Positive Approaches Journal, Volume 12, Issue 2
| Site: | My ODP |
| Course: | My ODP |
| Book: | Positive Approaches Journal, Volume 12, Issue 2 |
| Printed by: | |
| Date: | Sunday, August 2, 2026, 9:07 PM |
Positive Approaches Journal | 6-7

Volume 12 ► Issue 2 ► August 2023
Understanding the Complexities of Behavioral Phenotypes and How to Support People
Introduction
The term phenotype comes to us from the study of genetics and refers to observable traits, such as height, eye color and blood type. A person’s phenotype is determined by both their genetic makeup, which is called their genotype, and by environmental factors.1 Just as physical traits are shaped by the interplay of genetic factors and the environment, so too can such factors influence an individual’s tendencies in interactions, responses, and personality traits. These characteristic patterns of social, linguistic, cognitive, and motor observations consistently associated with a biological or genetic conditions are sometimes referred to behavioral phenotypes.2
This issue of the Positive Approaches Journal shares insights from several expert and skilled clinicians into biological and genetic conditions which have been associated with behavioral phenotypes, including fetal alcohol spectrum disorder, autism, and Down syndrome (trisomy 21). The field of intellectual and developmental disabilities in general has recognized the associated characteristic patterns referenced above for various conditions long before the term behavioral phenotype, or even the modern understanding of genetics, was developed. Those familiar with the historical aspects of the field are well aware that past attempts to characterize patterns in those with conditions or syndromes at times contributed to mischaracterizations and to damaging stereotypes of individuals.
Great progress in scientific understanding, due in part to the remarkable Human Genome Project, along with rigorous research, and an ever-increasing focus on person-centered approaches has brought forward new understanding to use in supporting and serving individuals with intellectual disabilities and autism. Any description of behavioral phenotypes must always be considered in context. Supporters must always remember that behavioral phenotypes describe “characteristic patterns” or tendencies. These do not describe the individuals themselves nor define the individuals’ true capabilities or limits to their potential. At best, this knowledge becomes a tool to help support an individual and to help promote their own pathway forward in achieving an Everyday Life.
On behalf of the Office of Developmental Programs and the Office of Mental Health and Substance Abuse Services, the editorial board of the Positive Approaches Journal thanks you for your interest. We welcome your comments and feedback.
Gregory Cherpes MD,
NADD-CC
Medical Director
Office of Developmental
Programs
References
2. O'Brien, G. (2006). Behavioural phenotypes: Causes and clinical implications. Advances in Psychiatric Treatment, 12(5), 338-348. doi:10.1192/apt.12.5.338
Positive Approaches Journal | 8-11
Volume 12 ► Issue 2 ► August 2023
Data Discoveries
The goal of Data Discoveries is to present useful data using new methods and platforms that can be customized.
Autism is a complex neurodevelopmental disorder that presents with a wide range of behavioral and social communication differences. Behavioral phenotyping in autism refers to the systematic observation and characterization of a person's behavior and cognitive traits related to autism.1 Behavior phenotyping aims to identify and describe the specific patterns of behavior that are commonly associated with autism. Behavior phenotyping includes various methods and tools to assess and categorize different aspects of an individual's behavior including direct observations, parent/care partner interviews, standardized questionnaires, and other behavioral measures.2 Some primary objectives of behavior phenotyping in autism are:
1. Diagnostic Classification: Behavior phenotyping helps in the process of diagnosing autism. By identifying and analyzing specific behavioral patterns and characteristics, clinicians can determine whether an individual meets diagnostic criteria.3
2. Understanding Variability: Autism is a spectrum disorder, meaning that it presents differently in each person. Behavior phenotyping helps researchers and clinicians understand the vast variability in autism traits, like social interaction difficulties, repetitive behaviors, and communication differences.4
3. Research: Behavior phenotyping allows researchers to study the relationship between specific behaviors and underlying neurological, genetic, or environmental factors, which can contribute to a better understanding.5
It's important to note that behavior phenotyping is just one tool for diagnosing and understanding autism. Comprehensive autism evaluations often involve a multidisciplinary approach, including assessments by psychologists, speech therapists, occupational therapists, and other professionals to capture the full range of an individual's strengths and needs.6
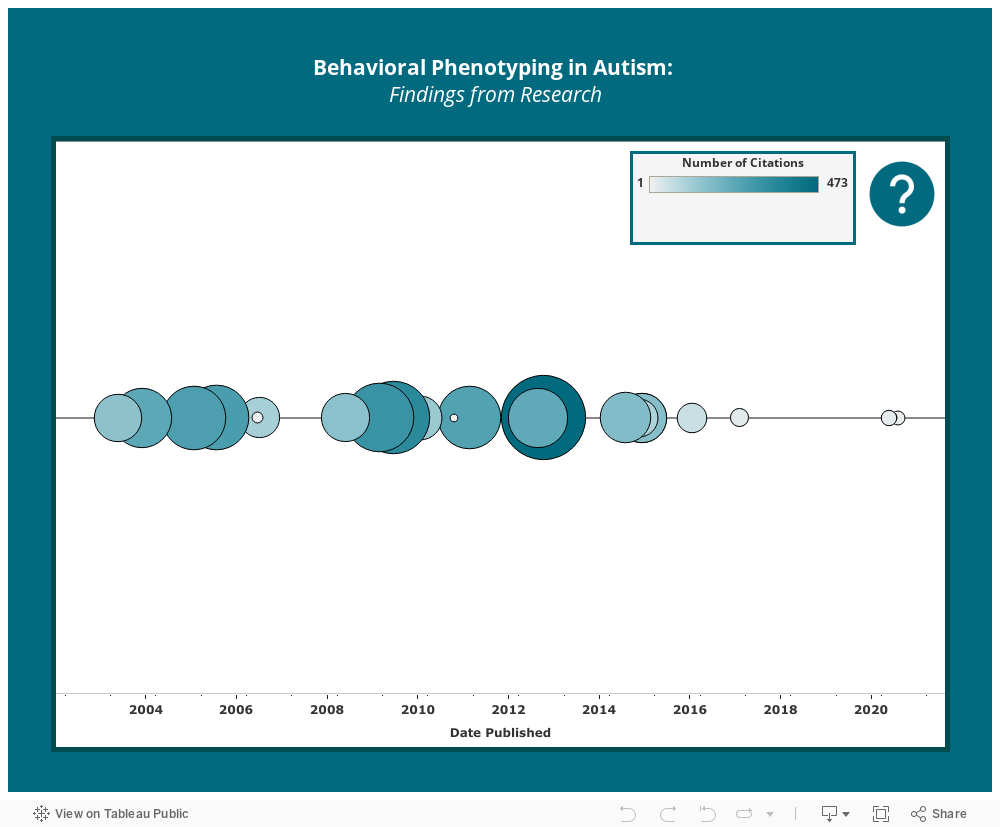
The data dashboard presented below provides an overview of peer-reviewed research on behavior phenotyping in autism. The dashboard displays a timeline of publications related to behavior phenotyping in autism, categorized by year. Each publication is represented by a circle, and the size and color of the circle indicate the frequency of citations received from other research, reflecting the publication's impact and reach. To access the abstract and potential full-text options for each article, simply click on the respective circle.
Conclusion
The Autism Services, Education, Resources, and Training Collaborative (ASERT) offers a robust array of resources related to autism across the lifespan and spectrum. To learn more about diagnosing autism and what an evaluation entails, access these resources created by ASERT: Understanding Autism Evaluations and What to Expect in an Autism Evaluation. You can also access the Support Professional Resources collection to learn more about the characteristics of autism and how it may look in individuals, presented in a way that is relevant and accessible to direct support professionals.
