker during meetings. Doing this, in conjunction with the caveat that participation is not compulsory, can be helpful. Providing the icebreaker ahead of time can also reduce anxiety. Opportunities for people to introduce and share can truly make people feel seen and heard.
It is also advisable that we be transparent about our mission, vision, practices, and ethics. A clear and concise FAQ page, about us page, or mission statements on websites can scaffold this effort. Clear boundaries are important in building a convivial and safe advocacy space. Understanding and communicating our stance on power dynamics, relationships, roles, and ways in which we interact with one another, is vital. When there is a lack of clear or ethical boundaries, we risk fostering untenable situations. Formalizing bylaws and codes of conduct can guide us in our work.
Training and mentoring
A component of building a welcoming space means embracing the opportunity to mentor and train emergent self-advocates. We can open up learning spaces by providing online learning and training materials. As time and resources allow, we can provide professional development, seek, or establish mentoring and training scholarships, and host regular question and answer sessions with potential self-advocates. When people feel as if they are welcomed to learn and ask questions in a safe and supportive environment, we can increase member retention.
Time and Capacity
As stated earlier, advocacy is comprised of education, lobbying, direct action, dissemination, and the general activities of movement building. All of this takes time, which is one of the greatest barriers to advocacy. Time is a commodity few can easily sacrifice. One may be limited by various commitments, doctors’ appointments, transportation logistics and variables, as well as familial and community obligations.
Removing this barrier requires transparency about time commitments and creating opportunities at different commitment levels. If funds allow, pay community members who are actively educating and working with policymakers to supplement any time taken off work or lack-there-of. We can also establish community support funds to offset the labor produced by self-advocates. Creating caring networks to assess and address any barriers self-advocates may face. This can look like establishing care for family members, providing case management for someone seeking healthcare, or other aid. We should also operate with a sense of flexibility. Some people can only participate sporadically, and we should make it clear that a varied level of commitment is acceptable, and they are welcome. If there is a large time commitment, we need to be upfront about that or direct people to alternative less time-consuming ways of getting involved.
Finally, it is vital that we conduct regular wellness checks and help members avoid burnout. Serving as a self- advocate can be a rewarding experience, especially when we see the difference we are making in our collective work. However, if we are constantly
giving and not taking time to refill our cups, we put ourselves at risk for burnout. We do not want to place people in a state of physical or emotional exhaustion, accompanied by a loss of passion for the work. Once these and other factors are considered,
we can begin to safeguard our collective work and take the important next steps of regularly evaluating our privilege and ensuring our self-advocacy work is intersectional. These simple recommendations can hold water. In the meantime, it is important
we start from a place where we are evolving, questioning, and investigating how we can dismantle barriers to self-advocacy.
References
1. Strunk, Ellen R,P.T., M.S. What is advocacy? GeriNotes. 2021;28(3):5-6. http://ezproxy2.library.drexel.edu/login?url=https://www.proquest.com/trade-journals/what-is-advocacy/docview/2536552850/se-2.
2. DREDF. Short History of the 504 Sit in. Disability Rights Education & Defense Fund. Published April 4, 2013. https://dredf.org/504-sit-in-20th-anniversary/short-history-of-the-504-sit-in/
3. Freeman J, Johnson V. Waves of Protest : Social Movements since the 1960s. Rowman & Littlefield Publishers; 1999.
4. Charlton JI. Nothing About Us Without Us : Disability Oppression and Empowerment. University of California Press; 1998.
5. NW 1615 LS, Suite 800Washington, Inquiries D 20036USA202-419-4300 | M88 | F44 | M. Americans with disabilities less likely than those without to own some digital devices. Pew Research Center. Published September 10, 2021. https://www.pewresearch.org/fact-tank/2021/09/10/americans-with-disabilities-less-likely-than-those-without-to-own-some-digital-devices/
6. How to Be an Advocate for Yourself and Others. The Well Project. Published March 18, 2019. https://www.thewellproject.org/hiv-information/how-be-advocate-yourself-and-others
Biography
Kyle Chvasta is a Macro Social Worker and Autistic-advocate with experience in public policy and health education. His background is in creating public health information access points for those living in Philadelphia, with a particular focus on breaking down healthcare stigma and addressing the systems that perpetuate adverse health outcomes. He has years of experience developing and implementing mechanisms for accessible public health education. His current area of focus is data translation and making the connection between autism research, policy, and the communities and people autism research could have an optimal impact on. His work is structured around the principle that one must address systemic and structural issues that create adverse conditions, impacting health outcomes. He also frames his projects and work within the belief that one must acknowledge and unpack one’s own privilege to dismantle racist, classist, and ableist systems. He works to integrate these radical models into his personal and professional practices.
Contact Information
Kyle Chvasta, MSW
The Policy Impact Project a program of the Policy and Analytics Center at the A.J. Drexel Autism Institute
Research associate, Project manager
kc3673@drexel.eduGuttentag | 23-30
Volume 11 ► Issue 4 ► February 2023
The Complicated Language of Autism Advocacy: Learning to Use Our Words
Rachel Guttentag
I am a self-advocate. I am on the spectrum. I am autistic. I am disabled.
These are the words, the labels, I choose to use for myself.
Though person-first language (person with autism) was long thought to be the most sensitive way to phrase things and remains the recommended phrasing in some circles, the rise of identity-first language has become an undeniable hot-button topic. It is a growing preference among autistic self-advocates to be referred to as an autistic person (or just autistic) rather than a person with autism. Unlike others, I don’t stringently hold to this phrasing. You will sometimes find me switching between the two when I write depending on what flows better. Still, I resonate with the idea that autism cannot be separated from me the same way you would want to separate a person with cancer from the disease killing them. We may not say “cancerous person,” but the reality of autism is more complicated than a disease infecting its host. Unlike the attention deficit hyperactivity disorder (ADHD) I also struggle with, I cannot conceive a version of myself if I did not have autism. I cannot envision it being neatly removed. I would not be the person I am without it, for both better and worse. There is no clear way to separate its symptoms from simply me being me. It is the lens through which I have always viewed my reality. I have lived with it my whole life, and it has shaped me accordingly, even in the ways it has made that life harder.
So, I choose to call myself autistic.
I call myself disabled because, to me, it is empowering. As many so-called “high functioning” (another term on the outs) autistic people were once handed the now defunct label of Asperger’s (aka autism-lite), the idea that I may not “seem” disabled or that I am indeed not “truly” disabled has been used against me. It has been used to push me past my limits until I burn out, to convince me I should be able to behave like a neurotypical and fill me with guilt when I do not.
