Positive Approaches Journal, Volume 12, Issue 1
| Site: | My ODP |
| Course: | My ODP |
| Book: | Positive Approaches Journal, Volume 12, Issue 1 |
| Printed by: | |
| Date: | Tuesday, July 14, 2026, 3:11 PM |
Positive Approaches Journal | 6-7

Volume 12 ► Issue 1 ► May 2023
Confronting Stigma and Promoting Wellness: Changing the Conversation
Introduction
In 1963, Erving Goffman described stigma as referring to “an attribute that is deeply discrediting” which serves to reduce an individual “from a whole person to a tainted, discounted one.” Though much has changed in the description and understanding of stigma in the 60 years that have followed, the underlying idea that stigma has a deep and devaluing effect on an individual persists.
Much of the early work examining stigma and its effects has been focused on the field of mental health. In more recent decades, increased attention has been paid to the role of stigma in the lives of individuals with intellectual and developmental disabilities and autism. This recognition has gone hand in hand with the increasing emphasis of person-centered approaches and the fundamental pursuit of Everyday Lives.
This issue of the Positive Approaches Journal is dedicated to a scholarly exploration of stigma through many points of view. Ranging from a broad vantage point of mental health stigma across ethnic minorities to a case study highlighting the impact on individual with stigma in recognized and address, our authors share their experience and expertise on this most important topic. Though quite diverse in background and focus, the contributors here all share in the recognition of the importance of lived experience when characterizing stigma, acknowledging the depth of impact, and designing support and treatment opportunities. A less-often discussed but tremendously important topic, self-stigma is addressed in this issue as well.
It is likely that in another 60 years from now, stigma will remain a topic of great societal importance. It seems, however, equally likely that with continued effort to recognize and address the presence and impact of the role of stigma in our own lives and the lives of others, great gains in creating a more accepting and welcoming world are achievable.
The editorial board of the Positive Approaches Journal looks forward to your feedback.
Gregory Cherpes MD,
NADD-CC
Medical Director
Office of Developmental
Programs
References
E. Goffman, Stigma: Notes on the management of spoiled identity, (1963)Positive Approaches Journal | 8-13
Volume 12 ► Issue 1 ► May 2023
Data Discoveries
The goal of Data Discoveries is to present useful data using new methods and platforms that can be customized.
Autism stigma refers to negative attitudes, beliefs, and stereotypes that society, in many contexts, holds about individuals.1 This stigma can lead to discrimination, social exclusion, and a lack of access to resources and support for people on the autism spectrum.2 The stigma that people experience may also prevent autistic individuals from being hired or promoted, despite their qualifications and skills. People may perceive autistic individuals as less competent, less reliable, and less able to interact with customers or colleagues.1 This stigma can potentially lead to discriminatory practices like not providing accommodations, refusing to hire or promote with the organization, or even terminating employment. 3 Individuals also may fear seeking accommodations for fear of facing stigma.3
Disclosing an autism diagnosis in the workplace is a personal decision that should be carefully considered by individuals on the autism spectrum that has both positives and potential negatives. Disclosure can help employers provide accommodations and support to ensure that the individual can work to their full potential. It can also help raise awareness and reduce the stigma surrounding autism in the workplace. However, disclosing a diagnosis can also lead to negative consequences such as discrimination, exclusion, and reduced opportunities for career advancement.4 It is important to weigh the potential benefits and risks before deciding to disclose a disability. It may be helpful to consult with a trusted advisor, like a job coach, career counselor, friend, or other supporter, to discuss the potential implications and determine the best course of action.
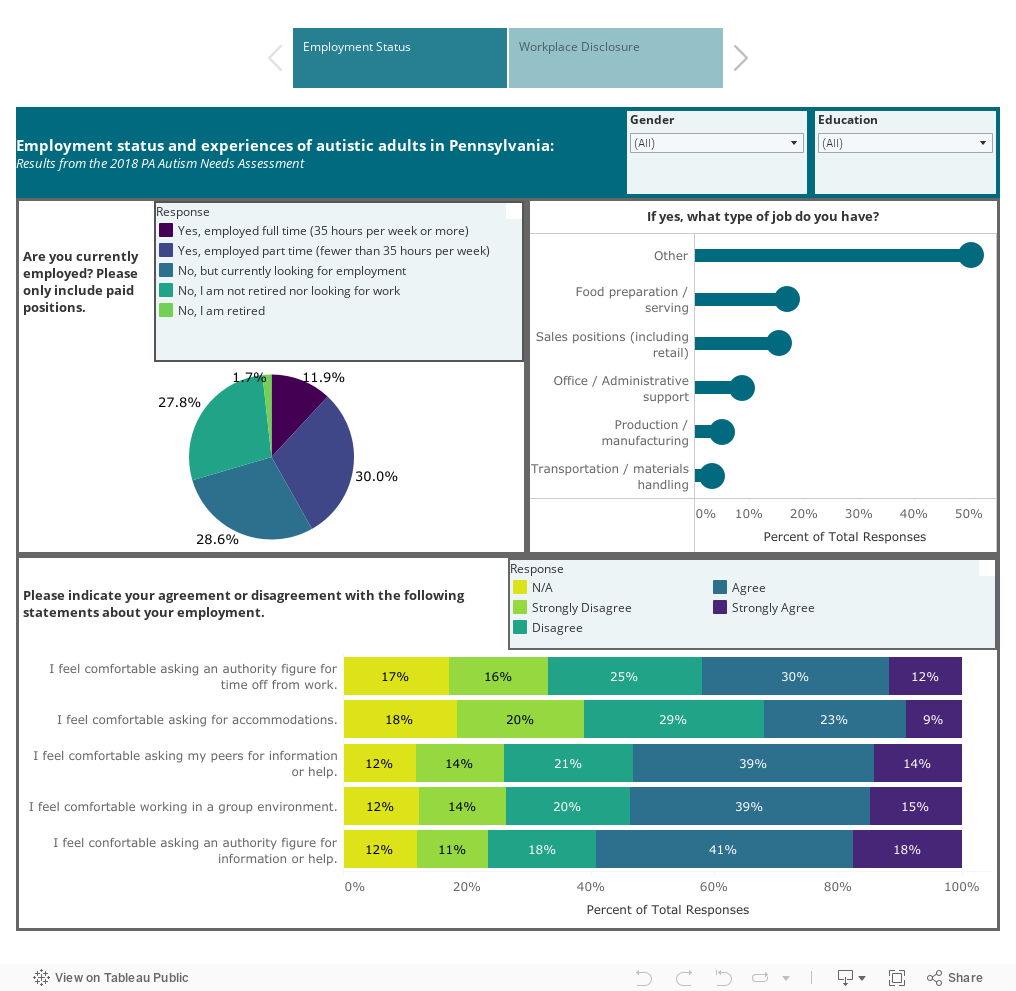
The Autism Services, Education, Resources, & Training Collaborative (ASERT) conducted the 2018 Pennsylvania Autism Needs Assessment (2018 PANA), a large survey of autistic individual and their family members in Pennsylvania. More than 8,000 people completed the 2018 PANA providing information about demographic, clinical characteristics, and other service experiences. For more information about the 2018 PANA and to view more data, visit: www.paautism.org/needsassessment. For the purposes of this data dashboard, only responses related to self-advocacy group participation from autistic adults over the age of 18 were included. In this sample, 41.2% indicated that they work in some capacity for pay, either full or part time. While most respondents generally respondent positively to their comfort level in seeking workplace supports, it is notable that many respondents (49%) indicated discomfort in seeking accommodations. Additionally, only 18% of respondents reported that everyone in their workplace knows about their autism diagnosis. Visit the dashboard below to learn more about this and other data points about autism and workplace disclosure.