References
1. Larner O, Roberts J, Twiss J, Freeman L. A Need for Consistency in Behavioral Phenotyping for ASD: Analysis of the Valproic Acid Model. Autism Research and Treatment. 2021;2021:8863256-10. doi:10.1155/2021/8863256
2. Carpenter KLH, Hahemi J, Campbell K, et al. Digital Behavioral Phenotyping Detects Atypical Pattern of Facial Expression in Toddlers with Autism. Autism research. 2021;14(3):488-499. doi:10.1002/aur.2391
3. Sarmiento J-AR, Naval Jr P. Behavioral Phenotyping for Autism Spectrum Disorder Biomarkers Using Computer Vision. Journal of Image and Graphics. 2020:47-52. doi:10.18178/joig.8.2.47-52
4. Schwartzman BC, Wood JJ, Kapp SK. Can the Five Factor Model of Personality Account for the Variability of Autism Symptom Expression? Multivariate Approaches to Behavioral Phenotyping in Adult Autism Spectrum Disorder. Journal of autism and developmental disorders. 2016;46(1):253-272. doi:10.1007/s10803-015-2571-x
5. Cheroni C, Caporale N, Testa G. Autism Spectrum Disorder at the Crossroad between Genes and Environment: Contributions, Convergences, and Interactions in ASD Developmental Pathophysiology. Molecular autism. 2020;11(1):1-18. doi:10.1186/S13229-020-00370-1
6. Steiner AM, Goldsmith TR, Snow AV, Chawarska K. Practitioner’s Guide to Assessment of Autism Spectrum Disorders in Infants and Toddlers. Journal of autism and developmental disorders. 2012;42(6):1183-1196. doi:10.1007/s10803-011-1376-9
Stephens & Roseman | 12-24
Volume 12 ► Issue 2 ► August 2023
Interdisciplinary Care for Adults with Down Syndrome and Autism – Practical Considerations and a Brief Literature Review
Mary M Stephens, MD, MPH, Karin Roseman, LCSW
Abstract
Individuals with Down syndrome are at an increased risk of a co-occurring diagnosis of autism (DS-ASD), although this has only been recently recognized. In this article, we will focus on a brief literature review and practical care considerations for adults with DS-ASD to maximize life-long well-being that may help patients, caregivers, and health care professionals work better together.
Individuals with Down syndrome (DS), caused by an extra copy of the twenty-first chromosome, are known to be at higher risk for a co-occurring diagnosis of autism (DS-ASD) (Hamner et al., 2020). Given the challenges in making the diagnosis of autism in this patient population, the diagnosis is often made later than in individuals with autism alone (Bull 2020). For young adults and their families and caregivers, this can be a very challenging time as there are far fewer resources readily available for adults. In this review, we will focus on transition to adult care models for individuals with DS-ASD and review common physical and mental health concerns. We will also briefly review the diagnosis of Down syndrome regression disorder (DSRD) as this emerging diagnosis has been described as the development of autistic-like features in teens and young adults with DS but is distinct from DS-ASD.
Transition to adult health care for people with DS-ASD is often a challenging time. Loss of school-based services, transitions to new medical providers, and changes to insurance benefits – often resulting in loss of wraparound behavioral health supports – have been likened to “falling off a cliff” (Steinway et al., n.d.). While evidence around health care transition for adults with DS-ASD is limited, it suggests that transition can be challenging and the gaps in services available lead some young adults with complex healthcare needs straddling the line between pediatric and adult systems (VanZant & McCormick, 2021; Varshney et al., 2022).
For young adults with DS-ASD this can be both an exciting and challenging time, a time for skill acquisition, development, and a desire for independence. Without demands of school and rigid scheduling some young adults thrive. There can still be downsides and challenges to parents and caregivers who have relied on consistency of services and schedules for so long, however.
In the adult healthcare system, primary care doctors may be more comfortable in managing some medical co-morbidities than pediatricians. When considering transition, think about primary care first. People with well controlled Celiac may not need an adult gastroenterologist, thyroid medication may not require endocrinology, and some adult primary care physicians may even be comfortable managing medications for anxiety, depression, and complex behavioral health needs, at least until an adult psychiatrist can be identified. Got Transition, a federally funded national resource center on health care transition from pediatric to adult care, offers tools for patients, caregivers, and providers to help navigate this transition. Resources can be accessed at www.gottransition.org (GotTransition.org, n.d.).
When making the transition to the new healthcare provider, try to engage some of these strategies for success:
- Does the patient do better with discussing the health history first or proceeding directly to the physical exam?
- Does the patient need to be present for the entire visit? While even for a telehealth appointment the patient needs to be present for some portion of the visit, can they leave after the physical portion while the paperwork and counseling is done? While certainly we want the patient to be engaged and learn new skills in the healthcare setting and the healthcare provider to talk/communicate with them directly, an incremental approach may work better for all involved. For example, does the visit have to start with vital signs if blood pressure is particularly challenging for the patient?
- Focus on the comfort of the patient – Do headphones, fidgets, taking a walk, listening to music, or stimming help the patient stay calm and focused and able to participate in the visit? Let the provider know when these behaviors are “ok” or when they mean the patient is starting to show signs of distress, and it’s time to shift gears or end the visit.
- Prioritize what needs to be accomplished in the visit and what can wait. Practical experience suggests that recovering from a “bad” encounter with a patient takes a lot longer than ending a visit early and trying on a better day, different time of day or via telehealth.
- Allow time for processing and communication and remember to charge up communication devices and bring them to the visit if they help the patient. If the diagnosis of DS-ASD was made later, has use of an augmentative and alternative communication system been considered?
Remember, not only is this health care provider new to you, but you are new to them too!
While it is important to share information specific to DS-ASD with the new provider, especially if they have limited experience in this area, it is important for providers to be cautious about diagnostic overshadowing. Healthcare providers should think broadly, and not attribute all symptoms or behaviors to DS-ASD. Especially when seeing a patient with new or troubling behaviors, think about a top to toe approach.
Looking at the healthcare experiences of those with ASD and intellectual disability, individuals with DS may be at greater risk for health problems than expected based on their age and specifically have a higher risk of seizure disorders, autoimmune conditions, sleep disorders, gastrointestinal conditions, and heart disease (Bishop-Fitzpatrick & Rubenstein, 2019). It’s unclear in terms of heart disease if the relatively protective benefit of having Down syndrome protects against the increased heart disease risk. Barriers to care cited by adult autistics with and without disabilities include fear and anxiety, need for additional processing time, sensory issues and difficulty communicating with health care providers. (Raymaker et al., 2017)
Based on adult guidelines for individuals with DS, routine screening in this age group should include thyroid bloodwork (TSH) every 1 – 2 years. Screening for diabetes, typically a blood test called an HbA1c, should begin in the 20s for those with risk factors and be repeated every 2 – 3 years. For those without risk factors such as overweight or obesity, consider starting in the 30s. Monitor for signs of celiac disease (loose stools, cramping and constipation) and screen with blood tests if they are present. (Tsou et al., 2020)
Evidence-based reviews from the Down Syndrome Medical Interest Group-USA (DSMIG-USA) adult health work group focus on additional areas of importance for the care of adults with DS and include (G. Capone et al., 2020; G. T. Capone et al., 2018):
- While the risk of atlanto-axial and hip instability decreases over time, there may be an increased risk of early neck and hip arthritis that clinicians should be aware of.
- The risk of hearing impairment approaches 70% in adults with DS, and there is an ongoing need for testing, treatment, and speech therapy.
- While we have a lot to learn about overweight and obesity, the 20s can be a particularly challenging time for young adults with DS and patients and caregivers need to think about strategies to mitigate this. In practical terms, what non-food rewards can be put in place to support positive behaviors, who is tracking what the young adult with DS eats in the community with support staff? How can we best partner with patients to educate them and help foster healthy nutritional choices? How can we promote enjoyable physical activity?
- As young adults age out of pediatric systems and caregivers may shift from parents to siblings or staff, patients need to continue to be monitored based on established guidelines for congenital heart disease and/or acquired heart valve disorders. It’s important to ensure that medical history in general transitions with the patient, and new caregivers are aware of prior diagnoses and treatments.
- Dysphagia or trouble swallowing remains more common in adults with DS along with reflux/GERD. Families and caregivers should alert the medical team about coughing or other mealtime symptoms, spit ups, new tooth grinding, or recurrent pneumonia.
- Referral to speech and occupational therapy may be a consideration although one might have to look a little harder to find adult therapists with the skills to meet the needs of the patient.
- Adults with DS remain at increased risk of sleep apnea (OSA). Although no formal screening guidelines exist for adults, symptoms of OSA can include both symptoms related to sleep like snoring and gasping and daytime symptoms including irritability, decline in performance and daytime sleepiness. Home sleep studies that feel less intrusive to patients may be an option to consider for making the diagnosis. Modalities other than CPAP or Bipap are emerging, such as the hypoglossal nerve stimulator that may make treatment a possibility for adults with DS-ASD when it was not before.
