Positive Approaches Journal, Volume 12, Issue 4
| Site: | My ODP |
| Course: | My ODP |
| Book: | Positive Approaches Journal, Volume 12, Issue 4 |
| Printed by: | |
| Date: | Sunday, July 26, 2026, 8:39 AM |
Positive Approaches Journal | 6

Volume 12 ► Issue 4 ► February 2024
Mindful Aging: Let's Start the Conversation
Introduction
This issue of the Positive Approaches Journal focuses on the aging process in those with Intellectual Disabilities and Autism (IDA) and mental health. Pennsylvania has seen significant growth in their older adult population, and this trend certainly applies to those with IDA and mental health. Aging is an opportunity and a challenge for everyone, and several aspects of the process have unique manifestations in the IDA and mental health populations.
The articles presented in this issue of the Positive Approaches journal offer insight and expertise into several aspects of the issues that Pennsylvania’s aging population is confronting. Discussion on such key topics as dementia, social isolation, mental health and substance abuse, and the Pennsylvania Master Plan on Aging, are addressed.
It
is hoped that the expertise presented in this issue of the Positive Approaches
journal will allow the reader to gain significant knowledge of the status of
those who are aging and have IDA and mental health. This knowledge can enhance the approach to the
work they do to assist some of Pennsylvania’s most vulnerable citizens.
Lawrence D. Appel MD, SFHM, Medical Director
Office of Long-Term Living
Department of Human Services
Positive Approaches Journal | 7-12
Volume 12 ► Issue 4 ► February 2024
Data Discoveries
The goal of Data Discoveries is to present useful data using new methods and platforms that can be customized.
For the estimated 5.4 million autistic adults in the United States,1 middle and later adulthood can be particularly vulnerable periods, characterized by a growing evidence base indicating increased risk of early-onset dementia (including Alzheimer’s),2 Parkinson’s disease,2-5 depression,6 and epilepsy5 among autistic individuals compared to their non-autistic peers. This evidence has contributed to growing concerns about gaps in services and supports for autistic individuals and their families as they age into adulthood. Studies focused primarily on younger autistic adults suggest significantly elevated rates of co-occurring acute and chronic health and psychiatric conditions,7-9 and while these conditions likely persist throughout adulthood, there is a dearth of research on how they may present or change during this later period.6 The November 2023 Pennsylvania Autism Training Conference (PATC) featured a session on aging, dementia, and autism. This session highlighted tools for providers, to help identify changes in behavior that may indicate a need for additional follow-up, to ensure that the appropriate services and support systems are in place as autistic people age.
Some research also suggests that participation in community activities among autistic individuals declines from adolescence to adulthood,10 and there is further evidence that both autistic children and adults are less likely to be involved in community, social, recreation, and leisure activities compared to their non-autistic peers.11-13 However, there is also growing evidence that community participation preferences, including the relative and perceived importance of community activities, may differ between autistic and non-autistic individuals.14 Social isolation and loneliness in later adulthood have also been associated with increased risk for poor health outcomes, including neurodegenerative conditions like Alzheimer’s and Parkinson’s Diseases, in adults. This linkage, however, has not been explored in autistic adult populations. As we continue to learn more about the experiences of aging autistic individuals, we can develop better resources, and services and supports can be designed to align with these preferences more closely.