The data dashboard below shows responses to the 2018 PANA questions about employment status and workplace disclosure. The first tab shows a visualizations of employment status, type of occupation, and comfort level with different aspects of the workplace. The second tab shows responses to a question about autism disclosure in the workplace and reasons for this decision. There are filters on both tabs to explore the data by gender and education level.
Conclusion
The Autism Services, Education, Resources, and Training Collaborative (ASERT) offers resources relevant to employment among individuals on the autism spectrum and with other IDDs. This includes the Employment Resource Collection which has a compilation of links focused on various aspects of employment and supports and #ASDNext Work Resources which are curated with a focus on transition age youth and young adults. ASERT also has resources related to disclosing an autism diagnosis in the workplace including The 411 on Disability Disclosure: A Workbook for Youth with Disabilities. Finally, ASERT has resource related to getting supports and accommodations in the workplace.
References
1. Botha M, Dibb B, Frost DM. "Autism is me": an investigation of how autistic individuals make sense of autism and stigma. Disability & society. 2022;37(3):427-453. doi:10.1080/09687599.2020.1822782
2. Turnock A, Langley K, Jones CRG. Understanding Stigma in Autism: A Narrative Review and Theoretical Model. Autism in adulthood. 2022;4(1):76-91. doi:10.1089/aut.2021.0005
3. Kaye HS, Jans LH, Jones EC. Why Don’t Employers Hire and Retain Workers with Disabilities? Journal of Occupational Rehabilitation. 2011;21(4):526-536. doi:10.1007/s10926-011-9302-8
4. Stangl AL, Earnshaw VA, Logie CH, et al. The health stigma and discrimination framework: a global, crosscutting framework to inform research, intervention development, and policy on health-related stigmas. BMC Medicine. 2019;17(1):31-31. doi:10.1186/s12916-019-1271-3
Ford | 14-21
Volume 12 ► Issue 1 ► May 2023
The Importance of Peer Support and Stigma Awareness: My Journey in Mental and Physical Health
Jamal A. Ford
At 14 months old my daughter was diagnosed with a brain tumor. We were told that she would likely succumb to her illness between the ages of five and seven. When we got this news, my now ex-wife and I were 23 years old and newly married. When you hear news like that, it is the loneliest feeling in the world. We did what we needed to do. We cared for our little girl. We tried to make her life as “normal” as it possibly could be, as long as we possibly could. When she was first diagnosed, I was working in the culinary field – a trained chef by trade. I switched professions, unknowingly, at the time, and that is when I first started working in mental health.
Time continued to pass. When she was six, her tumor had begun to grow at a rate where her doctor said she would not live through the end of the year. Her tumor was classified as inoperable, so we did not know what to do. It could not be removed but there was a small chance that someone could go in and debulk it, giving her brain stem some relief. We chose that option because it was the best one presented. September of that year, she was due to begin second grade. She attended the first day of school and then, the very next day, underwent the surgery we hoped would save her life. Life would never be the same after that.
She made it through the surgery, though she remained in a coma for six months after. She was put on hospice, and we were told that she would pass in that state. Then one day she decided to open her eyes and return to us. Still the same loving little girl she was before she went to sleep, but now she presented with a host of mental health and physical health issues that she did not have prior to the surgery. She had to learn to walk and talk again, attended frequent appointments with an occupational therapist, physical therapist, speech therapist, teachers, etc... It was overwhelming. When she was in the hospital, we only had to worry about our own jobs. Things changed drastically once we were released and back home.
I was ignorant to the stigma that existed when it came to mental and physical health. I had never really had to deal with the system in that manner. We did not know where to go for help and resources were not offered. We were told that we made too much money as a couple to qualify for assistance and so we struggled. Then we stopped asking for help. We started to just handle things on our own, relying on very few people for anything. As she grew, her condition worsened. She lost her ability to walk, talk, and eventually became bed ridden. She lived to be almost 16 years old. We could not receive home care for her until the last two years of her life. As parents, we suffered through depression, anxiety, and lack of communication. We took care of her and lost ourselves in that process because no one cared. At least, that is how it felt. We stopped seeking help, which is a very real effect of stigma. As a result, we suffered through until our daughter passed in 2015, after a very long, hard fought battle.
My story is not different than many families out there. The circumstances change but the feelings of loneliness, being overwhelmed, feeling like a burden, and feeling lost are the same. This is why shedding the light on stigma and letting people know that supports do exist is very important in the work that we do. I feel that if I had known more about the effects of stigma and the benefits of peer support, life might have been much different. Having people who can relate to what you are going through, point you to resources that may be unknown to you, and just lend an ear can be life changing. Knowing that you are not alone and learning to advocate for your needs is such an important part of those who are on a mental or physical health journey that cannot be overstated.
Here are some of the effects of stigma on mental health as experienced firsthand:
- It prevents people from seeking help. Many people who struggle with mental health issues are afraid or ashamed to admit that they need professional help, because they worry about being judged, rejected, or labeled as weak, crazy, or dangerous. This can delay or prevent them from getting the appropriate treatment and support that they need, which can worsen their condition and increase their risk of developing other problems such as substance abuse, isolation, or suicide.
- It reduces the quality of care. Even when people do seek help for their mental health problems, they may face stigma from health care providers, who may have biases or stereotypes about mental illness. This can affect the quality of care that they receive, such as being misdiagnosed, under-treated, over-medicated, or discharged too soon. It can also affect the relationship between the patient and the provider, making it harder to establish trust and rapport.
- It affects self-esteem and social relationships. People who experience stigma for their mental health problems may internalize the negative messages they hear from others, and start to believe that they are worthless, defective, or hopeless. This can damage their self-esteem and self-confidence and make them feel isolated and lonely. They may also face discrimination or harassment in various aspects of their lives, such as education, employment, housing, or legal rights. This can limit their opportunities and choices and affect their social and economic well-being.
- It creates a cycle of stigma. The stigma around mental health can create a vicious cycle that reinforces itself. For example, people who have mental health problems may avoid seeking help because of stigma, which can make their condition worse and more visible to others. This can then increase the stigma that they face from others, which can make them more reluctant to seek help again. This cycle can perpetuate the myths and misconceptions about mental illness and prevent people from understanding and accepting it.
Stigma around mental health is a challenge that affects millions of people around the world. It is a barrier to recovery and wellness, and a source of suffering and injustice. It is also a challenge that can be overcome by raising awareness, educating ourselves and others, challenging stereotypes and discrimination, and supporting people who have mental health problems. By doing so, we can create a more compassionate and inclusive society where everyone can thrive.
Why is peer support important?
Peer support is a form of mutual help that involves people with similar experiences of mental health challenges supporting each other. Peer support can take place in various settings, such as online communities, support groups, peer coaching, or peer workers in mental health services. Peer support can offer many benefits for people who are struggling with their mental health, such as:
- Connection: Peer support can reduce the feelings of loneliness and isolation that often accompany mental health problems. By connecting with others who have gone through similar situations, peer support can provide a sense of belonging and understanding.
- Validation: Peer support can help people to feel heard and accepted for who they are. By sharing their stories and emotions, peer support can offer a safe space where people can express themselves without fear of judgment or stigma.
- Normalization: Peer support can help people to realize that they are not alone or abnormal in their experiences. By learning from others who have faced similar challenges and overcome them, peer support can foster a sense of hope and possibility for recovery.
- Purpose: Peer support can give people a sense of meaning and direction in their lives. By helping others, peer support can boost self-esteem and confidence. By receiving help, peer support can empower people to take charge of their own well-being and goals.
- Hope: Peer support can inspire people to believe that change is possible and that they can overcome their difficulties. By seeing the examples of others who have recovered or improved their mental health, peer support can motivate people to pursue their own recovery journey.