Sometimes, after wondering for so long what is wrong with you, it can be a relief to realize there is something “wrong” with you. That you are not just lazy, clueless, childish, or hysterical. I have a disability. Just because others may not understand the ways in which I struggle does not mean those struggles are not real. Some things are hard for me, even impossible, that may seem trivial to other people. That is okay. There should be no shame in knowing my limitations and refusing to let others push me past them when I know it will not help me. I find power in being able to say, “I am disabled, I need help” just as much as in saying “I can do this on my own”.
And yet there are others on the spectrum who have completely different preferences than me. There are still plenty of self-advocates I encounter regularly who prefer person-first language. They do not want to be defined by their disability, which they feel identity-first does, and balk at being called disabled for similar reasons. A common argument I hear from them is that they want to be seen as “more than my disability” and so resist identifying too strongly with said disability. They are a person, not a diagnosis. They also point to the negative public perception of autism, usually based on the very limited and stereotyped media portrayals of it, as a reason not to want to be called autistic. It can sound more like an insult to them, and indeed some may have experienced the word being thrown in their face that way by ignorant people. For similar reasons, some originally diagnosed with Asperger’s are unwilling to give up the now outdated label for the far more stigmatized autism. At the other extreme, there are those who are enraged by autism being referred to as a disability at all. They maintain that autism is only disabling in a society not built to accommodate it and that calling autistic people disabled only serves to unfairly stigmatize those who simply have a different way of thinking. Similarly, these people may decry overly clinical language when discussing autism. They would undoubtedly object to my using the word “symptoms” in this essay. Their argument is that autism should not be talked about as a disorder or disease, and any language that implies as such is alienating and ableist (i.e. discriminatory against people with disabilities).
Even things one might imagine to be neutral terms have hidden discourse lurking around them. The term neurodiversity is something I have seen used more and more as a catch-all term for conditions like autism and ADHD that can be employed without causing much fuss from any side of the various label debates. And for the most part, this is true. I find it can be a useful term, especially when paired with its counterpart of neurotypical. It makes it easier to discuss how “normal” people think and behave vs. “abnormal” people without using either of those extremely loaded words. It is a way to talk about people who are different without the implication that those differences are bad. However, I feel some discontent around the term when it is used too much in autism support and advocacy spaces. I was surprised some months ago when other self-advocates I was with on a panel discussing that very term felt the same. The shock was mutual all around, all of us assuming we would be the odd one out. In short, the term has become so broad (beginning to encompass almost everything found in the Diagnostic and Statistical Manual (DSM) in some circles) that using it in spaces specifically for autism can feel pointless. Or as if the actual condition being discussed is obscured. It sanitizes autism for those ill at ease with the diagnosis, putting it under the umbrella of a bigger term even when that umbrella is not needed. The consensus that day seemed to be “if you mean autism, say autism”. Even so, I understand why it is so widely used, and I doubt that will change anytime soon. This is only one example. Many times, I have encountered people objecting to terms I think of as neutral or harmless, sometimes even positive. I recently heard objections to the term self-advocate, which I admit left me confused. Especially since the person who initially mentioned those objections to me may have thought these reasons were self-explanatory and so did not offer much follow-up. The moment stuck with me, and I’ve tried to piece together why such a term may be objectionable since. Like many things, I am sure there can be multiple reasons. The one I understand best is perhaps the way in which such a term automatically “outs” the person it is applied to as autistic. I myself have lately started referring to my job simply as “disability advocate” in situations where I would rather avoid the potential ableism self-identification can bring. I have also seen articles and lists attempting to compile the “correct” wording to use for everything related to autism. In them, I see terms facing the axe that I would never have before considered. Things like “special interest” or even the “low/high support needs” terminology I and others have been championing as a replacement for “functioning” labels have their objectors. Honestly, I could likely point to any term or label used or seen and discuss objections raised against it. Fortunately for both of us, I have a page count limit.
Ultimately, there is a futility in attempting to compile an exact list of words that everyone should use to describe the autistic experience. What speaks to one person may alienate another. It can be frustrating for me when it feels like other self-advocates fail to recognize this. I have dealt with another self-advocate brushing off wording I have approved as “stigmatizing” or “ableist” without thought to the fact another autistic person saw those words and was fine with them, or even that I might object to the wording they prefer. I think we would all benefit from learning to articulate “I do not like this wording” or :this wording makes me uncomfortable” without resorting to declaring it ableist and unacceptable in all contexts just to have our concerns taken seriously. There are nuances to be found outside of attempting to exorcise our vocabulary of any and all language that may have problematic implications. Just using the right words will not erase ableist attitudes on their own, or even stop the people using them from being ableist. Ableism takes a far more damaging form in people’s actions and attitudes than it ever can in just their words alone. It is true that the words people use can often betray or influence their attitudes but focusing only on changing their language is merely wallpapering over those attitudes instead of truly challenging them. I am tired of hearing advocacy organizations fret about their image more than they seem to think about their actions. Whenever I hear endless talk about updating logos and banners and whatever other branding to make sure they have an infinity symbol instead of the dreaded puzzle piece or making sure it is “autism acceptance” month now where we must wear red instead of blue, I want to gnash my teeth. “What does it matter?” I want to shout. Oh, I am sure it does matter a lot to many people, don’t get me wrong. They want at least surface-level proof that these organizations recognize that the much-maligned Autism Speaks is not a group to emulate. But I have seen at least one organization do this and yet still entertain discussions about “curing” autism. I would rather see slightly tone-deaf good intentions than the same ableism being covered up with top-notch public relations. I want these organizations to do the hard work of changing their priorities to reflect what the autistic community wants and needs from them before they start worrying about infinity symbols and puzzle pieces.
From all I have written so far, you would probably assume I am driving toward the argument that these language debates are pointless and that we should focus on things more important than trying to police what everyone says. But that is not the whole story, not for me. People who know me and have worked with me have heard me voice my opinions on what words I think should and should not be used. It would be hypocritical of me to pretend otherwise. Though I have tried to go along with and push the attitude of “let people use whatever language feels right to them,” I still find myself chafing against this at times. While it is an important sentiment that I think is ultimately beneficial to autism advocacy discourse, it can be used as a “get out of jail free card” when examining our own biases. It can shut down potential discussions and explorations of internalized ableism, which does not go away if we all pretend it’s not there. Or even just ableism in general, when interrogating why some neurotypicals want to talk about autism in certain ways. There is always value in questioning why we use the words we choose to use. It is an important step towards actually challenging deep-seated ableist attitudes. It is just a question of carving out appropriate times and places to have these discussions, instead of just constantly squabbling with each other over word choices. I will never stop trying to urge people to consider why they feel uncomfortable around certain words while preferring others, and whether their reasons are as black and white as they want to believe.