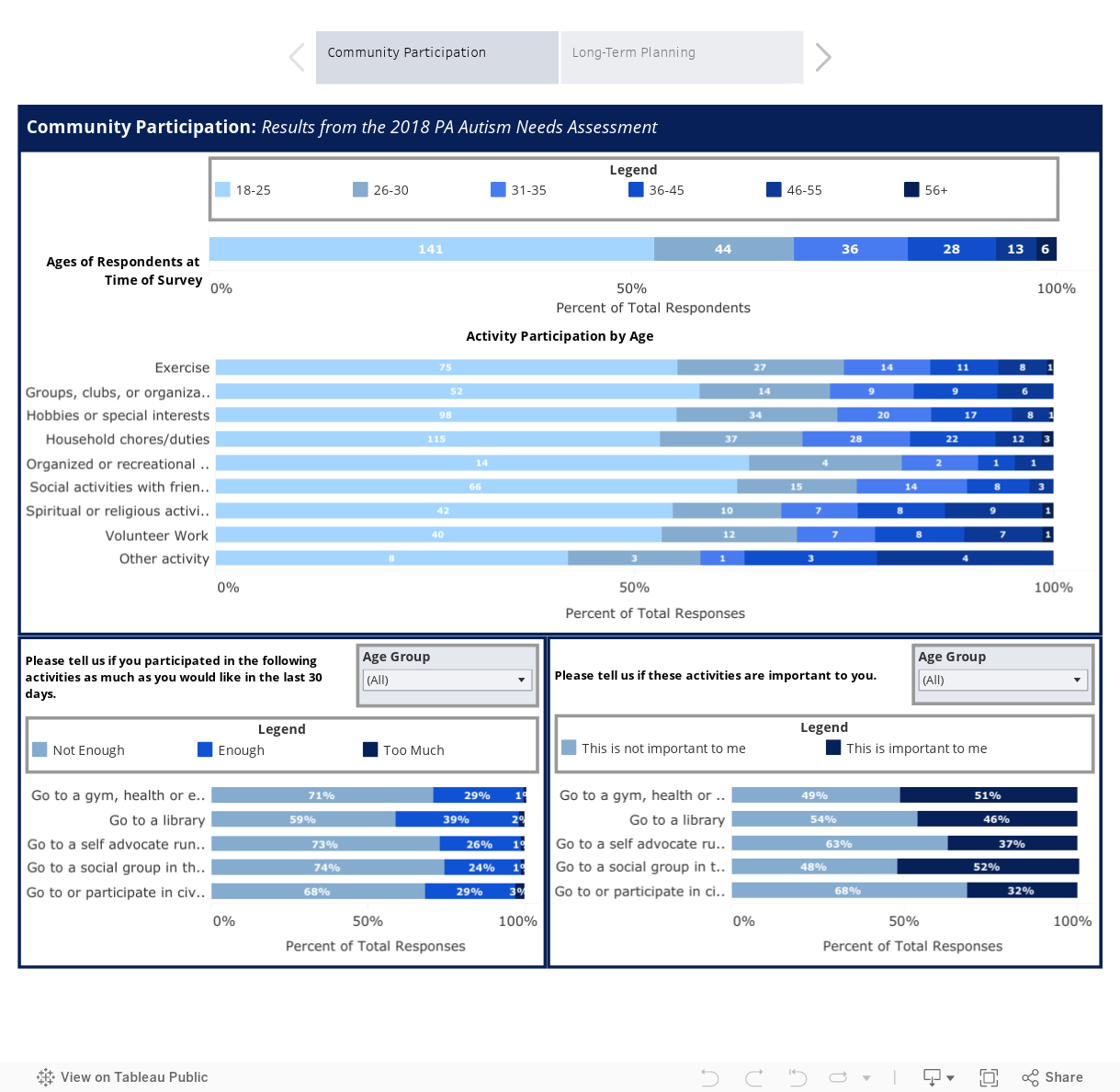
dashboard presented below visualizes data
from the 2018 Pennsylvania Autism
Needs Assessment (PANA) about community participation and preferences among autistic individuals
across different age groups (first tab) and caregiver long-term planning
activities and concerns (second tab). The data in the first tab show that
participation in activities, such as exercise and social activities, decreases
with age. Results also indicate that individuals have not participated in
community activities in the past thirty days as much as they would have liked.
Across all age groups, participants indicated that the activities listed were
relatively important with the importance of some activities increasing with
age. These findings underscore the importance of aligning services and supports
with the preferences of those receiving them. The second tab includes data from
caregivers of autistic individuals and captures long-term planning activities,
including concerns about making and maintaining these plans.
References
1. Dietz PM, Rose CE, McArthur D, Maenner M. National and State Estimates of Adults with Autism Spectrum Disorder. J Autism Dev Disord. Dec 2020;50(12):4258-4266. doi:10.1007/s10803-020-04494-4
2. Vivanti G, Tao S, Lyall K, Robins DL, Shea LL. The prevalence and incidence of early-onset dementia among adults with autism spectrum disorder. Autism Res. Oct 2021;14(10):2189-2199. doi:10.1002/aur.2590
3. Starkstein S, Gellar S, Parlier M, Payne L, Piven J. High rates of parkinsonism in adults with autism. Journal of Neurodevelopmental Disorders. 2015/08/30 2015;7(1):29. doi:10.1186/s11689-015-9125-6
4. Geurts HM, McQuaid GA, Begeer S, Wallace GL. Self-reported parkinsonism features in older autistic adults: A descriptive study. Autism. 2022;26(1):217-229. doi:10.1177/13623613211020183
5. Hand BN, Angell AM, Harris L, Carpenter LA. Prevalence of physical and mental health conditions in Medicare-enrolled, autistic older adults. Autism. 2020;24(3):755-764. doi:10.1177/1362361319890793
6. Lever AG, Geurts HM. Psychiatric Co-occurring Symptoms and Disorders in Young, Middle-Aged, and Older Adults with Autism Spectrum Disorder. J Autism Dev Disord. Jun 2016;46(6):1916-1930. doi:10.1007/s10803-016-2722-8
7. Croen LA, Zerbo O, Qian Y, et al. The health status of adults on the autism spectrum. Autism. Oct 2015;19(7):814-23. doi:10.1177/1362361315577517
8. Kohane IS, McMurry A, Weber G, et al. The co-morbidity burden of children and young adults with autism spectrum disorders. PLoS One. 2012;7(4):e33224. doi:10.1371/journal.pone.0033224
9. Buck TR, Viskochil J, Farley M, et al. Psychiatric comorbidity and medication use in adults with autism spectrum disorder. J Autism Dev Disord. Dec 2014;44(12):3063-71. doi:10.1007/s10803-014-2170-2
10. Myers E, Davis BE, Stobbe G, Bjornson K. Community and Social Participation Among Individuals with Autism Spectrum Disorder Transitioning to Adulthood. J Autism Dev Disord. Aug 2015;45(8):2373-81. doi:10.1007/s10803-015-2403-z
11. Egilson ST, Jakobsdóttir G, Ólafsson K, Leósdóttir T. Community participation and environment of children with and without autism spectrum disorder: parent perspectives. Scandinavian Journal of Occupational Therapy. 2017/05/04 2017;24(3):187-196. doi:10.1080/11038128.2016.1198419
12. Lamash L, Bedell G, Josman N. Participation patterns of adolescents with autism spectrum disorder compared to their peers: Parents’ perspectives. British Journal of Occupational Therapy. 2020;83(2):78-87.
13. Orsmond GI, Shattuck PT, Cooper BP, Sterzing PR, Anderson KA. Social participation among young adults with an autism spectrum disorder. J Autism Dev Disord. Nov 2013;43(11):2710-9. doi:10.1007/s10803-013-1833-8
14. Song W, Shea L, Nonnemacher SL, Brusilovskiy E, Townley G, Salzer MS. Community participation comparison between adults on the autism spectrum and adults in the general population. Journal of Autism and Developmental Disorders. 2021:1-12.