Peer support is not only beneficial for the individuals who receive it, but also for those who provide it. Research has shown that peer support workers (PSWs), who are trained and employed to use their lived experience to help others, can experience positive outcomes such as:
- Improved self-care and coping skills
- Increased social inclusion and community involvement
- Enhanced problem-solving and communication skills
- Greater access to work and education opportunities
- Higher levels of satisfaction, optimism, and acceptance
Peer support is based on the principles of mutual respect, empathy, reciprocity, and recovery. Peer support recognizes the value of personal experience and the potential of every person to grow and heal. Peer support is not a substitute for professional treatment, but rather a complement that can enhance the quality and effectiveness of mental health care.1,2
Peer support is important because it can offer a unique perspective and a different kind of support that professional services may not be able to provide. Peer support can help people to feel less alone, more understood, more empowered, and more hopeful about their mental health.
Mental health is a vital aspect of our well-being, but it is often neglected or misunderstood by many people. One of the reasons why mental health is not given enough attention or support is the stigma that surrounds it. Stigma is a negative attitude or belief that leads to discrimination or prejudice against people who have mental health problems. Stigma can have serious consequences for individuals and society, and it is a challenge that needs to be addressed. Our children deserve the care they need. Our families deserve the support. Normalize mental and physical health resources and end the stigma that surrounds those in need. Our world will be a much better place as a result.
References
1. Mead, S., Hilton, D., Curtis, L. “Peer Support: A Theoretical Perspective.” Accessed May 8, 2023. PSRJ article.PDF (intentionalpeersupport.org)
2. Substance Abuse and Mental Health Services Administration. Peer Support Workers for those in Recovery. Accessed May 8, 2023. Peer Support Workers for those in Recovery | SAMHSA.
Biography
Jamal joined the PA Care Partnership in August of 2018 after spending seventeen years at a residential treatment facility working with court adjudicated young men. Working in the RTF, he acquired a wealth of experience in the various positions he worked, including direct care, ropes course coordinator, director of therapeutic activities, and one-to-one care. He helped to implement the Sanctuary Model at the RTF which led to an opportunity to learn about Trauma-Informed Care from Lakeside Global Institute. His personal experience, along with his work at the RTF, fostered a desire to deepen his understanding and further his advocacy for youth voice. Jamal is currently continuing his education at Morehouse College and continues to use his experience and knowledge to help counties implement the system of care philosophy.
Contact Information
Jamal A. Ford
PA Care Partnership - Statewide Systems of Care Grant
Certified Peer Support Specialist (CPSS), Youth Resources Coordinator
fordj3@upmc.edu or c-jford@pa.gov
Quick & Schnoke | 22-26
Volume 12 ► Issue 1 ► May 2023
Life Through My Lens:
An Exploration of Self-Stigma
Dr. Kathy Quick, LSW, CPS and Tristan Schnoke, CPS
In the mental health world, everyone talks about the stigma that surrounds having a mental illness. But as with any problem-solving process, it is always beneficial to get to the root of the problem to develop an effective solution. Kathy and Tristan, the authors of this article, frequently share about their battles with self-stigma. They propose that the way we think of ourselves is the root cause of the pervasive and devastating mental health stigma in our communities.
Kathy experienced childhood trauma, extensive bullying, and problems with body image and weight, which led her down a dark road of self-loathing, feelings of inadequacy, and self-blame, which ultimately resulted in decades of substance use, inappropriate and abusive relationships, suicidal ideation, and a suicide attempt.
As a child, Tristan experienced domestic violence in the home, emotional abuse, and mental abuse. As she grew up, she found more relationships filled with the same. She struggled to find any value in herself and practiced blaming, shaming, and guilting herself for everything that had ever gone wrong in her life for a long time.
After a long journey through different types of employment, both Kathy and Tristan have found their way to the Pennsylvania Mental Health Consumers’ Association (PMHCA). Kathy’s journey took her through college, ultimately resulting in three degrees but not before she spent time grooming racehorses, working in factories, and cleaning bathrooms in a bar. After engaging in her educational journey, Kathy also worked in child welfare, outpatient therapy, family-based therapy, county government, and finally landed at PMHCA where she was able to freely acknowledge and speak about her life experiences and become a Certified Peer Specialist.
Tristan’s employment journey also included many different fields including waitressing, customer service, sales, and the labor industry. She found employment at PMHCA and was able to complete the Certified Peer Specialist training, which transformed the way she looked at her life and herself. Both Kathy and Tristan are currently taking the Certified Family Recovery Specialist training, and Kathy will also be eligible to receive the Certified Recovery Specialist certification. These certifications will allow Kathy and Tristan to provide peer services to family members of people with substance use disorder and Kathy to work with the individual themselves.
Kathy and Tristan are not only mother and daughter, but coworkers, too. During their time at PMCHA, they have discovered that as valuable as community stigma reduction efforts are, there is so much more work to be done. Stigma reduction typically focuses on how the outside person should treat the person with a mental illness and changing the way people view those who have struggled with mental health. Tristan and Kathy, and ultimately PMHCA, take a different perspective on stigma reduction that starts within the individual. We will never be able to make worldwide change if we don’t believe that we are worthy of positive treatment in the first place. The way we speak to ourselves dictates the treatment we accept from others.
The PMHCA team has started to advocate for this viewpoint to be brought to light and allow others to understand that the way they view themselves is the starting point to destroying stigma around the globe. With that concept in mind, Tristan and her co-workers from PMHCA created a workshop called “Life Through My Lens” which is an easy-to-understand way of describing this different perspective on stigma reduction and provides practical, real-life ways we can begin to address our own self-stigma.
The workshop helps people truly understand what it means to feel good about themselves. It helps people to connect the dots that were lost as a result of negative life experiences. PMHCA is offering this workshop to anyone who feels it may be helpful for them and their community. Details can be found on the website or by contacting either Kathy or Tristan.
https://pmhca.wildapricot.org/Life-Through-My-Lens-Workshop
Biographies
Dr. Kathy Quick serves as the Executive Director of the Pennsylvania Mental Health Consumers' Association (PMHCA). Dr. Quick is very invested in ensuring that individuals in recovery from mental illness have their voices heard. Dr. Quick is in long-term recovery from mental illness as well as alcohol addiction, and she shares her story to inspire others to embrace recovery and hope. Dr. Quick received her bachelor's degree from Penn State University in 1998, majoring in Criminal Justice. She went on to receive a master’s degree in social work from Temple University in 2005, and her Doctorate in Social Work from Capella University in 2020. She had over 20 years of experience in providing treatment services in mental health, family treatment, children's services, substance use disorder treatment, and local government before joining PMHCA. Dr. Quick is a resident of Schuylkill County with her husband, German Shepherd Duke, and three cats: Little AK, Molly and Princess Fiona. Dr. Quick's recovery tools include reading, hunting, painting, crocheting, counted cross-stitch, and gardening.
Tristan Schnoke is a young adult who is married, has a child, owns pets, and has a mental illness that she battles every single day. She has learned to grow through things instead of trying to jump over them and that has helped her to become a strong advocate for other young people who struggle with mental health and traumatic experiences. As the Program Director at PMHCA, Tristan's goal is to make sure that everyone's experiences are being included, heard, and understood when changes to the mental health system are being made. You have a voice, and we need to hear it!