This goes double for those who are not on the spectrum. Just because I have spent this entire essay arguing that reality is more complicated than choosing between “good” and “bad” words, that does not mean there is no such thing as ableist language. Words can be used in hurtful ways, but the attitude behind those words is even more hurtful. While intra-community discourse is complicated enough, it can admittedly become even uglier when non-autistic voices weigh in. An autistic person not wanting to be referred to as disabled is a different scenario from a neurotypical parent objecting to that word due to their own negative perception of disabilities. And while I think overall it is better to leave squabbles over small language choices at the door when we can, neurotypical advocates are as much responsible for the creation of a healthier discourse around language as any self-advocate. Partially in response to how heated these debates can get, I have seen neurotypical parents and experts become (however unintentionally) outright cruel in their defensiveness when challenged. A big tactic I have seen lately is dismissing the struggles of outspoken self-advocates who argue with them, downplaying their experiences as “not severe enough” to speak on the topic of disability. Even lately pushing the label of “profound autism” which seems designed to separate these (presumed low support need) self-advocates from those on the spectrum who “suffer more” and thus preventing them from being a part of the discussion when it comes to autistic people with very high support needs. Muscling self-advocates out of spaces they belong in is not the answer, however much you disagree with them. This should not be the next step in the language of autism advocacy. We are all capable of treating each other better than this.
There are some who will see this essay as unfair and biased. I cannot deny that it unavoidably is. I can only speak for myself, for my opinions and experiences, which is a big part of the issue I am attempting to tackle here. I have seen more harm than good come when attempts are made to speak broadly for others. Yet that is the whole point of advocacy, isn’t it? There are those unable or unwilling to lend their voice. Or even just uninterested, wanting to live their lives as their own person instead of being forced to represent a greater community. But activism requires some of us to speak, and so we are forced to speak for these unheard people in order to advocate for them. It is an imperfect and messy situation, so the words we use are often doomed to be imperfect and messy. What matters is why we use them, and how they are heard.
Biography
Rachel Guttentag graduated from Temple University with a Bachelor’s in Psychology in early 2019, participating in the first-ever community autism peer specialist (CAPS) training cohort later that year. Currently, she works with the Philadelphia Autism project on their board of advisors and on other projects, hoping to lend her voice and perspective as a self-advocate. Additionally, she works freelance with other organizations and researchers looking for that same voice and perspective. She hopes to complete a Psy.D. program in the future and use her personal experience and academic training combined to help bridge the gap between experts and the greater autism community. You can find more of her writing in her blog posts published by ASDNext.
Contact Information
Rachel Guttentag
Philly Autism Project
Autistic Self-Advocate
ryerguttentag@gmail.comLevine | 31-36
Volume 11 ► Issue 4 ► February 2023
The Importance of Advocacy at State Mental Hospitals
Laurie Barnett Levine
MSW, LSW
Mental health advocacy has existed for decades, even centuries. As long as there has been mental illness, individuals who experienced the illness have been misunderstood and locked away from society. In order to understand the importance of advocacy today, we must understand the history of advocacy and the stigmatization of those with mental illness.
The word “bedlam” that we use today to mean uproar, pandemonium and confusion came from the name of a hospital in London in the 1400s. The hospital, Saint Mary of Bethlehem, was devoted to treating the mentally ill.
According to the National Association for Rights Protection and Advocacy, “mental patients had been subject to torture which included being shackled to walls, put in tanks of ice water, strapped to chairs, over medicated, and even given forced lobotomies.”1 Society did not understand mental illness or the functions of the brain so individuals who had a mental illness were locked away in terrible conditions in what were called insane asylums.
Mental Health America, a national organization with whom my agency is affiliated, was established in 1909 by Clifford W. Beers who had been a patient in mental hospitals. He witnessed and was subjected to horrible abuse which spurred his advocacy and the founding of Mental Health America, the nation’s leading community-based nonprofit dedicated to addressing the needs of those living with mental illness. Clifford Beers wrote the book A Mind That Found Itself.2 At the Mental Health America national headquarters there is a bell the size of a smaller liberty bell that was formed out of shackles that bound mental patients. This bell is rung annually at the national annual meeting and has become part of the logo of that organization.
We have come a long way from the 1400s, 1800s, and 1900s, but we have a long way to go. The word “advocacy” means speaking for another. Advocates today do not speak for the individual. Instead, they help individuals to have a voice. Advocates in the early days were mostly ex-mental patients who sometimes called themselves ex-inmates. These are people who moved from being victims to activists.
In the 1970s, the federal government, through what was then the National Institute of Mental Health, gave grants to the states to involve individuals who had been receiving care to become involved with policy and program development. This began the consumer movement. There are many terms that are used today to define these advocates, the individuals with lived experience. Terms used include Peers, Individuals with Lived Experience, Consumer, Patient Advocate. These individuals are invaluable in the advocacy movement because they stand as a living, breathing example of help, hope and recovery. Today the peer movement is very strong, and peers function as part of the treatment team.
It is now understood that many individuals who have a mental illness can live full, productive, happy, and healthy lives. Individuals may need supports in state mental hospitals when there are no other options, and they require further treatment and additional services to meet their needs. People with mental illness are treated in the least restrictive environment. Mental hospitals are closing beds, and in some cases the hospitals themselves are closing. Individuals who are “patients” are transitioned into the community.
This discussion is a brief synopsis of a very important movement and evolution in treatment and best practices. This is by no means to diminish the role that advocacy has played and the advancements in treatment that have been made. We are constantly learning about the brain and research is steadily continuing. Medications are being invented that improve outcomes and systems of care are improving.
The stigmatization of those with mental illness has not been eradicated and there is much ignorance and misunderstanding concerning individuals with mental illness. There continues to be much shame and blame. This can present many challenges as individuals transition from hospitalization to the community.
There are many challenges that occur when transitioning individuals from the state hospital to the community. The community mental health system has long been underfunded. This results in waiting lists for services, low staff salaries and often not a full complement of services. There is currently often a shortage of programs to send individuals to after hospitalization. This has been exacerbated by the COVID-19 pandemic, which created an increased need for services and a serious shortage of workers. Services have had to be curtailed and, in some cases, programs have had to close, or implementation stalled.