Eilber, Gray, Kyle | 13-20
Volume 12 ► Issue 4 ► February 2024
Pennsylvania Department of Aging Offers Services and Supports to Combat Social Isolation and Build Community Connection for Older Pennsylvanians
Jack Eilber, Karen Gray and Katrina Kyle
Strong social supports and connection to community resources can have a powerfully positive effect on health and well-being as we age. Combatting social isolation is a top priority for the Pennsylvania Department of Aging, due to the negative impact that it can have on the overall health and emotional well-being of the Commonwealth’s rapidly growing older population of 3.4 million people aged 60 and older. Social isolation is associated with a lower use of healthcare and an increased risk of depression, loneliness, lack of self-care, and mortality. While there are many definitions of social isolation, in essence, it is a lack of meaningful social connections. For older adults, the type and number of connections shift with changing social roles, increasing the risk of isolation. As we age, we are more likely to face life events that reduce connection with others: loss of spouse, partner, or other family and friends, loss of workplace interaction, decreased mobility and access to transportation, chronic illness, and loss of faculties such as hearing or vision.
Though a lack of social connections and life events can contribute to social isolation, geography can also be a factor. On average, rural Pennsylvania residents are older than their urban counterparts. In 2020, 20% of the rural population was 65 years old and older compared to 18% of the urban population.i The proportion of Pennsylvania’s older adult population in rural areas has been steadily increasing and outpacing the proportion living in urban communities. It is considered that older adults in rural locations would be the most socially isolated as they face many different challenges than those in urban areas. Some of these challenges are reduced access to healthcare, transportation, technology, and community supports.
The Pennsylvania Council on Aging (PCoA) – made up of 16 members with the majority of whom are required to be age 60 and older – conducted a statewide survey of older adults in response to the COVID-19 pandemic, which helped the Department of Aging highlight the devastating effects of social isolation on older adults. The survey was open to any Pennsylvanian over the age of 60 and was available in English and Spanish. The council received more than 3,700 responses from across the Commonwealth. The survey questions touched on situations such as, “how often the older adult was communicating with people outside of their home”, “whether they were happy with the amount of communication they had”, “what their current living situation was”, “how they were getting food” (going to grocery store, curbside pickup, meal delivery, etc.), and “what reasons they had for leaving their home” (grocery shopping, pharmacy, bank, etc.).
With input from PCoA and other aging network stakeholders, the Department of Aging offers a variety of programs and supports for older adults to help them live happy, healthy lives and with the dignity and respect that they deserve. Pennsylvanians can learn about these offerings by visiting the Department of Aging’s Website. The 52 local Area Agencies on Aging (AAAs) represent all 67 counties of the Commonwealth and are the local authorities for aging services in each county. The AAAs are staffed with skilled workers who can provide information about services and navigate how older adults can go about receiving those services.
The AAAs also support close to 500 Senior Community Centers across the Commonwealth. Senior Centers are great places for older adults to connect and engage with one another and their community. Each center provides nutritious meals, social engagement, enrichment and education programs, creative arts, health and wellness programs, and other special events unique to individual centers. These centers are often a real lifeline to social connections for older adults.
Volunteering time and talent and getting out into the neighborhood can be a great source of social connection for older adults. Aside from helping others and improving their community, volunteers also receive personal benefits. People who volunteer tend to live longer more vigorous lives, with greater functional ability and lower rates of depression than those who don't. By giving of their time, older adults may discover skill sets they did not know they had. The outcome can truly benefit everyone involved.
There are a variety of organizations that could use volunteers, including the Department of Aging. The department has multiple opportunities that include serving as a volunteer ombudsman to help ensure that residents of long-term care are getting the supports they need and deserve; helping with meals at local senior community centers, and training to counsel older adults trying to select the right Medicare coverage for themselves through Pennsylvania Medicare Education and Decision Insight (PA MEDI). Learn more about volunteer opportunities by calling your local Area Agency on Aging, or by visiting The Pennsylvania Department of Aging.
Social isolation can be the cause or contribute to the need for mental and behavioral health supports. The Department of Aging is committed to extending its reach of current community-based aging services by offering programming that addresses behavioral health among older adults. Pennsylvania became the first state to independently train and administer Healthy IDEAS (Identify Depressions and Empowering Activities for Seniors), an evidence-based depression self-management program.
Healthy IDEAS brings together the aging network and the behavioral health community to achieve significant benefits for older adults and their families who may be dealing with depression. The Healthy IDEAS program is integrated into the AAAs’ existing aging services. It is conducted by trained staff either in-person in an older adult’s home, or by telephone or video chat, over a three-to six-month period. The AAAs partner with local health and mental health care providers to facilitate referrals.
There are currently 20 Area Agencies on Aging that offer the Healthy IDEAS Program:
- Active Aging, Inc. (Crawford)
- Aging Services, Inc. (Indiana)
- Allegheny County Area Agency on Aging
- Challenges: Options in Aging (Lawrence)
- Clearfield County AAA, Inc.
- Columbia-Montour Aging Office, Inc.