Contact Information
Dr. Kathy Quick, LSW, CPS
Executive Director of PMHCA
Tristan Schnoke, CPS
Program Director at PMHCA
Tristan@pmhca.orgMaguire, Haag, Benedetto | 27-37
Volume 12 ► Issue 1 ► May 2023
Overcoming Stigma through Education and Capacity Building in Communities
Helena Maguire, M.S., LABA, BCBA, CDE®
Maggie Haag, M.Ed., BCBA, LSW, CDE®
Ashley Benedetto, M.S. Ed., BCBA
Introduction
Stigma has always been part of the experience of those with disabilities. While much has been done legally to reduce stigmatization and to increase opportunities, challenges in creating maximal opportunities for those with disabilities remain. One of the primary clinical challenges is to ensure that the voice of the individual is solicited, valued, heard, and genuinely integrated into the treatment plan. For individuals with complex needs, it is especially important to ensure that their voices are heard, that their strengths are recognized, and that supports are provided.
Our case study illustrates creative ways that the preferences and needs of an individual with complex needs can be solicited, observed, and integrated into a plan of care. The case also highlights how important it is to build collaborative supports within the community, including within job placements.
We must continue to listen to the disability community about their needs and the best way to support a person with a disability. The critical factor is ensuring that the person receiving supports is actively involved in all aspects of planning to the greatest degree possible. Additionally, we must listen and heed the words of the advocates who are also disabled, learn from their feedback, and involve them in our work.
Stigma
Social Stigma1, according to Wikipedia, is the disapproval of, or is discrimination against an individual or identifiable group of people based on perceived characteristics that serve to distinguish them from other members of a society. Stigma can negatively affect the emotional, mental, and physical health of affected individuals, often resulting in isolation or feelings of depression, anxiety, and shame. At times, we see that social stigma also leads to discriminatory acts by others. Such discrimination can be intentional or can be a result of an unconscious bias. Regardless of the motivation, individuals may have experiences of rejection by other groups, or may experience verbal abuse or physical abuse, or may be denied access to basic needs such as education, healthcare, and employment. Many of these actions involve violations of human rights; these actions undermine the dignity of those with disabilities and fail to uphold the value of ensuring respectful care.
In 1972, Dr. Wolf Wolfensberger wrote the seminal article, “The Principles of Normalization.”2 This article highlighted the primary philosophy that all people with disabilities should be supported in leading their lives like others in their community and of their similar age. It emphasized that people with disabilities should be offered the same opportunities and environmental conditions to have a normal course of life. Dr. Wolfensberger offered a few guiding principles that included:
- Supporting the development of personal behaviors and characteristics that are culturally normative. (Please note that this can change over time, as such goals evolve over time with cultural changes. It has also been altered and influenced by an explicit value on individual difference and disability identity.)
- Supporting individuals to look and behave in ways that are considered culturally appropriate and similar to that culture relative to age and sex. (This can also change over time and should be flexible based on personal preferences and has also been altered by explicit values on individual differences and identities. However, the intent was to ensure that the individual’s dignity was always prioritized, and that their opportunities were maximized.)
- Supporting individuals to interact with others at an individual level, family level, peer group, school and education systems levels, in neighborhoods, in vocational /work settings, and through navigating social justice systems.
Overcoming Stigma
Since the writing of this 1972 article, several advances have been made in providing individuals with disabilities with equal opportunities. Laws have been passed prohibiting discrimination in schools and employment sectors.4,5 For example, special education laws, teacher training, and training and specialization in healthcare fields to promote comprehensive care has been emphasized in residency programs. In addition, disabilities awareness and specialty trainings for law enforcement personnel have been implemented nationwide. These advances are significant, and their attempts should be noted given the impact they have had thus far in attempting to equalize the opportunities for all individuals with disabilities. While we have certainly come a long way in reducing stigma, perseverance is still needed in finding ways to support people with disabilities in overcoming stigma. A major element of this movement involves having the community at large widen their definition of acceptable. Social acceptance of difference is key to improved outcomes.
Since some cultural norms change over time, we need to continually ask how we are helping overcome stigma. At the individual level, do we see the person we are supporting as able to dream and design a life by which they feel fulfilled? Or do we feel we “know better” and design a lifestyle for them with little regard to their desires? As a support system, we need to make sure we have educated ourselves about disabilities to be better positioned to support people with disabilities. Being supportive means treating people with dignity and respect and working together to figure out what they find meaningful. Establishing a better understanding of their personality and personal attributes can help us support their goals. In addition, helping family members in the process of supporting their loved one’s needs and desires allows that person to continue to thrive in loving environments and communities they live in.6
Helping people with disabilities overcome stigma and discrimination includes educating other members of the community who can also help support their needs in a natural way.7 A person’s community includes neighbors, schools, first responders, physicians, businesses, prospective employers, and any other location in the community that is important to that person.8 We need to help support people with disabilities to be fully integrated community members by ensuring they receive the appropriate access to education, healthcare, goods and services, and have the opportunity to have access to competitive employment, which can involve specific skills training. Disability advocates continually point out the ways in which marginalization continues to occur; we need to include those voices in all elements of planning and service provision. Elevating those voices ensures that we are including them as partners in these processes.
In addition to continuing to educate others on the abilities of people with disabilities, it is crucial to be careful with our words given that the language we use can significantly impact stigma reduction. Our words and conversations need to be supportive and positive in order to impact stereotypes that may still exist within the community. Remaining positive and highlighting the contributions of a person with a disability helps support them and assists other community or family members to value the person’s contributions. Ensuring that we see and name the “person” instead of referring to them as clients or patients helps others see the person too.
Case Study
The following case study illustrates an example of how one person was supported in ways that overcame stigma in their community.
William is a 38-year-old male diagnosed with an intellectual disability who resides in a home in the community. William receives 24-hour support from direct support professionals (DSPs) who work in his home as well as the program he attends during the day. William also receives behavior services to help support him to learn how to communicate his needs instead of engaging in behaviors that may be considered dangerous or disruptive, such as aggressive behaviors toward others, destruction of property, or yelling at others. William has great communication skills and is able to engage in conversations with others. He loves to help and will jump right in when he sees someone start to take the trash out or wipe down a table. He has strong gross motor skills and enjoys participating in a variety of vocational activities. William expressed a desire to be competitively employed, and the aforementioned skills helped his support teamwork with him to identify possible jobs of interest. Competitive employment involves working in the community while earning a competitive wage (i.e., earning what someone else working the same job without a disability makes, at minimum wage or higher), with the ultimate goal being to have natural community supports. Natural supports in an employment setting include co-workers, managers, and any other person who will be naturally in the environment, as opposed to a paid caregiver.
In order to help make William’s community involvement a success, preparation occurred for him, the community, and the DSPs providing support. To prepare William for success, his preferences were evaluated and community jobs/locations meeting those preferences were identified. William has full autonomy regarding when he accesses the community and what activities are completed. To prepare the natural supports at the job location, the DSP demonstrates for coworkers and community members that all interactions should be with William, and not with the DSP. They also demonstrate and teach how to build a relationship and how to respond if William starts to become agitated. They also demonstrate the best way to teach William any new skills.
Initially, William attended work once a week at the convenience store for 30 minutes and would complete a highly preferred job duty (taking out the trash). The length of time William attended and the number of days were slowly increased, closely monitoring his preferences and choices. This gradual increase allowed the co-workers to get to know William and build a relationship. Once that relationship was built, the DSP was able to step back, and the natural supports took over. William’s DSP pays close attention to his verbal and physical cues, and if he becomes agitated or overwhelmed, he is reminded of his ability to take a break, or even to leave work early. Because the relationship was developed over time with careful attention to relationship building, the place of employment understands the need for flexibility and William is permitted to leave early, come in late, switch days, etc., based on his needs. William has also developed relationships with community members who frequent the store and will notice if he’s been out for a few days. They too help to provide the natural supports needed to secure successful community involvement.