It is understood that an individual’s basic needs must be met in order to be successful in living in the community. The concept of Social Determinants of Health (SOD) has emerged and fulfilling as many of these SODs as possible is considered to be a best practice. According to the World Health Organization, “these are non-medical factors that influence health outcomes. They are conditions in which people are born, grow, work, live, and age, and the wider conditions of daily life.” Examples of the social determinants of health are education, housing, income, food security, and education. As we move forward with advocacy at hospitals, we must make sure that individuals that transition from the hospital to the community have provisions for their SOD. Research has shown that meeting these needs is as important, if not more important, than healthcare. If you do not have a safe place to live, with food to eat, it is very difficult, if not impossible, to focus on your mental health.
There are many positive advocacy endeavors that exist at the hospital in order to assist individuals in transitioning to the community. Hospital discharge discussions can be very stressful and is a big change in the person’s life. One of the important efforts is to teach people in the hospital about self-advocacy. According to Mary Ellen Copeland, “the number one reason for developing self-advocacy is that you are the only person who has to live your life.”1
Advocates have met with state hospital patients and reviewed a self-advocacy curriculum. The advocate, the patient, and hospital staff work together to develop a realistic discharge plan and access community resources. Preparation for discharge must begin while the individual is in the hospital so that the social determinants can be in place and the individual can seamlessly transition to the community.
Peers have also become involved in assisting individuals in being ready for discharge. They offer inspiration and support in what can be a very anxiety producing situation. The person being discharged must be a part of the planning process for discharge. As Copeland states, “it is their life after all.”1
We have made many strides from the days when patients were shackled. We must continue to learn about what assists individuals to transition successfully to the community, apply best practices, to nurture resiliency and to achieve recovery and improve wellness. The hospital advocates have an important role in this transition process, helping to achieve a successful hospital discharge.
References
1. Copeland, M.E. The National Mental Health Consumers’ Self-help Clearinghouse. “Self-Advocacy.” https://www.mhselfhelp.org/. Accessed February 6, 2023.
2. Beers, C.W. A Mind That Found Itself: A Memoir of Madness and Recovery. Waking Lion Press; 2008.
Biography
Laurie Barnett Levine is the Chief Executive Officer of Mental Health America of Southwestern PA. She holds a master’s degree in Social Work from the University of Pittsburgh and is a licensed social worker. Laurie has been a passionate advocate working to improve the lives of those impacted by mental illness. She has spent decades working in the behavioral health field promoting recovery, early detection, education, and quality services and programs for those with mental health issues. Laurie has supported the education of mental health professionals by working as a field instructor and adjunct professor for several colleges and universities. Laurie is a member of the Public Policy Committee of Mental Health America national, serves on the Public Policy Committee of the Greater Pittsburgh Nonprofit Partnership, President Elect of the Mental Health Association in PA, Allegheny County Mental Health, and Intellectual Disabilities Advisory Committee member and is Vice Chair of the Ray of Hope Suicide Awareness and Prevention Task Force of Westmoreland County.
Contact Information
Laurie Barnett Levine
Mental Health America of Southwestern PA
Chief Executive Officer
lblevine@mhaswpa.org
Marti, Malone, Knauss | 37-59
Volume 11 ► Issue 4 ► February 2023
From Infants to Adults: How Two Mothers Have Advocated for Their Sons with Autism
Introduction written by David Knauss
Articles written by Kathrin Marti and Melissa Malone
Family is the foundation of life in the United States. When a family member advocates for an individual with autism, an intellectual disability (ID), or a mental illness, a great deal of good can come out of it. The motivation to help a loved one is borne out of several things: outcomes affect the entire family, the entire process of helping can make the family closer, the concern about the cost of care, and, most importantly, the deep love for the family member. There is a lot at stake. The following is a two-part article that shows how two dedicated mothers have spent many years advocating for their sons. The first article is by a mother of two sons with autism, ages 26 and 25. The second article is by a mother of a son with autism, age 32. This second parent is also the legal guardian of a young man with Down syndrome, and has fostered two other boys: a teen-aged boy with bipolar and attention deficit hyperactivity disorder (ADHD), and another boy with ADHD.
How I have Been an Advocate for My Sons with Autism
Kathrin Marti
My name is Kathrin Marti, and this article is about how I have been an advocate for my sons, Christopher, aged 26, and Kieran, aged 25. Both of them have autism.
Pizza ,spaghetti, and meatballs are regular items on the menu at our house in Lebanon County, PA. Using premade frozen dough, Kieran has learned to make a delicious pizza, with unlimited toppings, the likes of which would rival any pizza shop that I know of, and Chris can roll the perfect meatball using ground beef, an egg, and some breadcrumbs. Like mothers the whole world over, we aim to teach our children to become as independent as possible, and to navigate the adult world when we are not around to help them. When your child has a disability such as autism, that can be a challenge, but we, being the warrior mothers that we are, do not give up. Preparing food for each other is one small facet of that process.
Both of my sons were born in different states, and I was born and raised in a different country. The relevance of this fact is that I have no cultural frame of reference for many things that are known by most of the people who grew up here and have family connections here. So not only was the experience of having children with special needs a challenge it was also, for me, quite literally, foreign.
My firstborn, Chris, was born in 1996 in Massachusetts and was six weeks premature. As a first-time mother, with little experience of babies and a long way from family, it was a rough start. Chris spent time in the neonatal intensive care unit (NICU) and when he came home after six weeks, he was a very challenging infant, and then a difficult child. His dad, a US Marine Recruiter, had to work long hours and was unable to be around often. My occupational therapist brain now recognizes the sensory overload and discomfort I was experiencing, but at the time, I just felt incompetent because I could not settle him or make Chris happy. Being diagnosed with congenital hypothyroidism at three days old meant that he had to take thyroxine, and his dose was high, which probably contributed to his agitation. I tried speaking to his doctors about his constant agitation and screaming, but my concerns were mostly ignored or placated.
My work was cut out for me. Over those first few months I lost so much confidence in myself as a woman, let alone a mother, and sought to educate myself by devouring every bit of information, from other mothers and from experts, that I could find for ways to help him. Most of it was unhelpful, and it was only once I started listening to my instincts and ignoring the well-meaning advice of others, most of whom had typically developing babies and children, that we became more connected, and Chris’ condition started to improve. The revolving door of Early Intervention therapists were supportive, and I was grateful for their input and suggestions, but there were times that I just wanted us to be left alone. It took this growth in my confidence to know that I also had the power to advocate for a break or to simply just cancel a previously scheduled appointment because we just needed to rest.