- Cumberland County Office of Aging & Community Services
- Delaware County Offices of Services for the Aging
- Experience, Inc. (Forest/Warren)
- Jefferson County AAA
- Lackawanna County AAA
- Lehigh County Office of Aging and Adult Services
- Mercer County Area Agency on Aging
- Montgomery County Office of Senior Services
- Northampton County Area Agency on Aging
- Northumberland County Area Agency on Aging
- Philadelphia Corporation for Aging
- Pike County AAA
- Southwestern PA AAA, Inc. (Fayette/Greene/Washington)
- Venango County Older Adult Services
The PA Link to Aging and Disability Resource Centers, also known as the PA Link, assists older adults and individuals with disabilities by providing information and connecting them to supports, including assistive technology to access telehealth services, check-in calls, and options to help reduce social isolation. Any older adult needing support can contact the PA Link Call Center by phone at 1-800-753-8827 or online at PA Link to Community Care.
Many of the programs and services to protect older adults from social isolation and depression will play a role in building on long-term goals in the Department of Aging’s master plan, Aging Our Way, PA. The plan is a ten-year, state-led, and stakeholder-driven strategic plan designed to help transform the infrastructure and coordination of services for older Pennsylvanians. The plan will also reflect the needs and preferences of this population to live where they choose and access supports they need to thrive and age in place. One of the action steps in the plan to help combat social isolation is encouraging state and local agencies who serve older adults to use validated tools to measure loneliness and social isolation. These tools will help provide direction on interventions to connect those at risk with opportunities for social connection and engagement.
The Pennsylvania Department of Aging’s mission is to promote independence, purpose, and well-being in the lives of older adults through advocacy, service, and protection, while creating a commonwealth where older adults are embraced and empowered to live and age with dignity and respect. The Department oversees an array of services and support programs that are administered through its network of 52 local Area Agencies on Aging. Pennsylvanians can learn more about the Department of Aging by visiting The Pennsylvania Department of Aging.
References
1. Pennsylvania Department of Aging website: Pennsylvania Department of Aging.
2. Benefits & Rights Book for Older Pennsylvanians, developed by the PA Department of Aging.
Biographies
Jack Eilber has served as the Deputy Communications Director for the Pennsylvania Department of Aging since January 2020. He was recently tasked with overseeing DEI initiatives for the department. Jack is a member of the Aging Workgroup with the Governor’s Advisory Commission on LGBTQ Affairs and a member of the Western PA LGBTQ+ Advocacy Team. Prior to PDA, Jack was a Media Specialist for the Pennsylvania House of Representatives – Democratic Caucus, specializing in communication and outreach supports for Philadelphia representatives. He also did public relations work for Oyster Mill Playhouse in Camp Hill, PA, and the American Red Cross Central PA Chapter in Harrisburg.
Karen Gray joined the Pennsylvania Department of Aging in 2019 as Communications Director. During her 20+ years in marketing communications, she’s helped create campaigns and messaging to reach and assist older adults, people with disabilities, low-income families, and many other underserved populations across Pennsylvania. Her communications work for Commonwealth of Pennsylvania outreach efforts includes the Children’s Health Insurance Program (CHIP), the Statewide Adoption and Permanency Network, the Special Kids Network and the Shared Housing and Resource Exchange (SHARE) program. She holds a bachelor’s degree in Professional and Creative Writing from Carnegie-Mellon University.
Katrina Kyle is the Health & Wellness Statewide Coordinator for the Pennsylvania Department of Aging in the Education and Outreach Office. She manages PDA’s Health & Wellness Program and is primary contact for PDA’s endorsement of Healthy IDEAS, Healthy Steps for Older Adults, Healthy Steps in Motion and SMRC’s Chronic Disease Self-Management Education Suite. She has a bachelor’s degree in social work with a minor in psychology from Shippensburg University. She has over 30 years of experience promoting access to health and access to behavioral health for those in greatest of need. She has worked in the behavioral health field starting as a mental health case manager and later as the Director of the York/Adams Drug and Alcohol Program and Deputy Director for Dauphin County Drug and Alcohol Program.
Contact Information
Jack Eilber
Karen Gray
Katrina Kyle
Email: agingcomms@pa.gov
Putnam & van Heumen | 21-27
Volume 12 ► Issue 4 ► February 2024
Why We Need to Stop Othering People Aging with Disability
Michelle Putnam, PhD and Lieke van Heumen, PhD
One of the most frequent things we
do as scholars studying the phenomenon of aging with disability is explain who makes
up this population. The standard answer we provide is that persons aging with
disability are people who first experience impairment and subsequently
disability before age 60 or 65 – the historical chronological ages for when
people become eligible for traditional aging-related federal programs like the
Older Americans Act (age 60) (Administration for Community Living, 2023) and
Social Security retirement benefits (age 65) (Social Security Administration,
2023). Despite initiatives like Reframing Aging (Gerontological Society of
America, 2023), these numbers remain our cultural markers for when later life
supposedly starts. Persons aging with disability are a heterogenous population,
and includes anyone who experiences sensory, physical, mental and/or cognitive
long-term disability prior to later life. Examples are people who at birth, or
when they were children, were identified to have impairments like intellectual
and developmental disabilities (I/DD). The population also includes people who
incurred injuries like spinal cord injuries or chronic diseases like multiple
sclerosis, and people with sensory impairments, mobility impairments or
work-limitations.