By educating the natural supports in William’s community about his needs and how to best support him, stigma around any perceived differences has been minimized and replaced with genuine care and concern for him as a person.
Conclusion
Though much progress has been made both legally and culturally related to discriminatory practices, there is still work to be done to create inclusive environments in all sectors of life. Modeling how to be inclusive in our everyday lives is crucial.
We must also continue to listen to the disability community about their needs and the best way to support a person with a disability in achieving the goals they set for themselves. While there are general guidelines for providing this support, specifics are determined by the person receiving supports and will look different for each person. The critical factor is ensuring that the person receiving supports is actively involved in all aspects of planning to the greatest degree possible. Additionally, we must listen and heed the words of the advocates who are also disabled, learn from their feedback, and involve them in our work.
References
1. Wikipedia, Social Stigma definition. https://en.wikipedia.org/wiki/Social_stigma. Accessed May 8, 2023.
2. Wolfensberger,
Wolf P.; Nirje, Bengt; Olshansky, Simon; Perske, Robert; and Roos, Philip,
"The Principle of Normalization in Human Services" (1972). Books:
Wolfensberger Collection.
https://digitalcommons.unmc.edu/wolf_books/1
3. U.S. Department of Education, Office for Civil Rights, Free Appropriate Public Education for Students with Disabilities: Requirements Under Section 504 of the Rehabilitation Act of 1973, Washington, D.C., 2010.
4. Americans With Disabilities Act of 1990, 42 U.S.C. § 12101 et seq. (1990)
5. Office of the Federal Register, National Archives and Records Administration. 122 Stat. 3553 - ADA Amendments Act of 2008.
6. Center for Disease Control. (2020). Disability and Health Inclusion Strategies. https://www.cdc.gov/ncbddd/disabilityandhealth/disability-strategies.html. Accessed May 1,2023.
7. Unicef. (2020). Reducing Stigma and discrimination against children with disabilities. Social and Behavioural Change Interventions to Strengthen Disability Inclusive Programming Summary. https://www.unicef.org/media/120421/file/Social_and_Behavioural_Change_Interventions_to_Strengthen_Disability_Inclusive_Programming_Summary.pdf. Accessed May 8, 2023.
8. Parenti, K. (2017). Clinical Corner: First responder education in autism. Science in Autism Treatment, 19(7). Accessed May 8, 2023.
Biographies
Helena Maguire serves as the Executive Director of Melmark New England. She oversees the development and implementation of programs and
services, as well as the daily operations for Melmark New England. She develops strategic objectives for the Massachusetts division and provides leadership to direct reports in order to assure the achievement of these objectives. Ms. Maguire supports the CEO through various committees and activities, and assumes responsibility for policy development, quality assurance, risk management, regulatory compliance, fiscal integrity, and excellence in care and delivery of all services. Ms. Maguire has presented numerous papers on staff management and staff training techniques, both at the local level and at the national level. Ms. Maguire is an Adjunct Professor at Endicott College and the University of Massachusetts-Boston.
Maggie Haag is a Board Certified Behavior Analyst and Pennsylvania-licensed social worker who has been working with individuals with autism spectrum disorders (ASD) and intellectual disabilities since 2003. She earned her bachelor’s degree in psychology from West Chester University in 2003, as well as her master’s degree in social work in 2012. Ms. Haag earned a Master of Education in Autism and Applied Behavior Analysis in 2018 from Endicott University. Ms. Haag began her career working for Devereux’s Children’s Intellectual and Development Disabilities Services programs in West Chester, Pa., where she supervised residential treatment programs for children and young adults. Following her work with children’s residential programs, she became the Program Director for Devereux’s Community Adult Autism Partnership Program, where she expanded community services for adults with ASD and Intellectual Disabilities. Ms. Haag began her career at Melmark in 2015 as the Director of campus-based adult residential programs, where she oversaw the comprehensive programming of adults with intellectual disabilities and varying medical challenges. Most recently, she served as the Senior Director of Melmark’s Adult Services Programs. She is currently the Executive Director of Melmark Pennsylvania.
Ashley Benedetto received her bachelor’s degree in Education from West Chester University and her master’s degree in Applied Behavior Analysis from Temple University. She is also a Board Certified Behavior Analyst. Ashley started her career at Melmark in 2010 as a direct support professional in children’s residential services and was later promoted to a Program Manager position. Ashley then moved into adult services where she gained experience in a variety of roles such as Program Manager, Behavior Specialist, Program Specialist, and Assistant Director. In 2016, she became the Director of Adult Day Programs, serving in that position for over six years. Ashley is currently serves as Senior Director of Educational Services.
Contact Information
Helena Maguire, M.S., LABA, BCBA, CDE®
Melmark New England
Executive Director
Maggie Haag, M.Ed., BCBA, LSW, CDE®
Melmark Pennsylvania
Executive Director
Ashley Benedetto, M.S. Ed., BCBA
Melmark Pennsylvania
Senior Director of Educational Services
Diaz | 38-45
Volume 12 ► Issue 1 ► May 2023
Mental Health Stigma Across Ethnic Minority Identities
Koebe S. Diaz
Abstract
Mental health stigma impacts our view on mental health and mental health care. These stigmas can be different according to our ethnic and racial identity. It is important to acknowledge the differences that may exist because of our identities and use this to drive our research and practice so that we can ensure that all individuals are receiving quality and culturally relevant health care.
Mental health stigma emerges when there is a societal misunderstanding of mental health diagnoses and how they may affect a person.1 The effects of mental health stigma can be felt in various ways, including discrimination in the workplace, misconceptions of capabilities, and influence on self-perception. These same stigmas that people use to judge others also influence how they view mental health for themselves, which can be referred to as “self-stigma.”1 A mental health diagnosis is often viewed as if the individual is at fault for their diagnosis, unlike a person who has a physical ailment such as the flu or cancer. Mental health stigma impacts how people are viewed and treated when they receive a mental health diagnosis. This can impact a person’s eagerness to acknowledge their need for mental health services.
Racial and ethnic minority groups have historically been marginalized in the United States. This discrimination is embedded within large institutions and systems. Over time, the result of this discrimination has caused a lack of trust between marginalized groups and these institutions, one of them being the health care system. Within the health care system, race and ethnicity have an impact on the quality of care a person can receive. This may be due to socioeconomic disadvantages, geographical restrictions, discrimination at the hands of health care providers, and a lack of cultural competency.2 The disparities that exist within the health care system can discourage individuals from accessing services and reaching out for assistance when needed. It is reported that 51.8% of white Americans will receive treatment related to a mental health condition each year. This rate is significantly higher than other racial and ethnic groups; 35.1% for the Hispanic population, 37.1% for Black Americans, and 20.8% for Asian Americans.3
Black Americans are, when compared to white Americans, less likely to be included in research, and “less likely to be offered evidence-based medication therapy or psychotherapy.”4 Hispanic children are, at times, at a greater risk for psychological disorders than white American children.5 Additionally, racial and ethnic minority groups face a variety of barriers to accessing mental health care. There are structural barriers that exclude racial and ethnic minority groups from accessing quality mental health services, which only strengthens mental health stigma among these communities. Some examples of these barriers include, language,6 legal restrictions,6 and a history of discrimination, misdiagnosis, and mistreatment by the healthcare institution.7 It is important that we challenge these ideas and offer perspectives that encompass the multiple racial, ethnic, and cultural identities that exist within the United States.