Other considerations:
Dementia
Early Dementia is common in DS and routine screening is recommended to begin at age 40 using the National Task Group – Early Dementia Screening Detection (NTG-EDSD) tool. Though some experts recommend screening as early as age 35, symptoms of cognitive decline before the age of 40 are unlikely to represent dementia and other causes should be thoroughly investigated. Even with a decline after the age of 40, other co-morbidities should be ruled out – think UTI, Vitamin B12 deficiency, hearing and vision loss, polypharmacy, and mood disorders such as depression, anxiety, and OCD. In individuals with DS-ASD also consider things that may be more common to them specifically such as hidradenitis or yeast infections of groin or armpits or constipation.
Down syndrome regression disorder
Historically described by some as late onset autism in individuals with DS, Down syndrome regression disorder (DSRD) is now felt to be a distinct clinical entity (Rosso et al., 2020). Previously described as DS disintegrative disorder or unexplained regression in DS, it occurs in individuals with DS between approximately 10 – 30 years of age (Santoro et al, 2022 and Rosso et al., 2020). Features of DSRD include a subacute loss of skills across multiple domains (language, communication, cognition, executive function, and behavioral and adaptive skills) (Santoro et al., 2022). New onset stereotypies such as rocking, hand-flapping, and waving and other autistic features, are hallmarks of DSRD (Santoro et al., 2022).
DSRD is a distinct disorder from autism, however, and efforts are underway to create more explicit diagnostic criteria and to better understand the etiology and optimal course of treatment. Neuroimmunology dysfunction is one hypothesis being explored given evidence in some cases of responsiveness to intravenous immunoglobulin (IVIG) (Santoro et al., 2022). The role of psychological stress, while commonly identified in individuals with DSRD, is unclear (Rosso et al., 2020).
Making the diagnosis in adults and behavioral health considerations
As the increased risk of autism in individuals with Down syndrome has only been more recently recognized, young and middle-aged adults with DS may not have been diagnosed in childhood. Caregivers and healthcare professionals should consider this diagnosis, particularly in individuals who struggle with communication and challenging behaviors. A retrospective review of developmental history, observations in school and the community, and reports from family, caregivers, and therapists may support the diagnosis. Formal diagnostic or neuropsychological testing may be harder to find in adult healthcare systems, but potential resources include Down syndrome clinics, offices of vocational rehabilitation, autism centers of excellence, and academic medical centers. While the absence of a diagnosis of autism should not preclude clinicians from addressing communication challenges or behavioral issues, a formal diagnosis may be worthwhile pursuing as it may open the door to additional services and help individuals with DS-ASD get the care and support they need.
Consider these behavioral approaches to treatment (McGuire, D. E., & Chicoine, B. (2021):
- Applied behavior analysis or ABA has been shown to be effective in teaching skills to people with autism and all sorts of developmental disabilities. ABA uses a variety of techniques to shape a person’s behavior and is rooted in the idea that rewards and consequences can teach specific and measurable skills.
- Help with sensory issues by engaging support from a trained Occupational Therapist to complete a sensory integration assessment.
- Provide structure and consistency through routines, pictures or visual cues and schedules, and consistency in the way tasks are done.
- Transitions from one activity to another can be challenging; be sure to provide warnings and explanation when it is time to transition.
- Utilize social stories to teach about social situations and learn new social skills.
- Prevent information overload, provide time for processing of information and present information in a concrete form (such as pictures).
- Medications are sometimes also used to help manage challenging behaviors such as aggression and self-injurious behaviors.
Putting it all together: A case study
In the case of a 32-year-old male with DS-ASD, the parent came in with concerns for change in functioning over the course of 1-2 years. Per parent (who – of note – is a psychologist) changes have been a subtle and gradual functional decline. Parent reported that she has taken a lot of care for patient’s mental health and feels there is a biological cause. During the patient’s visit mom expressed concerns for patient’s locomotor functioning, particularly in navigating curbs and stairs, increased isolation and self-talk, increased perseveration and rigidity, and sleep concerns.
Based on these concerns and physical exam, patient was referred for additional medical workup including x-rays, and follow up with ENT/Audiology and Sleep Medicine. X-Rays were recommended due to gait abnormality and a small left knee effusion. Patient was also found to have right-sided acute serous otitis media and started on Prednisone, as well as referred to ENT/Audiology. His hypersomnia was the impetus for a referral to sleep medicine. In addition to these medical follow ups, his behavioral health medication was adjusted. It was discussed with the parent that symptoms were likely multifactorial but not likely related to Dementia given his age.
Take Home Points: Adult Care
Don’t forget to consider that the diagnosis of autism may have been missed in individuals with DS during childhood and making the diagnosis can lead to better support and care of the individual.
Adults with DS-ASD may benefit from adaptions in the medical visit, but don’t forget that they are still capable of learning and may acquire new skills over time such as being able to tolerate blood draws and immunizations without drama or sedation. As they age, however, expectations may also need to change if there is a functional decline. Consider the use of telehealth as a way to allow adults to better access care and allow for 1:1 time for both patients and caregivers.
As technology has advanced, and especially if DS-ASD has been unrecognized earlier in childhood, consider evaluation or re-evaluation for assistive technology to decrease communication barriers and foster independence.
Primary care providers may be able to prescribe psychotropic medications if necessary to help address challenging behaviors in addition to recommending other therapeutic modalities.
As individuals with DS-ASD age, they may face transitions in caregivers as well as functional decline. It’s important for families and non-family caregivers to communicate and plan for these inevitable changes in order to best support the individual with DS-ASD.
References
1. Academic Autism Spectrum Partnership in Research and Education – Academic Autism Spectrum Partnership in Research and Education. (n.d.). Retrieved February 4, 2023, from https://aaspire.org/
2. Alzheimer’s Disease & Down Syndrome. (n.d.). Retrieved February 4, 2023, from https://ndss.org/resources/alzheimers
3. Bishop-Fitzpatrick, L., & Rubenstein, E. (2019). The Physical and Mental Health of Middle Aged and Older Adults on the Autism Spectrum and the Impact of Intellectual Disability. Research in Autism Spectrum Disorders, 63, 34–41. https://doi.org/10.1016/j.rasd.2019.01.001
4. Capone, G., Stephens, M., Santoro, S., Chicoine, B., Bulova, P., Peterson, M., Jasien, J., Smith, A. J., & Workgroup, D. S. M. I. G. (DSMIG-U. A. H. (2020). Co-occurring medical conditions in adults with Down syndrome: A systematic review toward the development of health care guidelines. Part II. American Journal of Medical Genetics Part A, 182(7), 1832–1845. https://doi.org/10.1002/ajmg.a.61604
5. Capone, G. T., Chicoine, B., Bulova, P., Stephens, M., Hart, S., Crissman, B., Videlefsky, A., Myers, K., Roizen, N., Esbensen, A., Peterson, M., Santoro, S., Woodward, J., Martin, B., Smith, D., & Workgroup, for the D. S. M. I. G. D.-U. A. H. C. (2018). Co-occurring medical conditions in adults with Down syndrome: A systematic review toward the development of health care guidelines. American Journal of Medical Genetics Part A, 176(1), 116–133. https://doi.org/10.1002/ajmg.a.38512
6. Down Syndrome and Alzheimer’s Disease. (n.d.). Alzheimer’s Disease and Dementia. Retrieved February 4, 2023, from https://alz.org/alzheimers-dementia/what-is-dementia/types-of-dementia/down-syndrome
7. GotTransition.org. (n.d.). Got Transition®. GotTransition.Org. Retrieved February 4, 2023, from https://www.gottransition.org/
8. Iulita, M. F., Garzón Chavez, D., Klitgaard Christensen, M., Valle Tamayo, N., Plana-Ripoll, O., Rasmussen, S. A., Roqué Figuls, M., Alcolea, D., Videla, L., Barroeta, I., Benejam, B., Altuna, M., Padilla, C., Pegueroles, J., Fernandez, S., Belbin, O., Carmona-Iragui, M., Blesa, R., Lleó, A., … Fortea, J. (2022). Association of Alzheimer Disease With Life Expectancy in People With Down Syndrome. JAMA Network Open, 5(5), e2212910. https://doi.org/10.1001/jamanetworkopen.2022.12910
9. Jenny’s Diary. (n.d.). Learning (Intellectual) Disability and Dementia. Retrieved February 4, 2023, from https://www.learningdisabilityanddementia.org/jennys-diary.html
10. McGuire, D. E., & Chicoine, B. (2021). Mental wellness in adults with Down Syndrome: A guide to emotional and behavioral strengths and challenges. Woodbine House.