Over the many years we have described and discussed this population, we still find ourselves starting from square one every time we begin a presentation, book chapter, article, or discussion – to clarify who we mean and to explain what is different about people in this group. We give examples – persons with I/DD might experience dementia earlier than those without I/DD. Individuals who experience blindness may have difficulty with wayfinding strategies they perfected as walkers if they begin to use mobility supports like a wheelchair in later life. Chronic pain may cause individuals with neuromuscular conditions to exit the workforce when pain levels are high or when workplace accommodations fall short. Autistic individuals may not be able to go about their usual routines when they become too physically demanding. We can come up with many more examples. Recently, we took a moment to reflect on this need to continually introduce this population to our audience. There seems to be little change in awareness of this population, despite the experience of aging with disability having been academically studied for several decades now (albeit by only a small number of researchers). This makes us wonder if we need a new way to discuss this group of people to increase their recognition in both domains of aging and disability. Here, we look at persons aging with I/DD as an example.
People with I/DD have historically been targeted by eugenics and other policies aimed at eliminating medical deviance, and they have been segregated through public policies and programs (Nielsen, 2012). Our hunch is that because of their long history of exclusion, people with I/DD are effectively “othered” into a category of individuals that has been extracted from the general aging population. Pulled out and to the side, if you will – and seen as a separate category of people. We see this clearly in the lack of inclusion of people with I/DD in gerontological research. There are aging-related studies with persons with I/DD as the study sample, but very few studies with general population samples are inclusive of persons with I/DD. It is also rare to see secondary data sets capture long-term disability, such as by including measures that ask if someone has been diagnosed with I/DD or how long a person has had an impairment or disability (i.e., duration or onset) (Coyle & Putnam, 2017). This means that many of the longitudinal aging studies that use these datasets create knowledge about aging experiences and the status of older adults without identifying persons with IDD or including long-term disability.
We also see an ongoing segmentation between U.S. federal and state programs for people who first experienced disability in early and mid-life and for those who may experience disability in later life. Although there are increasingly more initiatives that focus on families with individuals growing older with I/DD (Administration for Community Living, 2023), segmentation and exclusion of people with I/DD and their families from aging programs remains an ongoing issue. Individuals are rarely integrated and served by age, regardless of impairment or disability status. In practice, we see interest of service providers in aging-related organizations to increase training, knowledge, and inclusionary practices to support people with I/DD in later life, but there is limited investment in capacity building at federal and state levels to make that happen. This is a substantial problem as there is an absolute dearth of academic training on aging with disability in all fields, making on-the-job training critical to ensure that the needs of older people with I/DD and their families are met.
We ourselves have likely contributed to this segmentation as we employ the contrast of people aging with disability and people aging into disability, attempting to bring attention and awareness to this first group. It is perhaps easiest for our audiences to imagine that aging with I/DD is different than growing older without I/DD. For people with I/DD and other diverse cognitive, sensory, and physical traits, chronic conditions, and impairments, there are indeed differences in disability experience based on age of onset, duration of disability, and life stage. In identifying and learning more about those differences, we have often centered the disability experience – called it out as a distinguishing factor in the aging process. We have been articulating the need to recognize people with disabilities, including individuals with I/DD, as part of the aging population. We have been seeking inclusion by talking about advancements in longevity specifically. People with long-term disabilities are living longer than ever before. But stepping back, if we view aging as a lifelong process that starts long before age 60 or 65, then we recognize that people with I/DD, and others with long-term disability experiences, have always been a part of the aging population.
We collectively construct the definition and categories of the life course and its stages (Priestley, 2003). We have imagined a world where optimally, disability is not experienced until the very end of life and when it does, we imagine it to reduce the potential to engage – disability is about loss. This core tenet in Gerontology is exemplified by the goal of compressing morbidity – or concentrating disability towards the last years of life as much as possible (Minkler, 1990), and the focus on retaining independence rather than gaining or sustaining independence. Many “big ideas” in Gerontology are premised on these goals of avoiding and delaying disability and limiting its impact. This approach excludes people with disabilities by not recognizing them as an expected part of the general aging population, because by having disability in early and mid-life they have already failed to match our socially constructed expectations. This “othering” has led us to argue for inclusion for persons with disability into aging-related research, policies, programs, and educational training, but perhaps what we really need is to argue for ending their exclusion by recognizing the greater diversity of the aging experience and the older population in the first place.
This may seem like splitting hairs, a small pivot in approach, but we do not believe it is. We recognize that there is still a need to describe what is different about growing older with diverse cognitive, sensory, and physical traits, chronic conditions, and impairments, like I/DD. However, we realize that we need to frame this discussion, not as an ask for inclusion into Gerontology and aging-related policies and programs because of more people with disabilities living longer lives, but as a request to end the exclusion of people with disabilities. We can change how we frame, study, and support all people over the life course. Differences in humans are natural and normal. Disability is a variance in experience that can influence the aging process and outcomes across the life course – including later life.
Older people with I/DD have both similar and different needs and experiences compared to older people without I/DD. We need to be able to recognize differences while not “othering” older people with I/DD. We need to ground aging and growing older with I/DD as part of the larger collective set of experiences of aging. To conclude, we need to help people with I/DD age well and live meaningful lives, by ensuring that general aging services and policies can support them. If additional supports are needed, they should be provided because the older population is diverse, not because they are for the “other” aging population.
References
1. Administration for Community Living. (2023a, December 12). Older Americans Act. Administration for Community Living. Older Americans Act.
2. Administration for Community Living. (2023b). RAISE Family Caregiving Advisory Council. Administration for Community Living. Recognize, Assist, Include, Support, & Engage (RAISE) Family Caregivers Act Advisory Council.
3. Coyle, C. E., & Putnam, M. (2017). Identifying adults aging with disability using existing data: The case of the Health and Retirement Study. Disability and Health Journal, 10(4), 611–615. Disability and Health Journal.
4. Gerontological Society of America. (2023, December 12). Reframing Aging Initiative. Countering Ageism by Changing how we Talk about Aging. Reframing Aging. National Center to Reframe Aging.