There are many factors that contribute to the different experiences of mental health stigma that ethnic and racial minority groups face including language barriers, access to care, access to culturally competent care, and cultural or personal beliefs and attitudes.4,7,8,9 Two large factors that exist across racial and ethnic minorities that contribute to mental health stigma are strong religious affiliations and a desire not to appear “weak”. The strong religious affiliations that exist within these communities act as support and familiarity in the face of discrimination and adversity. Strong religious ties are often barriers to accepting mental health concerns that are disregarded and believed to be treatable through their participation in religious services.9,10 The desire to not appear “weak” or “crazy” is a common sentiment throughout many racial and ethnic minority groups and is a common factor of mental health stigma within these communities.8,9,10
Additionally, within specific ethnic and racial minority groups, there are culturally specific factors that impact mental health stigma for each cultural group. For example, Asian Americans are the least likely group in the United States to seek care for a mental health related issue.11 The “model minority” myth is a harmful stereotype which suggests that all Asian Americans possess the same characteristics which allow them to succeed more than other racial and ethnic groups, resulting in added pressure to reach these expectations.12 The existence of stereotypes, such as the model minority myth, strengthens mental health stigma within the Asian community, as it enforces the need to not be seen as “weak” or “less than”. This sentiment can also be extended to the strong cultural traditions that emphasize the importance of family and interdependence. If a person is viewed as not being able to provide due to mental health issues, they may fear that they will be viewed negatively.13 Many Black Americans experience mental health stigma due to a mistrust of the medical field which is due to a history of mistreatment, discrimination, and exploitation. This results in a reluctance to receive care for both mental and physical health needs.7 In Hispanic/Latinx culture, privacy is valued and expected, so the topic of mental health is preferred to remain within the family and not to be discussed publicly.8
To bridge the gaps that exist in research and implementation of mental health care with historically and systemically marginalized groups, we must question our current methods and structures. We must acknowledge the gaps in our research to fill them. In a systematic review on culturally competent health care interventions, it was found there is still a need for research in this area.6 We need more examinations of current culturally competent strategies and interventions to develop evidence-based strategies. In gaining knowledge we begin to move forward and correct the misinformation that continues to harm ethnic and racial minority groups. Setting up lines of research dedicated to understanding the racial and ethnic minority experience in the United States may be a good place to start. We can also enhance our individual understandings of cultural competency and integrate it into our daily lives and aim to repair the relationships between large institutions and marginalized groups. Some helpful resources related to cultural competency in healthcare can be found at; APA Cultural Competency, Guidelines and Strategies for Cultural Competency, Think Cultural Health, and National Center for Cultural Competency Georgetown University. Truly understanding the population that we wish to serve, especially those who have experienced systemic and institutional racism and discrimination, will aid us in building meaningful connections and trust.
References
1. Rusch N., Angermeyer M. C., Corrigan P. W. Mental illness stigma: concepts, consequences, and initiatives to reduce stigma. European psychiatry 2005 20 (2005) 529–539. Doi: https://doi.org/10.1016/j.eurpsy.2005.04.004
2. Thomeer, M.B., Moody, M.D. & Yahirun, J. Racial and Ethnic Disparities in Mental Health and Mental Health Care During The COVID-19 Pandemic. J. Racial and Ethnic Health Disparities 10, 961–976 (2023). https://doi.org/10.1007/s40615-022-01284-9
3. National Alliance on Mental Illness (NAMI), Mental Health By The Numbers. https://www.nami.org/mhstats. Accessed March 26, 2023.
4. Mental health disparities: African Americans. American Psychiatric Association. https://www.psychiatry.org/File%20Library/Psychiatrists/Cultural-Competency/Mental-Health-Disparities/Mental-Health-Facts-for-African-Americans.pdf. Accessed March 27, 2023.
5. Mental health disparities: Hispanics and Latinos. American Psychiatric Association. https://www.psychiatry.org/File%20Library/Psychiatrists/Cultural-Competency/Mental-Health-Disparities/Mental-Health-Facts-for-Hispanic-Latino.pdf. Accessed March 27, 2023.
6. Handtke O, Schilgen B, Mösko M (2019) Culturally competent healthcare – A scoping review of strategies implemented in healthcare organizations and a model of culturally competent healthcare provision. PLoS ONE 14(7): e0219971. https://doi.org/10.1371/journal.pone.0219971
7. Why mental health care is stigmatized in black communities. USC Suzanne Dworak-Peck School of Social Work. https://dworakpeck.usc.edu/news/why-mental-health-care-stigmatized-black-communities. Accessed March 27, 2023.
8. Hispanic/Latinx. NAMI. https://www.nami.org/Your-Journey/Identity-and-Cultural-Dimensions/Hispanic-Latinx. Accessed March 27, 2023.
9. Why Asian Americans don't seek help for mental illness. Why Asian Americans Don't Seek Help for Mental Illness | McLean Hospital. https://www.mcleanhospital.org/essential/why-asian-americans-dont-seek-help-mental-illness. Published May 1, 2022. Accessed March 27, 2023.
10. Black/African American. NAMI. https://www.nami.org/Your-Journey/Identity-and-Cultural-Dimensions/Black-African-American. Accessed March 27, 2023.
11. Asian American / Pacific Islander communities and Mental Health. Mental Health America. https://www.mhanational.org/issues/asian-american-pacific-islander-communities-and-mental-health. Accessed March 27, 2023.
12. What is the model minority myth? Learning For Social Justice. Blackburn S.S., https://www.learningforjustice.org/magazine/what-is-the-model-minority-myth. Accessed March 30, 2023.
13. Asian American Mental Health: Stigma, culture, and more. Medical News Today. https://www.medicalnewstoday.com/articles/asian-american-mental-health#why-is-there-a-stigma. Accessed March 27, 2023.
14. Kirmayer L. J., MD, Groleau D., PhD, Guzder J., MD, Blake C., PhD, Jarvis E., MD, MSc. Cultural consultation: A model of mental health service for multicultural societies. The Candadian journal of psychiatry. 2003 48(3). doi: https://doi.org/10.1177/070674370304800302
15. Black and African American communities and Mental Health. Mental Health America. https://www.mhanational.org/issues/black-and-african-american-communities-and-mental-health. Accessed March 27, 2023.
16. Mental health disparities: Diverse Populations. American Psychiatric Association. https://www.psychiatry.org/File%20Library/Psychiatrists/Cultural-Competency/Mental-Health-Disparities/Mental-Health-Facts-for-Diverse-Populations.pdf. Accessed March 27, 2023.
Biography
Koebe S. Diaz is a Research Coordinator at A.J. Drexel Autism Institute at the Policy, Analytics, and Community (PAC) Research Program. She has experience working as an undergraduate research assistant and hopes to continue working on research that focuses on mental health care for ethnic and racial minority groups.
Contact Information
Koebe S. Diaz
A.J. Drexel Autism Institute
Murray, Layton, Logan | 46-59
Volume 12 ► Issue 1 ► May 2023
Lessons from the Community: The Critical Importance of Lived Experience When Designing Trauma Recovery Programs.
Michael Murray, Andrea Layton, and Jeanne Logan
Abstract
This article reviews the importance of community engagement when designing clinical interventions and supports. This is especially timely given the need for enhanced trauma recovery and resilience building needs for the neurodivergent community following the increased awareness of the victimization/traumatization risks for autistic, intellectually disabled, and/or developmentally disabled individuals as well as the universal traumatic exposure resulting from the COVID-19 pandemic. Guiding principles for effective community engagement are reviewed. The four key activities of the community coalition action theory are reviewed and demonstrated by discussions of two recent Autism Services, Education, Resources and Training collaborative (ASERT) projects—TRAIN and Project ECHO.