11. Moore, C. M., Pan, C. X., Roseman, K., Stephens, M. M., Bien-Aime, C., Morgan, A. C., Ross, W., Castillo, M. C., Palathra, B. C., Jones, C. A., Ailey, S., Tuffrey-Wijne, I., Smeltzer, S. C., & Tobias, J. (2022). Top Ten Tips Palliative Care Clinicians Should Know About Navigating the Needs of Adults with Intellectual Disabilities. Journal of Palliative Medicine, 25(12), 1857–1864. https://doi.org/10.1089/jpm.2022.0384
12. Muccilli, K. (n.d.). Health Care for Adults with Intellectual and Developmental Disabilities: Toolkit for Primary Care Providers. Retrieved February 4, 2023, from https://iddtoolkit.vkcsites.org/
13. NTG-EDSD Screening Tool | Dementia and ID or DD | The NTG. (n.d.). NTG 2022. Retrieved February 4, 2023, from https://www.the-ntg.org/ntg-edsd
14. Raymaker, D. M., McDonald, K. E., Ashkenazy, E., Gerrity, M., Baggs, A. M., Kripke, C., Hourston, S., & Nicolaidis, C. (2017). Barriers to healthcare: Instrument development and comparison between autistic adults and adults with and without other disabilities. Autism: The International Journal of Research and Practice, 21(8), 972–984. https://doi.org/10.1177/1362361316661261
15. Steinway, C., Gable, J., & Jan, S. (n.d.). TRANSITIONING TO ADULT CARE:
16. Tsou, A. Y., Bulova, P., Capone, G., Chicoine, B., Gelaro, B., Harville, T. O., Martin, B. A., McGuire, D. E., McKelvey, K. D., Peterson, M., Tyler, C., Wells, M., Whitten, M. S., & Global Down Syndrome Foundation Medical Care Guidelines for Adults with Down Syndrome Workgroup. (2020). Medical Care of Adults With Down Syndrome: A Clinical Guideline. JAMA, 324(15), 1543–1556. https://doi.org/10.1001/jama.2020.17024
17. VanZant, J. S., & McCormick, A. A. (2021). Health care transition for individuals with Down syndrome: A needs assessment. American Journal of Medical Genetics Part A, 185(10), 3019–3027. https://doi.org/10.1002/ajmg.a.62403
18. Varshney, K., Iriowen, R., Morrell, K., Pillay, P., Fossi, A., & Stephens, M. M. (2022). Disparities and outcomes of patients living with Down Syndrome undergoing healthcare transitions from pediatric to adult care: A scoping review. American Journal of Medical Genetics. Part A, 188(8), 2293–2302. https://doi.org/10.1002/ajmg.a.62854
Biographies
Dr. Mary Stephens is an Associate Professor in Family and Community Medicine at Jefferson. She is a family physician with 25+ years of experience in patient care and teaching. In 2018, she returned to Jefferson to help launch a new primary care model for teens and adults with complex childhood onset conditions.
Karin Roseman is a licensed clinical social worker with over 10 years of experience working with children and adults with complex medical needs. Prior to joining the Jefferson team in 2021, she worked as a care coordinator for a large Medicaid managed care plan in Philadelphia, providing support to Medicaid members with complex medical needs, advocating to the plan to ensure that they received the services and medical care that they needed.
Contact Information
Mary M. Stephens, MD, MPH
Thomas Jefferson University, Department of Family and Community Medicine
VanEerden | 25-42
Volume 12 ► Issue 2 ► August 2023
Fetal Alcohol Spectrum Disorder Effects on
Communication, Learning, and Behavioral Health
Robin VanEerden, MS, LPC, NADD-DDS, CC
Fetal Alcohol Spectrum Disorder (FASD) is a non-diagnostic umbrella term used to describe a group of diagnoses related to prenatal alcohol exposure. This group includes Fetal Alcohol Syndrome (FAS), Partial Fetal Alcohol Syndrome (pFAS), and Alcohol Related Neurodevelopmental Disorder (ARND) (CDC, 2004). Fetal Alcohol Syndrome is a medical diagnosis, and it is the only syndrome under the FASD umbrella that can be diagnosed without confirmed maternal drinking (Streissguth, 2007). Alcohol puts the developing fetus at risk due to the interference of developing cells within the central nervous system.
FASD is the leading preventable cause of intellectual disabilities. While influenced by maternal nutrition, timing, frequency, and amount of alcohol exposure (Maier & West, 2001), FASD can happen to any fetus that comes into contact with alcohol while in utero. The only known cause of FASD is maternal drinking while pregnant. In the United States, by 1996 FAS was estimated to affect 1-3 live births per 1,000 (Stratton et la., 1996). By 2009 FASD was estimated to affect almost 1 out of 100 newborns in the United States each year (May & Gossage, 2001; May, et al., 2009). Currently, the estimated prevalence of fetal alcohol spectrum disorders (FASD) is conservatively around 1%; of the US population however, a recent study in North America found rates as high as 5 % of the school-age population affected by prenatal alcohol exposure, indicating a significant public health concern (May et al., 2014; May et al., 2015). While there have been considerable efforts in the public health sector to reduce drinking during pregnancy (Grant et al., 2004), there has not been a meaningful decrease in prenatal alcohol exposure over the past decade (Thomas, Gonneau, Poole, & Cook, 2014). Approximately half of all pregnancies are unplanned and the rates of drinking during childbearing age are substantial; thus, there is ongoing risk of having children born who are affected by prenatal exposure to alcohol (Finer & Zolna, 2011; Green, McKnight-Eily, Tan, Mejia, & Denny, 2016). The effects of this brain-based physical disorder can be life-long (from birth to death) and are influenced by access to effective services and supports. With effective supports, more positive life outcomes are possible. There are many children and adults who are living with the effects of FASD but have not been formally diagnosed or identified. This does not change the fact that their day-to-day lives may be impacted (Grant, Brown, Dubovsky, Sparrow, & Ries, 2013). In addition, Kara N. Thomas et.al, have recognized that FASD has not been thoroughly explored regarding the paternal contribution to the spectrum disorder. Using a physiologically relevant mouse model,
the studies are the first to demonstrate that male drinking is a plausible yet completely unexamined factor in the development of alcohol-related craniofacial abnormalities and growth deficiencies. The study demonstrates the critical need to target both parents in pre-pregnancy alcohol messaging and to expand epidemiological studies to measure the contributions of paternal alcohol use on children’s health (K. Thomas et.al 2023)
In Pennsylvania, an FASD Task Force was first convened in
2006. The Task Force is comprised of representatives from numerous stakeholder
groups including physicians, state agency representatives, service providers,
and parents and family members.
The initial product of the FASD Task Force, The Pennsylvania Fetal Alcohol
Spectrum Disorders Action Plan, released in 2008, provided “a plan of action to
address the very serious issue of birth defects caused by prenatal alcohol
exposure.”
The FASD Task Force was reactivated in 2015, with a broader mission: To help establish a system of care for FASD in PA that raises awareness of FASD, prevents FASD, and provides services and supports to individuals of all ages impacted by FASD and their families. Current Task Force goals include:
- Creation of a dedicated, consumer-led entity to promote prevention and support affected individuals and families.
- Broadly-based workforce training on FASD identification and interventions.
- Establishment of eligibility for Early Intervention services for children with an established or suspected FASD.
- Prevention and intervention of FASD
- Awareness: Increase awareness of FASD and its symptoms.
- Data: Collect, interpret, and disseminate information on FASD.
- Education: Increase the knowledge of FASD within the professional community and the general population.
- Funding: Ensure adequate funding for prevention as well as services for diagnosis and intervention for children, adults and families affected by FASD.
- System: Align and improve systems of care by making FASD a statewide priority.
https://www.dhs.pa.gov/Services/Mental-Health-In-PA/Pages/FASD-Task-Force.aspx
While these are positive changes regarding this spectrum disorder, identification and diagnosis can be difficult as not all people have specific characteristic facial features or physical symptoms due to FASD. (Erb, VanEerden, 2014). However, most of the primary effects of FASD are invisible and are related to neurological (brain based) changes (Substance Abuse and Mental Health Services Administration, 2014) and to the neuroendocrine system (hormones that regulate mood, emotions, immune system, … etc.) (Uban, et al., 2011).