Later that year, we moved to the Pittsburgh area, and eventually, we were able to buy our first home and finally settle down. Not long after that I got pregnant with my second son, Kieran.
In terms of advocacy, I gained confidence once I trusted myself, and was able to speak more clearly and definitively about how Chris was really doing and what he/we needed. We continued to receive support from the Intermediate Unit (IU) with Early Intervention, and when Kieran was born in 1997, we joined other support groups, such as the church, Mothers of Preschoolers (MOPS) and La Leche League and became part of the community. Kieran’s birth, happily, was typical in such a contrast to Chris’. When Chris turned three, he was discharged from direct IU services, just retained consultation for his developmental delays. We noticed a steep decline in his functioning that year, as did his doctors. We advocated for more supports and services but were denied. I felt like I was continually having to go into battle and fight for him which was very draining.
Making progress at the IU preschool
Finally, after a regular observation visit at his church preschool, the IU teacher called me and told me of her concerns about Chris. She said that he had been at that preschool for 18 months and still did not know a single child’s name. She asked if it would be okay for him to begin attending the IU preschool a couple of afternoons a week. Okay!! - I was delighted and it finally felt like I was being heard! He started later that week and the progress that he made in the right environment, with the right supports, was tremendous. When it came time to register him for kindergarten, I refused to send him -- he was making great progress at the IU preschool and I wanted to provide him the gift of time, and for the district to pay for him to continue there. I had anticipated a fight, like so often before, but they agreed. It was without doubt the best decision to retain him. That felt like a huge win.
Whilst all this was going on, Kieran was developing well. His vocabulary was extensive, and he was intelligent and inquisitive. Even though there were 21 months between them, they were developmentally almost at the same level, including for things like potty training. We were fortunate that we could rely on some marvelous teenage babysitters in our neighborhood who were both understanding and capable. We had no family close by and by Kieran’s first birthday, both of my parents had died.
In 2001, their dad retired from the Marine Corps, and we moved to West Virginia soon after. Both boys went to regular kindergarten and preschool. Chris received some speech therapy but that was it. Kieran attended a wonderful small church preschool, where his “quirkiness” (he was in his Blue Phase in which his clothes, for example, had to be the color blue) was accepted and he flourished. He learned to read in preschool and seemed to be doing well. When Kieran started having problems at school, his teachers asked permission to evaluate him and it came as a shock to learn that he had been diagnosed with Asperger’s syndrome, a form of autism. I knew that he was “different” but thought it was because he was so bright. Having one child with special needs was rough, but two?? For a while I thought that God hated us. The fact that he would read dictionaries in first grade and would just walk around the perimeter of the playground every day instead of playing with the other children should have sent alarm bells ringing, but we thought that it was because he was just so bright and was bored.
We tried to involve both Chris and Kieran in typical childhood activities such as sports, Sunday school, and Cub Scouts, but it was always difficult. Their father became the Cub Scoutmaster and T-Ball coach so that he could be there for them and support them, but they still struggled.
School was becoming more and more of a challenge for both boys. By first grade, Kieran was already refusing to go and was deeply unhappy. There were constant Individualized Education Program (IEP) meetings and we -- both Mike, my then-husband, and I -- felt like we were trying so hard and getting nowhere fast. In first grade, Kieran was evaluated for the Gifted Program, and for a while he was appeased with that as he enjoyed the lessons, but his behaviors were becoming more challenging. I advocated for Kieran to skip second grade, as he was already reading at a fourth- or fifth-grade level. The school was hesitant at first but permitted it. From third grade on, both boys were in the same grade, despite their age difference. That year, their father gained a promotion and he moved to Lancaster County, Pennsylvania, whilst I stayed in West Virginia so that they could finish out their school year.
Finding more support in Pennsylvania
When we all moved into our house in Lancaster County, I can recall feeling positive about the opportunities for support that presented themselves -- so much more than was available to us in West Virginia. Kieran was assigned a 1:1 aide, which he continued to have from fourth grade until twelfth grade, but the district refused to assign one to Chris, whose behaviors were much more challenging. With the support of a 1:1 aide, Kieran was able to participate in the regular curriculum successfully for the most part, but I spent many hours around the IEP table for Chris. Eventually, he was reevaluated, and was finally diagnosed with autism spectrum disorder (ASD).
Chris’ receiving the diagnosis of ASD was a shock, but it finally made sense, and it meant that valuable supports such as Medical Assistance were activated, a benefit which has been worth its weight in gold. He also qualified for therapeutic staff supports(TSS), and behavioral supports. We found a psychiatrist who ended up working with us for many years, and the boys each received counseling and were prescribed medication. With all this upheaval, I confess that I was often overwhelmed and quite depressed, and sadly, it was at this time that their father found solace elsewhere and left the family, which added another tier of stress onto an already difficult situation.
I became accustomed to IEP meetings where I was on one side of the table and ten teachers or staff members were on the other. Having to listen to the litany of difficulties that both boys (but mostly Chris) were experiencing was so hard. A plan would be made, but invariably it would fail.
I got to know their special education teachers well and felt that they were kind and supportive. The assistant principal at their high school took a special interest in Chris, and even kept a packet of hot dogs in her fridge for him for when he found the school lunch choices unappetizing, as by that time he had also been diagnosed with type 1 diabetes too, and so food became an issue.
Eventually they both graduated from high school, and Kieran, having earned an excellent SAT score (2040), achieved a scholarship to Albright College. Chris went to Hiram G Andrews (HGA) school in Johnstown, Pennsylvania. Life seemed positive and exciting.
Everything changed when Kieran entered his third year at Albright. He was living with his father and commuting to college on the bus. Both of us tried to encourage Kieran to advocate for himself at college to access tutoring services and supports, but unfortunately, he would avoid asking for assistance or simply not show up when arrangements had been made. He had success with his general education classes, but Albright steers students toward a professional major in their third year. He was (and still is) unsure of what career path to choose, so I encouraged him to take accounting courses, believing that would suit his personality and aptitude. Big mistake -- he hated his classes and did not do the work, failing them, and eventually losing his scholarship.
Navigating the world of work
Kieran dropped out of college four years ago and it has been an extremely difficult recovery since then. His anxiety and depression have increased considerably and there have been times when it has been difficult to rouse him out of bed. He has really withdrawn, and it has been difficult to get him to apply for jobs. Unfortunately, even when he applies for positions for which he is more than qualified, he cannot get beyond the interview stage because employers find his speech difficult to understand (his stuttering has increased tenfold) and his responses/demeanor during the interview are awkward to say the least. Kieran faces so much prejudice and, as a mother, it is heartbreaking to witness. I have advocated for him to receive speech therapy and interview practice but unfortunately the business world is less than accommodating for people like him.