Public health concerns are increasing in scope and impact. COVID-19 was a global event with universal range—everyone was truly impacted to some degree. There has not been such a universal trauma exposure in our lifetimes. Despite this there were positive outcomes resulting from the pandemic. One of these has been the emphasis on community engagement as we struggle to expand access to quality care, prevent disease, and achieve greater health equity. As clinicians and investigators, we are being increasingly encouraged to engage key stakeholders when designing health promotion programs and interventions. But what does this really mean? What is the community to be considered and what constitutes engagement? The Centers for Disease Control (CDC) defines community engagement as “the process of working collaboratively with groups of people who are affiliated by geographic proximity, special interests, or similar situation with respect to issues affecting their well-being.”1
When the ASERT collaborative became interested in addressing trauma recovery needs for our community members, it was clear that all of the elements that the CDC definition reference were present as the team started to contemplate this work: a group of people affiliated by proximity (Pennsylvania), special interest (trauma risk reduction and more effective intervention) and similar situation (members of the neurodivergent community) that affects health and well-being. What was not as obvious was how to best engage this community.
The concept of community engagement has expanded. Key stakeholders—especially those with lived experience—have critical information to share for outreach, education, and intervention efforts. Furthermore, lived experiences should be considered central to the design of these efforts. Successful engagement strategies can range from highly structured and formalized to grassroots level led coalitions, but the most successful enable sustained and committed engagement among partners working on well-defined goals with actionable strategy. In 2022, the National Academy of Medicine published a report from their national workgroup aimed at identifying best practices for community engagement in health care programs and policies.2 In this report, core principles for fully engaged community participation in design and execution of policy and practice were identified. They included: trust; bi-directionality; inclusiveness; culturally-centeredness; and equitably financed. These core principles promote multi-knowledge and informed projects with shared governance.
Butterfoss and Kegler describe four key activities in their community coalition action theory widely considered to be one of the strongest models for promoting inclusive and sustained community engagement:3
1. Know the community: This is the intelligence gathering phase where the history, experiences, and capabilities of key stakeholders are gathered and integrated. Identifying and understanding needs develops collectively.
2. Establish positions and strategies: Active attention and support from shared engaged leadership leads to identification of goals and key activities. This needs to occur within the structural capacity of the partners where existing limitations need to be recognized. Long-term intentions and openness to change resulting from community input needs to be clearly communicated on an ongoing basis as needs and experiences change so may overarching priorities.
3. Build and sustain networks: Leadership should seek communication opportunities with those within the network as well as other aligned stakeholders outside of the network. This communication should occur formally and informally so as to promote free exchange of information and perspectives. Existing network structure (communication efficacy, shared power, and resource flow) should be analyzed and modified to meet ongoing needs. Communication and resource allocations should target and leverage agenda-setting priorities for the larger community for greatest sustainability.
4. Mobilize constituencies: Earning and re-earning trust is an ongoing process in efforts to maintain commitment and engagement from all parties. Cyclically moving through process of dialog, debate, and decision-making achieves greatest ongoing commitment to what should be constantly evolving collaborative goals.
With this framework and guiding principles in mind, the ASERT Collaborative utilized a community engagement approach when designing and implementing two new initiatives aimed at responding to the growing need for neurodivergent-informed trauma resources.
Issue 1: The critical gap of qualified therapists equipped to offer evidence-based treatment for the growing number of neurodivergent individuals coming forward with their experienced trauma.
According to the most recently available Pennsylvania Adult Protective Services (APS) report for fiscal year 2020-21, there were 15,249 reports of abuse, neglect, exploitation or abandonment with 7,082 of these reports ultimately being substantiated.4 Of course, this figure does not represent all of the victimization experiences and there are many other types of trauma—both past and present—which are not victimizations or reportable under APS guidelines.
In 2018, the Office of Developmental Programs’ (ODP) Information Sharing and Advisory Committee (ISAC) discussed the growing awareness of the high vulnerability for victimization and trauma exposures for neurodivergent individuals. The ASERT team initially responded by partnering with state Milestone Health Care Quality Unit (HCQU); Temple Institute on Disabilities (Temple IoD); Office of Developmental Programs (ODP) and national partners (National Crime Violence Research and Treatment Center at the Medical University of South Carolina) to create a resource collection aimed at reducing risk (prevention strategies) and informing stakeholders what good care should look like (intervention strategies). Additional information can be found at www.PAAutism.org/BeSafe. But it became apparent during subsequent conversations with ISAC and other community stakeholders that the lack of treatment options for individuals after they disclosed their victimization and trauma experiences was a significant barrier. Essentially the good evidence-based care that the resource collection described was difficult to access.
This led to next stage of this project—training therapists to modify evidence-based treatment for trauma recovery to meet the needs of neurodivergent individuals. In addition to partners already mentioned, the ASERT team determined it would be critical to incorporate as much lived experience perspective into this training as possible. This led to partnering with Self Advocates United as 1 (SAU-1) during the development of the training topics and content. Self Advocates United as 1 Power Coaches shared their victimization and/or trauma experiences, past ineffective treatment, and successful treatment experiences. Some Power Coaches agreed to being filmed while discussing these topics and this material was incorporated into the training materials providing powerful context for training concepts.
Trauma Recovery for Autistic, Intellectually disabled, and Neurodivergent individuals (TRAIN) consists of two components: a 12-week didactic portion of asynchronous webinars and synchronous clinical skills application workshops and a 12-week clinical consultation portion where trainees present a clinical case of a neurodivergent individual they are working with which provides an opportunity for the cohort to offer insights and feedback creating a strong learning collaborative. Lived experience from the SAU-1 Power Coaches and the case discussions pervades all aspects of this project. Thirty-three therapists have completed TRAIN to date and have come from both urban and rural areas from across the Commonwealth.
Community Coalition Action review for TRAIN
1. Know the community: ASERT has extensive experience engaging key stakeholder groups in the neurodivergent community. Early partners increased access to provider perspectives. Self Advocates United as 1—the critical community partner—provided feedback on topics, materials, and enriched TRAIN with lived experience perspectives.
2. Establish positions and strategies: Partners determined that increasing evidence-based therapy access for victimized and traumatized neurodivergent individuals was a high priority. While addressing the needs of non-speaking neurodivergent individuals is important, to do so will require exceptional clinical skills as the therapists will need to be well versed in evidence-based trauma recovery and augmentative/alternative communication strategies. The partners elected to initially focus on neurodivergent individuals with good expressive language skills so as to reduce therapist burden and increase buy-in for this effort. However, feedback from community members (including therapists who have completed TRAIN) indicate increased recognition of the need to better support non-speaking neurodivergent individuals—this has influenced the next development of the TRAIN project which will focus on individuals with significant cognitive and/or communication challenges.
3. Build and sustain networks: Information from the TRAIN project has been shared in a variety of ODP sponsored networks including newsletters and listservs as well as presentations at the Everyday Lives Dual Diagnosis Conference, the Residential Learning Collaborative, and the Pennsylvania Autism Training Conference. Past TRAIN participants have shared their experiences in testimonials and with colleagues. Subsequent cohorts of TRAIN participants have become easier to recruit reflecting greater awareness and interest in the project.
4. Mobilize constituencies: Collaboration with SAU-1 and other key community partners remain active as new directions for the work are considered leading to overall goal of increased capacity for evidence-based trauma recovery for neurodivergent individuals at all levels of disability in every county.
Issue 2: Combatting the high direct and indirect consequences of the pandemic for the neurodivergent community.
As mentioned previously, COVID-19 caused universal trauma exposure. The neurodivergent community was at particular risk due to heightened risks for morbidity and mortality during the initial phase of the pandemic; disruptions in highly relied upon community resources to provide stability and sense of well-being; isolation from loved ones leading to mental health challenges; and struggles adjusting to frequently changing “new normal.”2 Moreover, this population which is already at high risk for victimization and adverse life events may have experienced trauma directly related to the pandemic and mandated containment measures—including stay-at-home orders resulting in isolation and lack of services. They may have also experienced exacerbation of pre-exiting or unresolved trauma issues.