Primary effects include challenges with:
- executive function (planning, switching between tasks, reasoning, problem solving and navigating relationships)
- understanding and foreseeing consequences; not foreseeing danger
- memory (can be both long and short term)
- applying knowledge in different environments (generalization)
- recalling information
- regulating emotion
- being biologically unable to calm once emotionally escalated (altered stress response)
- making connections between cause and effect
- learning from mistakes
- attention deficits
- coordination
- identifying hunger, thirst (too much, too little)
- sleeping disturbances
- cognitive abilities and below average IQs
These effects can be made better or worse through support strategies, life experiences, social situations, and access to appropriate and effective services. When effects, poor supports, and stressful social situations combine, they can lead to common but not inherent characteristics. These characteristics can include problems with (Substance Abuse and Mental Health Services Administration, 2014):
- impulsivity
- disobedience/resistance/refusals
- lack of stranger awareness
- misinterpretations of social situations and social cues
- enjoying talking though the act of talking is often more important than the content
- talking about unrealistic subjects (magical thinking)
- poor judgment
- waking up in the morning
- confabulation (telling made up or misinterpreted memories about oneself or the world, without a conscious intention to deceive).
Cumulatively, these characteristics can put a person with FASD at a greater risk for:
- school/work failure
- homelessness
- employment difficulties
- substance abuse issues
- incarceration
- psychiatric confinement
(Substance Abuse and Mental Health Services Administration, 2014)
Due to the exposure of alcohol, on the developing brain and the influence of social factors, those on the spectrum may present very differently. Specific strengths and deficits need to be identified. A person may be able to read a book but be unable to process what was just read. One day memory may be intact, and recollection of task completion is apparent yet the next day these skills may not be present. Most people are incredibly friendly and caring, though they may lack important social skills which subjects them to victimization. They may desire to go to an event, but at the last minute become emotionally over aroused and refuse or decline to go. The transition may cause overwhelming emotions in relation to the environmental change. A person may not be able to manage money or balance a checkbook yet can create beautiful artwork (Erb, VanEerden 2014)
Token economies and reward systems are often ineffective interventions for persons with FASD. This is because of the difficulty with connecting cause and effect over time. Due to cognitive and auditory processing issues, even a simple conversation could be over- stimulating. The combination of an altered stress response and ineffective coping skills could cause overwhelming emotions. These uncontrolled emotions might lead to property destruction, elopement, legal issues, and other potentially dangerous behaviors [reactions]. (Erb, VanEerden, 2014).
In efforts to distribute evidence-based practices, the Substance Abuse and Mental Health Services Administration published TIP 58 A Treatment Improvement Protocol that explains in detail best practice prevention, intervention, and strategies across the life span. This article cannot possibly cover all the information listed in TIP 58, however its review is essential to work and serve people on this spectrum.
The topics that will follow are dedicated to identification, screening and strategies that are helpful to those on this spectrum.
The physical signs of Fetal Alcohol Syndrome can include a thin upper lip, flattened philtrum, shortened palpebral fissures which makes the eyes look farther apart, a shortened nose relative to the length of the midface and underdeveloped jaw. Not all children or adults exposed prenatally to alcohol will have the physical features. The neuropsychological and behavioral aspects of the spectrum disorder can include lower to average IQs, which can range from an intellectual disability to normal IQ, poor executive functioning, lack of social and communication skills, lack of motivation or initiative, poor judgement, failure to consider consequences of actions, social withdrawal, poor impulse control, intermittent anxiety. (Understanding Fetal Alcohol Spectrum Disorders (FASD) – A Comprehensive Guide for Pre-K-8 Educators (duke.edu) 2016. People on the spectrum may also appear to be oppositional, stubborn, or resistant at times. Therefore, separating what appears for example, to be oppositional or resistance to the environment can be better assessed through the lens of identifying strengths and abilities through a neuropsychological assessment. According to the Cleveland Clinic a neuropsychological assessment tests for the following:
- General intellect
- Reading/reading comprehension
- Language usage and understanding of what others say (receptive language skills)
- Attention/concentration
- Processing speed
- Learning and memory
- Reasoning
- Executive functions, which are higher-level skills used to organize and plan, manage time, problem solve, multi-task, make judgments and maintain self-control
- Visuospatial skills
- Motor speed and dexterity
- Mood and personality
With the ability to gain knowledge regarding strengths and deficits, strengths can be acknowledged and used to build self-esteem and additional skills, while deficits can be recognized and accommodated or in some cases developed.
According to Duke University FASD Guide, sophisticated brain imaging technologies are now being used to identify the structural abnormalities present in the brains of living FASD children. Magnetic Resonance Imaging (MRI) has revealed an overall reduction in brain size, confirming previous autopsy findings. However, independent of the overall reduced brain size, MRI has revealed at least four (4) major brain structures that are affected. These include: the Corpus Callosum, a large bundle of nerve fibers that connects the two hemispheres together, enabling communication between the right and left brain; the Caudate Nucleus, a structure that resides below the level of the cerebral cortex, which controls motor abilities and cognitive function; the Hippocampus, another subcortical structure, which controls the ability to store new memories and participates in spatial learning; and the Cerebellum, a structure that resides at the back of the brain, controlling motor skills, balance, and coordination. In addition to imaging structural abnormalities, other forms of brain imaging can reveal functional abnormalities within specific brain areas. For example, scientists have shown that FASD children have a delay in a certain type of electrical activity within the Parietal Cortex that is associated with information-processing. In addition, imaging techniques, such as Positron Emission Tomography (PET), can be used to study the metabolic activity of the brain (i.e., how well it is actually working). In FASD children, there is a reduction in metabolic function within the caudate nucleus as demonstrated by PET imaging. When combined with structural information from MRI studies, these studies can provide a powerful picture of the damage to specific regions within the working brain. This information can guide treatment and communication for improved outcomes. Other interventions both early and throughout the life span may include full medical examinations that follow the child in the early years to ensure healthy development, occupational therapy that would include sensory integration and processing assessments.
According to Manitoba Education, Training and Youth, “Students who are alcohol-affected often experience difficulties in processing the different sensory information they receive. For most individuals, the processing of sensory information is automatic. Most individuals can screen, filter, and selectively attend to different sensory information. However, children who are alcohol-affected often have difficulty with these processes. They may be over-responsive to some forms of sensory input and under-responsive to others. They may become overloaded by the sensory information they receive and, as a result, are unable to organize their behavior.” https://fasdsocalnetwork.org/sensory-processing/
As individuals age and life issues become more complex, therapeutic interventions may be needed. Because of processing, recall, and lack of ability to generalize information and executive functioning capabilities, it is important that counselors and other helpers are educated on FASD. Therapeutic interventions that are more effective can be effective if counselors or helping partners pair talk therapy with pictures, art, music, and possibly pet and equine therapy. These interventions can play a great role in expression of feelings and processing information in a way that is understood between the helper and the person on the spectrum. According to the CDC the following are alternative treatments that can be helpful:
- Biofeedback
- Auditory training
- Relaxation therapy, visual imagery, and meditation (especially for sleep problems and anxiety)
- Creative art therapy
- Yoga and exercise
- Acupuncture and acupressure
- Massage, Reiki, and energy healing
- Vitamins, herbal supplements, and homeopathy
- Animal-assisted therapy
There are many other “day to day” interventions and strategies needed that can make each day a more positive one for professionals, caregivers, family members and the person on the spectrum.
- Educate the entire team on FASD. This can include natural supports, family, vocational and residential supports, supports coordinators, community habilitation workers, law enforcement, primary care physicians, therapists, direct care professionals, and hospital staff.
- When developing support strategies, utilize the strengths and input of the entire team: the individual with FASD, family, friends, community supports.
- Partner with community services to ensure that people and their needs are understood.
- Make sure support plans are FASD informed, strength based, and trauma informed.
- Request assessments that may identify which area of the brain may have been affected (i.e., neuropsychological evaluation).
- Make sure that expectations for people match their ability.
- Work with a prescribing psychiatrist who is FASD informed and understands the mental health diagnoses that may co-exist with FASD.
- Accept that sometimes people can’t do a task; it is not that they won’t (and sometimes they can one day and not the next).
- Look at how to make a person’s routine more structured and predictable.
- Investigate and address sensory issues such as problems with auditory processing and visual deficits, and then implement effective strategies (i.e., sensory integration evaluation by an occupational therapist trained in sensory integration).