Chris was at HGA for almost a year, but that did not work out either. We tried to support him by visiting as often as possible, but with me working full-time and the three-hour drive each way it was very difficult. His father and I both tried to set him up for success and advocate for him to get the supports that he needed. Sometimes this worked and sometimes it did not. He was seeing the counselor daily and making his own appointments to get his medication, but ultimately, it was not enough.
Chris has tried to secure different types of employment since he returned after dropping out of college, but sadly, none have panned out. We have encouraged him to self-advocate by speaking to his supervisors about both his diabetes and autism conditions whenever possible and advising them to ask for accommodations where necessary, including having access to insulin and testing supplies, or a visual checklist of tasks to be done.
In 2022, both Chris and Kieran worked at a warehouse facility in Lebanon County, Pennsylvania, and were also able to take advantage of the job coaches, which were paid for by the Office of Vocational Rehabilitation (OVR). The Lebanon Youth Program, operated by the Lancaster-Lebanon IU, assisted with placing Kieran in that job. The job coaching did help, but unfortunately, neither Chris nor Kieran were happy there and they resigned.
Navigating the adult world for an individual with autism is remarkably difficult. Whilst at school, there are supports that can be put into place and it feels like there is a team to support you, both as an individual and as a family. However, once you have graduated, it is a very different story. We can only speak from our experience, and it has been chaotic to say the least in the last few years. One of the problems that we have faced is that both Chris and Kieran have been denied any kind of Social Security disability benefits and so have no financial support whatsoever beyond what I (and sporadically their father) contribute. It is as if they are deemed too disabled to work by the business community and not disabled enough by Social Security. Another problem that I have faced is that I do not really know what supports are out there and how to access them. There is an alphabet soup of agencies (OVR, ODD, etc.) and I have found that in order to meaningfully advocate for your adult children with autism, you really have to be that squeaky wheel. You need to reach out to as many contacts, preferably who have walked this walk before, as you can and keep on pushing. We recently re-engaged OVR to help Kieran and Chris gain employment supports and education. The pandemic did not help, but I will not give up until both Chris and Kieran have found functional, worthwhile employment where they can be part of the world, just like everyone else. One bright spot was that Kieran recently obtained his driving license, which was fantastic.
In conclusion, I would say that if you have a child with a disability such as autism, it very often feels like you are on the outside looking in and it can be very isolating. It is tempting to give up, and frankly, I think that there are many people in
our situation who would have, but do not. Keep fighting! We are warriors, and we will blaze a path to make it easier for others in the future, but for right now, find your tribe, be it a support group, church, family or whatever, put your armor on
and go into battle for your child because both you and they deserve nothing less.
An Advocating Journey
Melissa Malone
Advocating for family members with special needs is a topic that is very special to me. I have been an advocate for both my 32-year-old son Mike, who has had autism since he was born, and for a boy with Down syndrome who is now, at age 25, a member of our family. Additionally, I was blessed with the opportunity to advocate for a teenage boy with bipolar disorder and attention deficit hyperactivity disorder (ADHD) who lived with us for one year. And I was a foster mother for another ADHD child who lived with us for nine years. The following is my story.
After four years of marriage, Michael William Malone was born in May 1990 to Melissa and Shawn Malone. Blessed with our bundle of joy, a new home purchase in Montgomery County, Pennsylvania, and career jobs, time flew by quickly. The first two years we attended to Mike's medical needs of a left club foot correction and hearing issues due to acute ear infections. By the age of two, it was evident Mike had some developmental delays of speech, fine motor skills, physical mobility skills, attention, and socialization. Since his birth I fortunately scaled back with my job and settled into a part-time human resource position from my full-time job. Because of his delays, Mike's pediatrician prompted us to get him tested with the Intermediate Unit in our area. He did qualify for Early Intervention services and attended a learning center daycare program three days a week at two and a half years of age. Mike started to make better progress; however, his teachers informed us that Mike had extreme attention issues. He was disruptive during circle time, always getting up. Instead of walking around his peers while they played with toys on the floor, he would unconsciously walk through the toys. There was talk that Mike could benefit from a one-on-one aide, but the question was how to make this happen when the initial request of the service was denied.
Luckily, the learning center advertised a weekend conference for parents with special needs children. I cannot remember what agency sponsored the event, but Shawn and I jumped on the chance to apply for a scholarship and were accepted. This was our first chance to seriously network with other parents. What a beautiful event! Meeting those other parents was so exciting, but almost embarrassing when asked “what diagnosis does your child have?” It gave me a reality check of what some parents faced medically and emotionally when they shared their children's stories of cerebral palsy, blindness, deafness, muscular dystrophy, epilepsy, etc. When I said we have a corrected club-footed, hyperactive, developmentally delayed child, I just felt like we were unqualified to be at this type of conference. However, with the wealth of knowledge and friendships formed, it made a huge difference in our lives to know we were not out there by ourselves! We attended the same conference a year later as well.
At the initial special needs conference we attended, one advocate kept coming up as an excellent resource, free of charge, so we contacted him to see if he could help us advocate for Mike to get a personal care aide in Early Intervention. Upon meeting him he shared he had a law background, although he was not officially a lawyer. He traveled across Pennsylvania helping families with advocating. He had a special needs child himself, so what could go wrong? After briefing him on specifics, I had him attend our child’s Individualized Family Service Plan (IFSP) meeting. It was unexpected when he came on like a bulldog, giving the Intermediate Unit an ultimatum. Oh my, I almost freaked out then and there and he was on my side! The teacher was crying, and I was so nervous I literally ripped my nylons I was wearing. I asked him afterwards if that was necessary to come on that strong and he told me, YES as he did not have time to loop around for second rounds. It was not my style of communicating, but it worked. Mike had a personal care aide.
When Mike was three years old, I changed my work field to part-time banking which helped me concentrate on Mike’s developmental milestones. My working hours were coordinated with his preschool hours. It worked out nicely to concentrate on his speech, behavior, and hyperactivity.
In 1994, when Mike was four years old, talks ensued from my family if we would consider moving back to Lebanon County to occupy a family homestead residence. Wow, what a question! We only owned our Montgomery County home for four years. Could we swing this? Shawn’s career was based out of Philadelphia, but it would be nice to have family support close by. Could he swing it? His answer was yes, so the house was sold and on the way we went.