5. Minkler, M. (1990). Aging and disability: Behind and beyond the stereotypes. Journal of Aging Studies, 4(3), 245-260.
6. Nielsen K. E. (2012). A disability history of the United States. Beacon Press.
7. Priestley, M. (2003). Disability: A life course approach. Cambridge: Polity.
8. Social Security Administration. (2023, December 12). Manage Benefits and Information. Social Security Administration. Social Security Administration.
Biographies
Michelle Putnam, PhD, MGS, is a Professor and Jennifer Eckert '08 School of Social Work Endowed Chair at Simmons University, School of Social Work in Boston, Massachusetts. Her scholarship focuses on the intersections of aging and disability, with a particular focus on aging with disability, long-term services and supports, and participation. She is a Fellow of the Gerontological Society of America and Member of the National Academy of Social Insurance.
Lieke van Heumen, PhD, FAAIDD (she/her) is a Clinical Associate Professor in the Department of Disability and Human Development at the University of Illinois Chicago. Her research interests include aging of people with intellectual and developmental disabilities, inclusive research methodology, and the scholarship of teaching and learning. She was a 2019-2020 American Political Science Association Congressional Fellow and Health and Aging Policy Fellow, placed with the U.S Senate Special Committee on Aging in the Office of Ranking Member Senator Bob Casey.
Contact Information
Michelle Putnam
Email: michelle.putnam@simmons.edu
Lieke van Heuman
Email: lvheumen@uic.edu
Lampenfeld, Pierce, Szymanski, Hancock | 28-39
Volume 12 ► Issue 4 ► February 2024
Aging Our Way, PA: Paths to Independence
Nathan Lampenfeld, Jessie Pierce, Gabrielle Szymanski and Kevin Hancock
On May 25, 2023, Governor Shapiro signed Executive Order (EO) 2023-09. This EO directed the Pennsylvania Department of Aging (PDA) and partners to evaluate issues facing older Pennsylvanians to support the development of a ten-year strategic plan. Recognizing that Pennsylvania has a larger than average older adult population, and that this population is growing faster than any other demographic, Governor Shapiro initiated this planning process to address the concerns of older adults across the commonwealth. To begin this planning process, stakeholders - including Pennsylvanians over the age of 60, caregivers, care partners, individuals engaged in supporting these populations - were asked to identify barriers that inhibit independence and opportunities to improve community living for older adults. Comments were organized by eight Domains of Community Living, created by the World Health Organization, and adapted for the United States by AARP. These domains are: Housing, Outdoor Spaces and Buildings, Transportation, Civic Engagement and Employment, Communication and Information, Respect and Social Inclusion, Social Participation, and Health Services and Community Supports. [i] According to many community members and service providers, Pennsylvania’s service system and infrastructure are not currently able to support these large and growing numbers of older adults. Extensive quantitative and qualitative data was shared with the Steering Committee and Subject Matter Experts, who provided recommendations within the eight Domains of Community Living. This plan, now known as Aging Our Way, PA, includes priorities, strategies, and tactics that promote the health, well-being, and quality of life of older Pennsylvanians and prepare the Commonwealth for a larger, longer-living older adult population. The plan is designed for adaptability, to respond to changing needs, shifting priorities, and available resources.
The development of Aging Our Way, PA is critical as demographic changes place a heavier burden on Pennsylvania’s service and infrastructure future. By 2030, the population of older adults, aged 60 and above, is projected to surpass 3.8 million (29% of the total population) and will outnumber every other demographic age group. [ii] Currently, nearly 14% of Pennsylvanians have a disability. [iii] With increased age, there's a heightened risk of acquiring physical disabilities and cognitive decline, both of which have impacted our activities of daily life. Estimates suggest that 50% or more of people with Down syndrome will develop dementia due to Alzheimer’s disease as they age. [iv] Additionally, the number of people with disabilities reaching older age groups and caregivers of people with disabilities becoming older adults are increasing. Older age, compounded with a physical or cognitive disability, presents new and different challenges. Anticipating and preparing for these intersecting trends is essential, as many people will have unique desires and needs as they age and will need specialized support for their journey.
Governor Josh Shapiro recognized that these distinct and overlapping trends are a call to action to build more inclusive, supportive communities for Pennsylvania’s older adults and adults with disabilities. A Master Plan for Older Adults (MPA) is a general term for a state-led planning process that convenes multiple departments and agencies designed to foster cross-sector collaboration and improve the infrastructure and coordination of services for older adult populations. [v] This term originated through the collaboration of a collective of organizations and funders that are working to mobilize financial, social, and intellectual capital, to restructure state and local policies and convene a wide range of cross-sector stakeholders to address the needs of Pennsylvanians as we age. The latter collective includes the Center for Health Care Strategies (CHCS), The SCAN Foundation, West Health, the May & Stanley Smith Charitable Trust, and the John A. Hartford Foundation, among others. MPAs allow states to plan for the rapidly growing population of older adults and people with disabilities, as well as the various compounding demographic shifts like increasing racial and ethnic diversity, increasing rates of solo-aging, and greater longevity among the oldest of the older adult cohort. MPAs consider the entirety of state, county, local and federal policies and programs, and private industry practices that directly or indirectly affect older adults and residents with a disability. A ten-year strategic plan is optimal for stable and mature organizations like state governments, to articulate a long-term vision and to ensure that the goals of the plan are in line with that vision. Several states are actively developing and implementing MPAs. The Pennsylvania Department of Aging (PDA) began this effort immediately after the executive order was signed, using the guidelines set by the Center for Health Care Strategies (CHCS) toolkit along with recommendations from the SCAN foundation and AARP.