- Assess the environment for potential sensory issues: Is it too cluttered, loud, or crowded?
- Use labels, color codes, visual schedules, and other organizational tools.
- Use role play and modeling to teach new skills and to review acquired skills.
- Assist the person to develop healthy friendships and community supports.
- Encourage physical exercise.
- Write things down, draw pictures, and do not rely on verbal communication!
- Support persons must role play appropriate social skills and healthy choices.
- Use a coaching or mentorship model.
- Develop a Wellness Recovery Action Plan (Copeland Center, Mary Ellen Copeland).
- Develop a crisis plan.
- Develop safety plans, as necessary.
- Clearly explain expectations before, during, and after activities.
- Plan for breaks and rest periods before someone experiences emotional dysregulation.
- Use auditory cues according to developmental skill level including texting, phone reminders, egg timers, and other electronic reminders.
- Provide appropriate instruction regarding dating, sexuality, and sexually appropriate behaviors.
- Match strategies with personal strengths and personal motivation.
Fetal Alcohol Spectrum Disorders are prevalent yet, by providing appropriate intervention, people can lead more successful, productive, and happy lives.
In conclusion, this brain-based disability is invisible unless the person has physical features that can be identified. A small percentage of people who have an FASD have the all the accompanying facial features (Substance Abuse and Mental Health Services Administration, 2014). Persons are not always diagnosed with an intellectual disability, but may have severe deficits in social, communication, and vocational/educational domains. FASD does not have a socio-economic or cultural boundary. While influenced by maternal nutrition, timing, frequency, and amount of alcohol exposure, FASD can happen to any fetus that comes into contact with alcohol while in utero.
It is important to learn to understand the presentation of people with FASD. Referral to the proper community physicians including primary care physicians, psychologists, counselors, and neuropsychologists is important for the journey towards appropriate and effective supports. It is also a social responsibility to not judge and to spread the message of “0-4-9” as a preventative measure. Zero alcohol for nine months.
While those with FASD may have deficits, they also have many wonderful skills and strengths. These need to be identified to create life goals which foster self-esteem and increase motivation. Strategies and services must be friendly to people with an FASD. When strategies are not FASD friendly, problems can be made worse causing frustration, low self-image, and high stress.
References
1. Center for Disease Control and Prevention (2004). Fetal alcohol syndrome: Guidelines for referral and diagnosis. Retrieved from: http://www.cdc.gov/ncbddd/fasd/documents/fas_ guidelines_accessible.pdf
2. Doctor, S. (2013, May 23). FASD intervention strategies part I: A global approach to interventions appropriate to a person with an FASD. FASD Interventions Across the Lifespan. Webinar retrieved from: http://fasdintervention.wordpress.com/2013/05/
3. Graefe, S. (2006). Living with FASD: A Guide for Parents. Vancouver, B.C.: Groundwork Press.
4. Grant, T. M., Brown, N. N., Dubovsky, D., Sparrow, J., & Ries, R. (2013). The impact of prenatal alcohol exposure on addiction treatment. Journal of addiction medicine, 7(2), 87-95.
5. https://fasdsocalnetwork.org/sensory-processing/ last viewed 6/19/23
6. https://www.dhs.pa.gov/Services/Mental-Health-In-PA/Pages/FASD-Task-Force.aspx last viewed 6/19/23
7. Maier, S. & West, J. (2001). Drinking patterns and alcohol-related birth defects. Retrieved from: http://pubs.niaaa.nih.gov/publications/arh25-3/168-174.htm
8. Malbin, D. (2008). Fetal Alcohol Spectrum Disorders: A Collection of Information for Parents and Professionals. Portland, OR.: FASCETS, Inc.
9. May, P. A., & Gossage, J. P. (2001). Estimating the prevalence of fetal alcohol syndrome: A summary. Alcohol Research and Health, 25(3), 159-167.
10. May, P., Gossage, J., Kalberg, W., Robinson, L., Buckley, D., Manning, M., & Hoyme, H. (2009). Prevalence and epidemiologic characteristics of FASD from various research methods with an emphasis on recent in-school studies. Developmental Disabilities Research Review, 15(3),176-192.
11. May, P. A., Baete, A., Russo, J., Elliott, A. J., Blankenship, J., Kalberg, W. O., ... & Hoyme, H. E. (2014). Prevalence and characteristics of fetal alcohol spectrum disorders. Pediatrics, 134(5), 855-866.
12. Mitchell, Kathleen T. (2002). Fetal Alcohol Syndrome: Practical Suggestions and Support for Families and Caregivers. Washington, D.C.: National Organization on Fetal Alcohol Syndrome.
14. National Organization on Fetal Alcohol Syndrome: www.nofas.org
15. Paley, B. (2009). Introduction: Fetal alcohol spectrum disorders - shedding light on an unseen disability. Developmental Disabilities Research Reviews, 15, 235-249.
16. Streissguth, A. (2007). Offspring effects of prenatal alcohol exposure from birth to 25 years: The Seattle prospective longitudinal study. Journal of Clinical Psychology in Medical Settings, 14, 81-101.y
17. Substance Abuse and Mental Health Services Administration: Fetal Alcohol Spectrum Disorders Center for Excellence: http://www.fasdcenter.samhsa.gov/
18. Substance Abuse and Mental Health Services Administration. (2014). Addressing Fetal Alcohol Spectrum Disorders (FASD). Treatment Improvement Protocol (TIP) Series 58. HHS Publication No. (SMA) 13-4803. Rockville, MD: Substance Abuse and Mental Health Services Administration.
19. A Treatment Improvement Protocol (TIP); Addressing Fetal Alcohol Spectrum Disorders (FASD) TIP 58 (2014). Substance Abuse and Mental Health Services Administration Center for Substance Abuse Treatment: Rockwell, MD.
20. Uban, K. A., Bodnar, T., Butts, K., Sliwowska, J. H., Comeau, W. and Weinberg, J. (2010) Direct and Indirect Mechanisms of Alcohol Teratogenesis: Implications for Understanding Alterations in Brain and Behavior in FASD, in Fetal Alcohol Spectrum Disorder: Management and Policy Perspectives of FASD, First Edition (eds E. P. Riley, S. Clarren, J. Weinberg and E. Jonsson), Wiley-VCH Verlag GmbH & Co. KGaA, Weinheim, Germany. doi: 10.1002/9783527632510.ch5
21. Understanding Fetal Alcohol Spectrum Disorders (FASD) – A Comprehensive Guide for Pre-K-8 Educators (duke.edu) 2016 last viewed 6/19/23
22. Erb, A. and VanEerden, R. (2014) The Direct Support Workers Newsletter, Vita Community Services, Volume 3, Issue 5. Originally titled: Something Is Different Here: Promoting Awareness of an Invisible Disorder. Minor edits made from original article.
23. Erb, A. and VanEerden, R. 2014 Brief Review of Fetal Alcohol Spectrum Disorder, Applied Case Study and Discussion: The NADD Bulletin, Volume 17, Number 6.
Biography
Robin VanEerden earned her Master of Science Degree from Shippensburg University in Community Counseling and acquired her License in Professional Counseling (LPC). She has served adults with Dual Diagnosis for over 44 years. She has acquired the first ever Dual Diagnosis Certified Clinician credential awarded by the National Association for Dual Diagnosis. Robin is an Eye Movement Desensitization Reprocessing Therapist and has received a certificate in Trauma through Drexel University. Robin is the Co-chairperson of the NADD-CC committee and assisted in formulating a certification in Dual Diagnosis for clinicians (NADD-CC). Robin has served as the Clinical Director for the Commonwealth of Pennsylvania, Department of Human Services, Office of Developmental Disabilities, Central Region. She is the former Vice President of Integrative Counseling Services, PC in Harrisburg, PA. In 2019, Robin won the NADD Earl L. Loschen Award for contributions that have resulted in significant improvement in the quality of life for individuals with intellectual and developmental disabilities as well as mental health needs. Robin has developed the Risk Screening for Best Practices Tool. She is a subject matter expert on Fetal Alcohol Spectrum Disorder “The Invisible Disability” and has articles published on the topic. Robin administers sexuality assessments for consent, knowledge, and attitudes. She also administers trauma informed assessment for people with problematic and sex offending behavior. She is currently the Executive Clinical Director for Merakey Pennsylvania, NJ, DE & VA and assists with consultation services that include New York, and California.