Mike starts public school
At the age of five, Mike was starting kindergarten in Lebanon County. He had an Individualized Education Plan (IEP), so again I said, what could go wrong? Well, the special education director of our school district at that time announced to us they do not provide individualized speech therapy, even though it was listed on his IEP, and he would need to use classroom aides. Now what?! Was I going to call our previous bulldog advocate or try to handle this myself? The speech therapist at the time agreed with me, that Mike’s attention span was really impaired, but he wanted to tread carefully with this situation. So, with his help collaborating with me about the facts of Mike’s case, the school system finally supported it. This should have never been an issue since an IEP was a legal document. When I asked what was the problem that this was an issue, I was told, “parents are not really involved around here, they just go with the flow. You deciding to advocate for your child not only rocked the boat but sunk it.” OK, that was surprising information.
Also at age five, Mike was officially diagnosed with attention deficit disorder (ADD). The evaluator said she did not usually put a label on children that young, but when Mike wrapped himself up like a hot dog with a hospital room divider curtain, she felt that that, and other history, was enough to warrant the diagnosis.
Between the ages of five and seven, Mike began to have more pronounced behaviors of stimming -- whirling, twirling, humming, rocking back and forth, and hand gesturing. He also was very pervasive with his thoughts. After we sought out another well-known developmental specialist in our area, he then was diagnosed with pervasive developmental disorder (PDD). I still remember the doctor after evaluating him for a half day stating, “This was an easy one. He talked about Goosebumps books while traveling up the elevator, down the elevator, and fit it in on every opportunity throughout the evaluation.” At this point we did pursue medication management to aid Mike with his impulsiveness, short attention span and hyperactivity. In elementary school, supports were going strong. We had supportive teachers who I handpicked to best suit the needs of Mike. I think with me being so involved with tutoring him, the principal and special education director gave me that privilege.
Community support in Lebanon County was good. When Mike was five, I joined the Children and Adults with Attention Deficit Disorder (CHADD) group in our area. What a pleasure to meet other parents with children of similar needs. I eventually became a co-leader in CHADD and attended National CHADD conferences to educate ourselves and others. I just loved the support and being able to support others. It really made a difference in our lives.
In 2000 after working a part-time job as an accounts receivable analyst for two years, I was blessed to find out our area was training bachelor’s degree graduates (like myself) to substitute teach in our area. It was the perfect part-time job for me! I was sure it would be a good fit, even though I was a business major. Tutoring Mike so heavily throughout his school career, I knew I would love teaching. The flexibility of scheduling and summers off, who could beat that?! Again, I learned so much from this job and really had a fond heart for children with disabilities. Specialized classes of life skills, learning support, behavior support, and autism support were my favorites. I felt I understood these children.
With us being back in my hometown in Lebanon County, our family got to know Mike better. In general, our family and friends were accepting of Mike; however, my ex-Marine Corps father had more difficulty. When Mike was small, Grandpa had a hard time accepting his autistic behaviors. We had a behavioral specialist talk with him. He told her, “A good slap on the butt would correct the problem, and she (myself) just did not know how to properly parent Mike.” My dad’s relationship with Mike failed to bloom to its full potential. My father died when Mike was 14.
I initially feared Mike attending middle school. How was this all going to work with a different teacher for each subject and the increasing academic demand? Upon meeting the learning support teacher, I was relieved. She was the master coordinator of all and wow, did she do it well. Mike’s aide scribed notes for him in class when he could not keep up, and the learning support teacher manufactured study guides and adapted tests that were mostly multiple choice and true/false, limiting the amount of essay questions. The only time Mike had to use the learning support classroom was for testing. It was a dream come true! Inclusion was again working well for Mike.
We had a similar experience with high school. That learning support teacher was the principal’s wife, and we had the inside track when we hit any bumps in the road with teachers. During Mike’s senior year, he was able to secure his first part-time employment with Service Source, at Fort Indiantown Gap National Guard Base. The government had an AbilityOne Program contract (from the U.S. AbilityOne Commission, an independent federal agency) to hire personnel with special needs. Mike was fortunate to secure this job as a dishwasher and performed this job as part of his afternoon high school curriculum. (Mike still works there today, one day a month.) I felt so blessed! Life was good. There was minimal friction all around.
Embracing more children with special needs
A call from a high school friend changed all of that. Her youngest boy, aged 16, was self-destructing in the Florida school system. He was being held back for a third year and was quite distraught. After talking to Shawn, we decided to offer to take guardianship of him for a year and have him fly to Pennsylvania to live with us. He was diagnosed with bipolar disorder on top of his ADHD diagnosis. He received proper medication management, counseling to address trauma as a youth, and heavy learning support through an adapted IEP. Unfortunately, his biological father decided to take him to a different state the next year and he did not fare as well. But I felt satisfied that we gave him a good foundation to build upon. The lesson learned was, passing the ball to others does not always work out as expected.
We were not done helping children. The next year a friend of ours asked us to get involved in foster care. We took in a seven-year-old child with ADHD and a learning disability and a non-verbal nine-year-old child with Down syndrome. We had them both for a five-year period under foster care.
With the child with Down syndrome, we took a Subsidized Permanent Legal Custody agreement when his mother, who had four other special needs children and could not take him back and asked us to please keep him. When this child turned 21, I took permanent guardianship of him; he lives with us today and is part of our family.
The child with ADHD was scheduled to go up for adoption. Shawn was adamant he did not want to legally adopt either child. Then, one day Shawn asked me if I was going to put the Down syndrome teenager in a group home when he turned 18. I was devastated and responded, no. Shawn explained he was eligible for early retirement and wanted to travel and did not want the younger set of kids to weigh us down. I promised him that would not happen, but that apparently was not a good enough answer. That summer after I took the younger children to Florida, Shawn let me know he was having serious heart-related symptoms and needed a lot of testing completed. His mood turned to the worse and I felt helpless in this situation. After three mini vacations that summer, Shawn announced he needed to leave us and he got an apartment by himself, in order to “find himself.” I was devastated. Being married for 22 years at that point, this crushed me, but what was I going to do?
Mike graduated from high school and went off to live at a technical school for adults with disabilities. After about a month of classes, Shawn visited, and a special friend joined them for supper. Mike freaked out when he realized this was not just a friend. Mike called from school to tell me about the situation. Within two days I got a call from the school letting me know our son was mentally unstable and I needed to pick him up and get him evaluated. When a cousin and I arrived, Mike was pacing back and forth saying he did not want to live. I coaxed him to the car, as the cousin loaded up his personal belongings. I felt beyond devastated. I can even feel those emotions of that day flooding back in me writing this. How could everything we worked so hard for with Mike come crashing down?