PDA began and will continue this effort anchored by five core tenets:
- Transparency and inclusion involving significant stakeholder- and public-facing engagement as well as a strong communication plan.
- Embed diversity, equity, and inclusion in all phases of development, addressing disparities and promoting equity and inclusion regardless of a person’s age, gender and gender expression, sexual orientation, race, color, religion, national origin, disability, veteran status, socioeconomic status, geographic location, genetic information, and other differences not yet identified.
- Principles of person-centered planning, valuing older Pennsylvanians and Pennsylvanians with disabilities holistically, with careful consideration to each person’s unique needs and preferences.
- Creation of a living document that will evolve through the ten-year span of the plan based on the changing needs and preferences of older Pennsylvanians and Pennsylvanians with disabilities.
- A reframe of how we think about, talk about and value older adults and people with disabilities to recognize the momentum, experience, longevity, economic contributions, and wisdom of older adults and people with disabilities, and how these individuals add energy, vitality, and possibility to Pennsylvania.
Guided by these tenets, PDA began an extensive community engagement series to understand the barriers that older adults and people with disabilities face in accessing community life and enjoying the journey. PDA, in partnership with the statewide network of Area Agencies on Aging (AAAs) and the Pennsylvania Association of Area Agencies on Aging (P4A), sponsored over 200 virtual and in-person listening sessions, to gather more input from an individual or group either engaged with or affected by older adult and disability related services, programs, and infrastructure. Stakeholders were also invited to submit comments by mail, an online form, or e-mail. This complementary, multi-pronged approach to stakeholder engagement provided over 10,000 constructive points to engagement that allowed the PDA staff to understand the needs and perspectives provided.
PDA also collected data through a Community Needs Assessment, developed and distributed through academic and community partners, including the University of Pittsburgh and AARP Pennsylvania. This Needs Assessment was issued to document the baseline for older adult and disability services, infrastructure, and programming, and to identify clear gaps or barriers that need to be addressed by the plan. The Needs Assessment included a randomized, representative sample of older adults and older adults with disabilities, to present a more objective understanding of perspectives and barriers related to older adult quality of life. The Needs Assessment survey was also available to stakeholders to complete at their discretion. This survey was made publicly available in digital and printed forms in multiple languages and distributed to community partners and their networks, to broaden the understanding of perceived barriers to older adults in accessing services and infrastructure.
Both the Needs Assessment and listening sessions were structured through framework developed by the World Health Organization (WHO) and adapted by AARP for the United States to support the advancement of livable communities for older adults and adults with disabilities. [vi] This framework uses eight domains of livability to assess the characteristics of a geographic area, such as a municipality, city, or state, that make it more accessible to the 60+ population (with benefits for all residents.) The availability and quality of these domains are known to positively impact the well-being of older adults and help make communities more livable for people of all ages across the world. These eight domains include:
- Respect and social inclusion: Older adults and adults with disabilities from all backgrounds are valued and appreciated and no one is excluded based on race, geography, culture, language, gender, sexuality, ability, or socioeconomic status.
- Civic participation and employment: Older adults and adults with disabilities participate in employment, training, lifelong learning, volunteering opportunities, and inform government policies.
- Communication and information: Older adults and adults with disabilities access information they need in a variety of formats to stay informed and connected with their communities, families, and friends.
- Community support and health services: Older adults and adults with disabilities are assisted in staying healthy, active, and independent through community support and health services, including services responding to elder abuse, fraud, or exploitation.
- Outdoor spaces and buildings: Older adults and adults with disabilities live in an environment that includes open spaces, buildings, shaded areas, and walkways that are safe and easy to navigate.
- Transport: Older adults and adults with disabilities can get out and about using a range of affordable, user-friendly transport and associated services.
- Housing: Older adults' and adults with disabilities’ housing options are affordable, accessible, and close to transport and community services.
- Social participation: Older adults and adults with disabilities are supported to be active in their community, doing the things they enjoy.
Responses to the community engagement and the Needs Assessment survey clearly identified gaps and opportunities for improvement in each of these domain areas. Many of the comments presented by community members overlap in multiple domains, which emphasizes the purpose of this effort: to transform our infrastructure so that all Pennsylvanians are living in and experiencing the support of a holistically age- and disability-friendly community.
Stakeholders highlighted many barriers they face as areas of concern as they age:
- Health Systems and Supports: Concerns focus on long-term services and supports and behavioral health services for older adults and adults with disabilities, Alzheimer's and Dementia care costs, accessibility, workforce shortages, quality of care, and enhancing older adult substance abuse treatment.
- Communication Accessibility: Stakeholders emphasize the need for information to be from a source that they trust, and accessible in various formats, especially for those with vision impairments and those with hearing difficulties. They seek plain language and interpretable resources that may be understood by everyone.
- Navigation Challenges: Many community members expressed challenges in understanding where to get services and how to activate those services. Community members would like someone to assist them with navigating the system, coordinating services, and supporting them as they get connected to programs.
- Social Engagement: Loneliness is a major concern for older adults and adults with disabilities. Many respondents suggest that active involvement in community life helps prevent the negative health effects associated with social isolation. This involvement can significantly contribute both to the well-being and quality of life for the individual older adult, as well as benefit the community. Social participation can include a wide range of options including community events, individual activities, such as going to the movies, or events created specifically for older adults.