Fostering resilience is of critical importance in enhancing adaptive stress responses. Some resilience needs are universal; individuals who had been at home for months are now re-engaging with their communities at some level. Other resilience needs are more specific to an individual’s lived experience; for instance, one of the consequences of the previous stay-at-home orders is that some individuals were “trapped’ with individuals who have abused/victimized them in some way currently or in the past. This prolonged exposure, especially without opportunity for escape, is of high concern for individuals at risk especially for those who may rely on distraction and external supports as means of coping with trauma.
The Community Resilience Model (CRM) seeks to create social networks of community members mutually supporting each other through chronic stress and/or trauma exposures. This is a skills-based approach aimed at stabilization of physiological stress responses. An additional focus of CRM is to create “trauma-informed” and “resilience-focused” communities. The CRM was highlighted in the United Nations Common Guidance on Helping Build Resilient Societies guide.5
The ASERT Collaborative engaged community partners to explore how CRM could be adapted to meet the needs of the neurodivergent community in these unprecedented times. Stakeholders included representatives from the Office of Developmental Programs and Office of Mental Health and Substance Abuse Services in the project formation phase. Key stakeholder mapping was conducted with input from self-advocacy agencies (SAU-1 and the Acres Project); family members/natural supports of neurodivergent individuals; and professionals who support neurodivergent individuals including direct support professionals and licensed/managerial professionals. These were the four target stakeholder groups for this effort.
The initial effort for this project was a Project ECHO © clinic aimed at licensed professionals who supervise direct support professionals and neurodivergent individuals. Project ECHO (Extension for Community Healthcare Options) is a hub and spoke model where “all teach and all learn” in a collaborative environment based largely on case-based learning. Project ECHO has been demonstrated to be an effective means of building skills for community service providers working with neurodivergent individuals.6,7 This particular series focuses on trauma and stress responses in neurodivergent individuals. Brief lectures provide an overview of the CRM as well as adaptations which may be helpful for neurodivergent individuals. The main thrust of the sessions come from participants who present de-identified cases to each other and the specialist team in order to gain confidence and competence in providing evidence-based supports to increase resilience for neurodivergent adults.
The “hub team” consists of individuals from a variety of backgrounds with content expertise—the hub team for this effort include community providers, an autistic adult, and members of the ASERT clinical team. The “spokes” consist of community health care providers—in this case community-based service providers supporting neurodivergent individuals. To date, 32 community providers have participated in the Fostering Resilience for Neurodiverse Communities ECHO series.
Community Coalition Action review for ECHO
1. Know the community: ASERT has extensive experience engaging key stakeholder groups in the neurodivergent community. The ECHO team at Penn State University brought additional expertise in marketing and recruiting participants. Self Advocates United as 1and the Acres Project provided feedback on topics, materials, and enriched with lived experience perspectives.
2. Establish positions and strategies: Partners determined that increasing evidence-based community approaches for building resilience was of key importance and achieving buy-in from managers and supervisors at community agencies was an important first step. Project ECHO’s emphasis on case-based learning and wide inclusion/diversity of the hub team members are in alignment with the principle of incorporating lived experience to promote optimal outcomes. Materials are in development which will cover the same material in self-paced online learning experiences allowing the other targeted stakeholders to access the materials in ways and times which are optimal for them. A true community-based approach can be achieved where all key stakeholders share the same information and support one another.
3. Build and sustain networks: Information from the ECHO project has been shared in a variety of ODP sponsored networks including newsletters and listservs as well as presentations at the Everyday Lives Dual Diagnosis Conference, and ODP Capacity Building Institute. Past ECHO participants have shared their experiences in testimonials and with colleagues. Subsequent cohorts of ECHO participants have become easier to recruit reflecting greater awareness and interest in the project.
4. Mobilize constituencies: Collaboration with SAU-1, Acres Project and other key community partners remain active as new directions for the work are considered leading to overall goal of increased capacity for evidence-based trauma resilience building for neurodivergent individuals at all levels of disability. Access to new materials on the learning platforms and ECHO updates will help to sustain active engagement.
Summary
Community engagement requires time, effort, and careful consideration. It is an active and dynamic process which necessitates careful planning and continual reassessment. Community partners need to make effort to understand the unique perspectives and powerful lived experience that each can provide. True community engagement where partners are truly sharing in the governance of the work has the potential to create powerful and immediately impactful work. The ASERT Collaborative’s recent experience with the TRAIN and ECHO projects are testament to this.
The research and development phase of TRAIN was funded by PA Department of Human Services, Office of Development Programs Money Follows the Person (MFP) funding. The implementation phase of TRAIN receives ASERT funding and support.
Project ECHO: Fostering Resilience is funded by the PA Department of Human Services, Office of Development Programs Money Follows the Person (MFP) funding.
References
1. Centers for Disease Control and Prevention Principles of community engagement (1st ed ) Atlanta (GA): CDC/ATSDR Committee on Community Engagement; 1997
2. National Academy of Medicine: Organizing Committee for Assessing Meaningful Community Engagement in Health & Health Care Programs & Policies. 2022. Assessing Meaningful Community Engagement: A Conceptual Model to Advance Health Equity through Transformed Systems for Health. NAM Perspectives. Commentary, National Academy of Medicine, Washington, DC. https://doi.org/10.31478/202202c
3. Butterfoss FD, Kegler MC. The community coalition action theory. In: DiClemente RJ, Crosby RA, Kegler MC (editors). Emerging theories in health promotion practice and research (2nd ed., pp. 237-276). San Franc cisco: Jossey-Bass; 2009.
4. Pennsylvania Department of Human Services, Office of Developmental Programs, ADULT PROTECTIVE SERVICES (APS) ANNUAL REPORT Fiscal Year 2020-2021; https://www.dhs.pa.gov/about/Fraud-And-Abuse/Documents/APS-Annua_Report_FY_20-21.pdf
5. United Nations (2020), United Nations Common Guidance on Helping Build Resilient Societies, New York (UN) https://unsdg.un.org/sites/default/files/2021-09/UN-Resilience-Guidance-Final-Sept.pdf
6. Dreiling, N. G., Cook, M. L., Lamarche, E., & Klinger, L. G. (2021). Mental health project echo autism: Increasing access to community mental health services for autistic individuals. Autism, 26(2), 434–445. https://doi.org/ 10.1177/13623613211028000
7. Komaromy, M., Ceballos, V., Zurawski, A. et al. Extension for Community Healthcare Outcomes (ECHO): a new model for community health worker training and support. J Public Health Pol 39, 203–216 (2018). https://doi.org/10.1057/ s41271-017-0114-8
Biography
Michael Murray is a board-certified child and adolescent psychiatrist. He is the director of the Division of Autism Service at Penn State College of Medicine and the medical director of the Autism and Developmental Disabilities Clinic for Penn State Health. He is the director of the Central Region ASERT collaborative.
Andrea Layton is a board-certified behavior analyst. She is the assistant director for the Central Region ASERT collaborative. She directs the ASERT training, communication, and outreach missions.
Jeanne Logan is certified registered nurse practitioner. She is the associate clinical director for the Division of Autism Services for Penn State Health.
Contact Information
Michael Murray
Penn State College of Medicine
Department of Psychiatry and Behavioral Health
Division of Autism Services
Central Region ASERT Collaborative
mmurray2@pennstatehealth.psu.edu
Andrea Layton
Penn State College of Medicine
Department of Psychiatry and Behavioral Health
Division of Autism Services
Central Region ASERT Collaborative
alayton@pennstatehealth.psu.edu
Jeanne Logan
Penn State Health
Certified Nurse Practitioner
717-531-8338