Now I had to switch my brain into pure survival mode. The younger children were now 11 and 12. Through a lot of tears and prayers we made it to the other side. The child with ADHD got adopted by a college professor and public relations director. I was so nervous about this, but felt I needed to let this happen for his best interests. They were gracious enough to make an informal deal with me that I could still see my lad, one weekend a month, a couple weeks over the summer and part of Christmas vacation. I was ecstatic I could still be in his life. From the ages of 18 to 21, due to his wayward actions in a bigger city, he did come back to live with me full-time. He graduated from high school in Lebanon County with his IEP accommodations. The adopted parents were very supportive, and it all worked out for everyone.
It was determined it was best for Mike to not return to trade school, especially with his first-choice study of bookkeeping being discontinued. He really did not want any other curriculum. Shawn asked for a divorce and was loosely connected to Mike moving forward.
Nevertheless, life was getting better for Mike. A year earlier, at around 20 years of age, Mike had applied for the Pennsylvania Adult Autism Waiver. At age 21, bingo, fate was on his side. A slot opened and he immediately enrolled. This Waiver was a lifesaver for me, being a single parent. Mike had so many opportunities to advance his job skills, communication skills, and social skills. The agencies we signed up with were both very good. They provided community support services to assist Mike one on one. One agency handled behavioral support, and this helped Mike, who was having a lot of picking-his-skin tendencies. The other handled community support and skill building.
Assisted by this Autism Waiver support, Mike was gearing up for further exploration of the work force. His goal – to get an office worker job. From 2013 to 2017, he journeyed through a succession of six jobs – one of them as a volunteer – while continuing to work part-time as a dishwasher at Fort Indiantown Gap. Here are the jobs that Mike worked at:
- In 2013, Mike secured a janitorial job at our local PA CareerLink, benefitting from a contract that the Pennsylvania Office of Vocational Rehabilitation (OVR) had with a job search and training agency. He got job coaching from community inclusion workers through the Autism Waiver.
- In 2015, Mike got a tax preparer position at H&R Block. He got the job following attendance at a tax preparation class, where a CSS worker always joined him. Mike held this job for one year.
- Also in 2015, Mike was a volunteer with Volunteer Income Tax Assistance (VITA) doing simple returns. He worked there for three years.
- In 2017, through OVR, Mike nailed down an internship with Project Search, with Dauphin County as the participant, working at three locations successively – Department of Human Services, Department of Clerk of Clerk of Courts, and a local magisterial judge’s office.
- From this internship, Mike then secured a job as a driver’s license associate at the PA Department of Transportation, Bureau of Motor Vehicles, in Harrisburg, PA. He stayed there only briefly due to a consensus that he needed more customer service experience to succeed. Otherwise, he had the necessary skills to do the job.
- In 2017, the same internship program then helped Mike secure a job with Goodwill in Lemoyne, Pennsylvania., to gain customer service experience. Soon, Mike transferred to our local Lebanon County Goodwill, where he works as a cashier today.
All in all, lessons learned from 32 years life experience of raising and advocating for a special needs child are:
1. Surround yourself with a strong network of support. This may entail family, friends, and support groups.
2. Get evaluations to pinpoint your child’s disabilities and set into motion therapies needed – speech, physical, occupational, behavioral therapy, etc.
3. Apply for appropriate funding – Social Security Income and waivers if your child qualifies.
4. Get yourself educated about your child’s disability. You can do this through books, videos, conferences, and support groups.
5. Check to see if counseling or medication management would benefit your child.
6. Always be respectful and kind to your resources. Mike came a long way by good people willing to help him out.
7. Never give up and when you find successful avenues, share with others, and help them out of the rabbit hole.
Conclusion
The two articles above provide much insight into the great amount of time and effort needed by a parent to advocate for a child with autism. The two mothers, Kathrin Marti and Melissa Malone, give us a window into the challenges, successes, emotional toll, and lessons learned they’ve experienced in their journey of helping their sons. These stories are written within the very important context of family. Their separate articles are long and worth reading; they are written from the heart.
Biography
Kathrin Marti was born and raised in Liverpool, England. She worked as a teacher before meeting her (now ex) husband in Berlin, Germany, who was a U.S. Marine. She moved to the U.S. with him in 1992 and lived in North Carolina, Massachusetts, West Virginia, and Pennsylvania. Kathrin had two sons, Christopher in 1996 and Kieran in 1997, and was a stay-at-home mother for a number of years. Her oldest child had some health issues from birth, was involved in Early Intervention, and continued with therapies and special education. But her second son did not exhibit concerning behaviors until he started school. Both boys are now diagnosed with autism spectrum disorder. Kathrin and her family moved back to PA in 2006. She became a single mom in 2008 and went back to college to get an occupational therapy associates degree to support herself and her children. Her sons are now 27 and 25, really struggling to find their place in this world.
Melissa Malone was born in 1961 and raised in Lebanon County, PA. She graduated from Elizabethtown College in 1983 with a bachelor’s degree in business administration--marketing and management concentrations. She moved to Montgomery County, PA, and pursued management positions in retail management. Melissa married in 1986, and in 1990 they bought their first home and had their son, Michael. In 1994 they returned to Lebanon County, still actively advocating for Mike's special needs. In 2000 Melissa became a substitute teacher in Lebanon County. She and her husband became foster parents in 2004. She separated from her husband in 2008 and eventually got divorced. Melissa is still doing foster care and currently has one placement.
Dave Knauss is retired following a career of 29 years in Pennsylvania State Government. He served as an Income Maintenance Caseworker for 12 years at the Berks County Assistance Office. He also served as a Human Services Program
Specialist doing policy work at the Office of Medical Assistance Programs and doing quality assurance work at the Office of Long-Term Living. His career also includes ten years as a reporter and editor at three newspaper organizations in central Pennsylvania.
He has a Bachelor of Arts degree in American Studies from Dickinson College. From 2007 to 2019 he served as the volunteer leader of a support group for adults with ASD, Spectrum Friends of Lebanon County. He was diagnosed with Asperger Syndrome in
2003. While his ASD is just a small part of his identity, he believes his ASD is a gift.
Contact Information
Kathrin Marti
COTA/L or Certified Occupational Therapy Assistance, school based
Melissa Malone
Foster Parent
Dave Knauss
dcharlesknauss@gmail.com