Contact Information
Robin VanEerden, MS, LPC, NADD-DDS, CC
Executive Clinical Director, National Presenter, Co-Chair of NADD Clinical Certification Committee
Merakey Intellectual Disabilities Services Division
Dubovsky | 43-48
Volume 12 ► Issue 2 ► August 2023
Optimizing Outcomes by Recognizing and Responding to Fetal Alcohol Spectrum Disorders
Dan Dubovsky, MSW
Fetal Alcohol Spectrum Disorders (FASD) are caused by the effects of alcohol on a developing embryo and fetus. As alcohol is a legal drug and is frequently consumed, the effects of alcohol on an unborn child are not universally recognized, about half of all pregnancies are unplanned, and people are most often not aware of when they first become pregnant, FASD are more common than many other disorders and are much more common than most people think. Although there is a great amount of stigma regarding FASD, people who are pregnant do not intend to harm their unborn children. The current generally accepted prevalence is 1 in 20 or 5%. However, recent studies in the U.S. (May P, Chambers C, Kalberg MA, et al. (2018). “Prevalence of Fetal Alcohol Spectrum Disorders in 4 US Communities.” Journal of the American Medical Association: 319(3) 474-482) have found the weighted prevalence to be as high as 1 in 10. This is especially significant in our specialized services as the prevalence is often even higher in settings such as developmental disabilities, intellectual disabilities, special education, mental health, vocational rehabilitation, and corrections.
The diagnostic capacity for FASD is miniscule compared to the prevalence. FASD is therefore often not recognized. As a result, behaviors such as not following through with multiple instructions or directions, overreacting to minor stressors, acting aggressively, and having repeated tantrums or rages are seen as willful and purposeful behaviors. However, due to the effects of prenatal alcohol on the developing brain, behaviors that individuals with an FASD often demonstrate are due to how their brain is functioning. These individuals frequently receive other diagnoses, which may be misdiagnoses or true co-occurring issues. However, no matter which it is, the treatment will not be effective if the FASD is not correctly recognized and integrated into approaches. Therefore, it is essential to be able to recognize FASD, and the earlier it is identified, and appropriate approaches are implemented, the better the long-term outcomes for the individual, family, providers, and systems of care. Understanding brain structures that are affected by prenatal alcohol and the functions of those structures helps us understand the behaviors of those with an FASD differently and change our approaches with this in mind. For example, as the part of the brain responsible for immediate or working memory is often impaired, instead of giving someone multiple instructions, directions, or rules, it is more effective to provide one step at a time.
As a result of this imperative to identify FASD, it is vital to utilize a screening/assessment approach to identify those individuals with a probable FASD and implement modifications to approaches as early as possible. With this in mind, two colleagues of mine at the University of Washington and I developed the Life History Screen (LHS) to identify older adolescents and adults with a probable FASD. The LHS has 32 questions in 9 categories. It was developed based on statistically significant differences in responses to these questions in categories such as childhood history, prenatal alcohol exposure, day to day behaviors between those with and without an FASD (Grant TM, Novick Brown N, Graham JC, Whitney N, Dubovsky D, Nelson LA. “Screening in treatment programs for Fetal Alcohol Spectrum Disorders that could affect therapeutic progress.” International Journal of Alcohol and Drug Research 2013: 2(3) 37-49). The draft screen was tested by 22 residential substance use treatment programs in several states, the results of which identified the key categories as those mentioned above. Additional categories included education, living situation, employment and income, and substance use. The screen is administered by an FASD trained individual after training on the screen, how it is introduced, and how to ask questions in a way to promote honesty and minimize stigma. Although this screen is not diagnostic, a German study (Shwerg and Ahlert (2018) presentation at the 8th International Research Conference on Adolescents and Adults with FASD, Vancouver BC) found that it was 92.8% accurate in identifying those with or without an FASD.
Once a person receives a positive Life History Screen, modifications need to be implemented based on the scientific understanding of brain processing issues in FASD due to the effects of alcohol on the developing brain. Behaviors that appear to be willful and purposeful may well be due to damage to certain brain structures. If that is the case, typical reward and consequence approaches will not improve those behaviors. The LHS and modifications approach has been utilized in adult treatment settings with positive shifts in understanding on the part of staff regarding behaviors and how best to address them. Modifications are based on an understanding of brain processing in individuals with an FASD and include approaches that modify the environment to help the individual reach their optimal potential rather than expecting the individual to change his or her behavior. In addition to providing one direction at a time as mentioned above, utilizing repeated role playing, being consistent in routines, utilizing multiple senses such as visuals and tactiles rather than relying on verbal approaches, providing a mentor as a positive role model, and simplifying the environment.
In 2017, the State of Michigan wanted to implement a screening and assessment approach to identify youth who come through the public mental health system who may well have an FASD. To this end, a quick 5-6 question screen that could be implemented by a trained intake worker for families of children Birth-5 and 6-21 was developed, along with a modification of the Life History Screen. A positive brief screen would lead to an assessment utilizing the modified LHS completed between a trained clinician and the family and older youth. A positive assessment would lead to two main interventions, either Families Moving Forward, an evidence-based practice developed by Heather Carmichael Olsen at the University of Washington, or Strengths and Strategies, an evidence-informed practice developed by Dan Dubovsky in collaboration with Kathy Fitzpatrick, the FASD Initiative lead at the State of Michigan Department of Health and Human Services. Families Moving Forward is a manualized approach working with parents of children with an FASD 3-13 years old to build an understanding of the basis of the child’s behavior and respond differently to improve outcomes. Strengths and Strategies begins by identifying strengths in the individual, family, providers, and community and utilizing those in combination with strategies based on the understanding of brain functioning to modify the environment and improve functioning for those with an FASD.
In Pennsylvania, we have been able to collaborate with Luzerne. Wyoming, and Crawford Counties to implement the screening, assessment, and strengths and strategies approach in Children’s Service Center in Luzerne and Wyoming and the Juvenile Probation Office in Crawford County. Staff are trained in FASD and in the use of the screen and assessment, a strengths assessment, and strategies to address challenging behaviors. Regular coaching calls with staff were also provided to address specific issues and situations.
This approach of identifying and utilizing strengths in the individual along with strategies based on brain processing to address challenging behaviors and educating families and other providers to understand the basis of behaviors in FASD, has resulted in positive outcomes for many, including lowering a risk of family disruptions and improving behaviors in the individual. The key is helping those living or working with a person with an FASD to understand that we need to modify the environment in order to help the individual reach their best potential rather than expect the individual to change their behavior if they are motivated.
Biography
Dan Dubovsky, MSW, has worked for over 50 years in the field of behavioral health as a direct care worker in residential treatment and a therapist in residential, hospital, and outpatient settings. For over eight years, he was an Instructor in Psychiatry in the Division of Behavioral Healthcare Education, writing and teaching courses on child and adolescent development, loss and grieving, schizophrenia, mood disorders in children and adolescents, youth and violence, transition, fetal alcohol spectrum disorders, and psychopharmacology among others. He has been involved in fetal alcohol spectrum disorders (FASD) for over 35 years. For 14 years he was the FASD Specialist for the Substance Abuse and Mental Health Services Administration (SAMHSA) FASD Center for Excellence until its funding was eliminated. For the past several years, he has focused on the development and implementation of a screening, assessment and modification protocol for children, adolescents, and adults to help individuals and families reach their best potential. For his work in FASD, his son Bill has been his mentor and best teacher. He is currently an independent contractor providing training and technical assistance throughout the U.S. and Canada.
Contact Information
Dan Dubovsky, MSW
FASD Specialist ddubovksy@verizon.net
215-694-845
Hodas | 49-58
Volume 12 ► Issue 2 ► August 2023
Fetal Alcohol Spectrum Disorder (FASD): Thirty
Reasons Why Early Identification Matters
Gordon R. Hodas MD
As discussed in this paper, identification, and especially early identification of an FASD in a child can be quite empowering, especially to the child’s parents or other caregivers (family), because identification clarifies the primary source of the child’s challenges and provides an invaluable cognitive anchor. However, valuable as early identification is, the child and family also need an FASD-informed workforce, providing expertise in helping the family effectively address specific areas of concern while also promoting the child’s positive developmental progression over time. This is why the Luzerne and Wyoming counties FASD pilot project described in the current issue of the ODP Positive Approaches Journal is so meaningful. Identification is an important first step, but we also collectively need to work to develop a comprehensive FASD system of care.
This article was reprinted from permission of the Office of Mental Health and Substance Abuse. Children’s Mental Health Matters (pa.gov)
Introduction
Previous articles in the Children’s Mental Health Matters series (Hodas, 2012, 2015, 2016) have addressed the nature and challenges of Fetal Alcohol Spectrum Disorders (FASD). Given that the primary deficits in FASD – namely, those related to the direct effects of in-utero alcohol exposure on the developing brain – are irreversible, some might be tempted to dismiss early identification as a waste of time. In fact, such thinking is erroneous. In what follows, we consider thirty reasons why early FASD identification truly matters.
What is “early identification”?
While there is frequent mention of early identification in the literature, often this term is not explicitly defined. With progress in research and technology, the operational definition of early intervention can be expected to change, making it easier to identify FASD early in a child’s life and perhaps even in-utero.
For purposes of discussion here, early intervention refers to early childhood, with a range from birth to 6 years, and with identification ideally occurring by age 2 years. It should be appreciated that, for all children, brain plasticity and therefore the potential capacity for growth are greatest early on. This is the case even for children with in-utero brain damage, such as children with an FASD.
Thirty reasons why early identification of FASD matters.
Early identification of FASD matters, and can benefit family, child, and schools/service providers. When the child’s strengths and FASD-related limitations are understood, the following can occur:
Family
- The specific FASD diagnosis serves as a cognitive anchor for parents, enabling them to better understand their child, offering them a sense of relief, and increasing their sense of mastery.
- Parents can more easily understand the child’s realistic capabilities and limitations and thereby have appropriate expectations of the child – e.g., they can be developmentally competent with their child.
- It becomes less likely that parents will blame the child for challenging behaviors, limited academic performance, and apparent failure to cooperate – all of which may be due to neurologically-based limitations.
- It is less likely that the child will be subject to maltreatment on the part of a frustrated family.
- It is less likely that others will blame the child’s parents for the child’s behavior and other limitations. In addition, siblings will less likely be targeted, and will be better prepared to respond appropriately to unkind comments.
- The child’s family can be helped to understand that the child will likely require greater supervision and oversight to ensure safety than an unaffected child of the same chronological age.
- The child’s family can learn about and seek evidence-based and promising practices for children with FASD.
- Parents can seek the support of other parents dealing with similar challenges.
- The family, by learning how to navigate complex systems and community resources and by maintaining realistic goals, is better able to be hopeful and strengths-based throughout the child’s development.
- The biological mother of a child with an FASD, once informed about the deleterious effects of prenatal alcohol exposure and given nonjudgmental support, is less likely to use alcohol during future pregnancies.
Child
- The child can be helped to understand the likely reasons for various behavioral, cognitive, and interpersonal struggles.
- The child’s strengths and interests can be identified and cultivated.
- In a developmentally appropriate way, the child can be assisted in addressing areas of weakness at the same time that areas of strength are supported.
- Others can learn how to best communicate with the child. This includes parents, teachers, and involved human service professionals, and siblings, extended family, neighbors, and other community resource persons.
- Commonly co-occurring disorders can be identified and treated, without the underlying FASD being overlooked.
- The child’s capacity to maintain personal safety and respond to unsafe situations can be assessed, and appropriate interventions implemented.
- The child is less likely to engage in self-blame and more likely to continue to put forth efforts to improve.
- Shaming of the child becomes less likely.
- Small successes that might otherwise be ignored or taken for granted can be highlighted, enabling the child to feel supported and competent.
School and Service Providers
- It becomes easier to work in partnership with the family to develop and implement a plan of care.
- It is more likely that Early Intervention services will be sought and provided.
- There is a compelling reason to convene a child and family team and embrace a system of care approach to intervention.
- Involved professionals can work to strengthen the family’s safety net, so that the community becomes safer and more responsive to child and family needs.
- A more informed decision can be made regarding what type of educational setting is most appropriate for the child at different times.
- Teachers can learn how to best teach the child, building on strengths and making necessary accommodations.
- Teachers and service providers are more likely to avoid interventions that are ineffective and punitive, and instead use interventions appropriate for a child with an FASD.
- Involved adults can ensure that teaching is multi-sensory in nature and makes use of modeling and role-playing, with less reliance on just verbal communication.
- More intentional efforts can be made to help the child deal with change and transitions.
- Involved mental health and other human service professionals can explore whether other children or adult family members might also be affected by an FASD.
- The family physician can monitor possible physical health problems associated with FASD, offer the family anticipatory guidance, and promote wellness.
Discussion
When a child presents with problematic behavior or is underperforming for unknown reasons, the family is stressed and well aware that something is wrong. Under these circumstances, a medical diagnosis is often experienced as “a gift.” It removes a paralyzing sense of uncertainty, instead providing much greater clarity regarding what is going on. A medical diagnosis can empower parents, whose concerns may have been dismissed by others or who may have been unjustly blamed for their child’s behavior. With a valid medical diagnosis at hand, child and family can now learn about the disorder and, with the help of others, explore what can be done.
For all of us, what we think influences how we act. If we believe that a child is being defiant and spiteful, it becomes challenging to show compassion. Anger and an urge to punish the child are more likely. However, children with an FASD are not acting spitefully, and most of their limitations are beyond their control. A very different response is needed – involving empathy, encouragement, and patience. Parents who unknowingly raised a child with an FASD in years past not uncommonly experience profound regret years later. Fully aware of the importance of early identification in retrospect, many such parents have thought, if not said, “If only I’d known at the time – what a difference it would have made.”
In working with children with an FASD, effective intervention for parents and others requires at least two fundamental skills.
- The first skill involves the ability to recognize that the child’s maladaptive functioning is not intentional – e.g., in the words of Diane Malbin, that it’s not that the child “won’t,” but rather that she “can’t” (2017).
- The second essential skill involves learning to be developmentally competent. This involves determining over time the child’s actual capabilities, so that realistic expectations can be developed and maintained.
These specific skills, together with relentless persistence, enable the family to offer the child encouragement and support, and can help the child experience success despite significant concurrent limitations.
Children with a chronic illness or medical disorder can lead meaningful, productive lives. Early identification promotes such positive outcomes. It opens doors, restores morale, and helps us discover next steps. For the wellbeing of individual children and their families as well as the larger community, we need to become more aware of FASD and better able to identify it – the earlier, the better.
References
1. Hodas, G (2012). Addressing the challenge of Fetal Alcohol Spectrum Disorder. Children’s Mental Health Matters, Number 3, September 2012.
2. Hodas, G (2015). How common are Fetal Alcohol Spectrum Disorders (FASD)? Children’s Mental Health Matters, Number 35, May 2015.
3. Hodas, G (2016). Fetal Alcohol Spectrum Disorders and systems of care: intervention at a higher level. Children’s Mental Health Matters, Number 52, October 2016.
4. Malbin, D (2017). FASCETS, 2017. PA/Articles/Blogs/FASD Identification/Why Identification Matters
Biography
Dr. Gordon R. Hodas, Board Certified in Adult and Child Psychiatry, has been Statewide Child Psychiatric Consultant to the Pennsylvania Office of Mental Health and Substance Abuse Services (OMHSAS) in Harrisburg since 1992. He has previously provided consultation and training in children’s mental health, including childhood trauma and the provision of trauma-informed care, for both Bucks County and Delaware County. Dr. Hodas served as a school-based child and adolescent psychiatrist at the former Wordsworth Academy, an approved private school for students with academic and emotional challenges, from 1992-2019. Dr. Hodas was formerly Clinical Professor of Psychiatry at the Pearlman School of Medicine at the University of Pennsylvania.
For many years, Dr. Hodas wrote many columns under the theme of “Children’s Mental Health Matters” for the now inactive PArecovery.org, a website operated by OMHSAS. These columns addressed children’s behavioral health from a public health perspective. Specific columns published on this address the following topics: trauma and trauma-informed care, youth suicidality, fetal alcohol spectrum disorders (FASD), strengths-based treatment, youth and family empowerment, wellness and resilience, and the need to promote healthy attachments between caregivers and children.
Dr. Hodas is a published songwriter, who uses music and poetry to engage and motivate children and families. In 1992, he published an audiotape of original songs to promote coping by children. Dr. Hodas, the father of three adult children, lives in Philadelphia with Barbara, his wife of 50 years.
Contact Information
Gordon M. Hodas, MD
gordonhodas@hotmail.com.