- Caregiver Support: Comments highlight challenges faced by professional and informal caregivers, emphasizing the need for recognition, fair pay, policy improvements, training, and resources. Financial struggles, lack of respect, and empathy in care settings are major concerns.
- Ageism and Ableism: Older adults and adults with disabilities express experiencing discrimination based on age, ability, race, sexual orientation, gender, and socioeconomic status. People feel disregarded, excluded from decisions, and subject to condescension. Discrimination extends across employment, customer service, and social interactions. A significant emphasis was placed by respondents on discrimination experienced in the healthcare system. Respondents believe that more education, intergenerational social activities, inclusive community spaces, and stronger neighborhoods could enhance community cohesion and respect.
- Crime and Abuse Concerns: Older adults of all abilities fear being targets of crime, leading to isolation. Issues of abuse, neglect, scams, and exploitation demand better protection for physical, emotional, and financial well-being.
- Home Modifications: Most older adults and adults with disabilities want to age in their homes and communities, but barriers exist in accessing necessary home modifications, healthcare, nutrition programs, and social opportunities.
These themes and more, were included in qualitative summary reports for each domain and shared with the Steering Committee led by the Pennsylvania Long-term Care Council (LTCC) per EO 2023-09. This committee was supported by Subject Matter Experts (SMEs) who were recruited from state government agencies and organizations that specialize in the domain areas mentioned above. They reviewed the data and spent October and November 2023 crafting recommendation reports for each of the eight domains. These reports outlined priorities, strategies, and actionable tactics, forming the basis of the Aging Our Way, PA plan. The recommendations are intended to build upon the existing infrastructure of public and private policies and programs.
These recommendation reports informed Aging Our Way, PA’s, 5 priorities of concern:
- Unlocking Access: Design and offer equitable, affordable, and available options and opportunities that older adults and adults with disabilities may choose from for healthy and engaged lives, regardless of ability; socioeconomic status; racial, ethnic, linguistic, or cultural backgrounds; or geographical location.
- Aging in Community: Remediate barriers that prevent older adults and adults with disabilities from remaining in their own homes, maintaining familiar surroundings, staying connected to their communities, and living in secure dwellings.
- Gateways to Independence: Promote older adults’ safe, convenient, and autonomous use of transportation and unhindered mobility.
- Caregiver Supports: Build a comprehensive catalogue of supports and enhancements that provide caregivers with help at home, respite, training, and navigations tools.
- Education & Navigation: Lead an extensive, coordinated network of community and academic partners to raise public awareness of services for older adults, provide information that reaches everyone and is understandable by all, ensure timely and streamlined connection to assistance with any need, and resolve the challenging problems that older adults and adults with disabilities face in their daily lives.
Each priority includes several strategic approaches to address barriers presented by community members and numerous actionable and measurable tactics actions to direct resources, including policy proposals, new programs or program changes, research proposals, proposed new and changed legislation, or funding requests, to support each strategy.
Aging Our Way, PA will provide a unified and realistic plan to guide every older adult, family, and stakeholder through a shared vision of how we, as individuals, determine to age our way with dignity, self-determination, and the supports and services we need to remain independent. In drafting this plan, Pennsylvania is committing to a future in which Pennsylvanians of all abilities have the resources we need to age with dignity and respect and continue to be vital, active members of our communities.
In this vision for the future, Pennsylvania will serve as a model for the nation, and prove that a community is only as strong as its commitment to inclusivity, respect, equity, and support for all its residents. By embracing the AARP's eight Domains of Community Livability, we commit to creating a state where every Pennsylvanian, especially older adults and adults with disabilities, can experience happiness, dignity, and fulfillment.
Aging Our Way, PA is a living document that is designed to be refreshed and advanced as priorities shift, and tactics are executed over the next ten years and beyond. The plan that we publish in 2024 will likely be different from the plan we have in 2034. PDA will continue to engage community members, coordinate efforts with other agencies, formalize collaborative partnerships, elevate common goals, and align the execution of strategies.
References
1. AARP Livable Communities (March 2023) The 8 Domains of Livability.
2. Rural Pennsylvania Population Projections by Gender and Age 2020 to 2050 Center for Rural Pennsylvania.
3. National Disability Rights Network. States Ranked by Percent of People with Disabilities Living in Hard-to-Count (HTC) Census Tracts. From Source: U.S. Census Bureau, American Community Survey 5-year Estimates 2017, and the CUNY Center for Urban Research, Hard-to-Count map data, 2019. States Ranked by Percent of People with Disabilities Living in Hard-to-Count (HTC) Census.
4. National Institute on Aging (November 2020). NIH Publication No. 20-AG-8021. Alzheimer’s Disease in People with Down Syndrome.
5. Center for Health Care Strategies. (2023). Getting Started with a Multisector Plan for Aging.
6. ARP Livable Communities. The 8 Domains of Livability: An Introduction (2023). The 8 Domains of Livability.Biographies
Nathan Lampenfeld is a William and Hannah Penn Fellow with the Commonwealth of PA. Through this program, Nathan is working within the Department of Aging, other state agencies, and countless stakeholders to develop and implement Aging Our Way, PA, Pennsylvania’s Multisector Plan for Aging.
Jessie Pierce is the Executive Assistant at the PA Department of Aging. Prior to PDA, she provided administrative services to the State Employees’ Retirement System, the Pennsylvania Liquor Control Board, and the Governor’s Office. In her current role, she is supporting the development and implementation of Aging our Way, PA, the ten-year strategic plan for aging in the Commonwealth.
Gabrielle Szymanski is currently the Executive Director of the Pennsylvania Council on Aging at the Department of Aging. In her previous role, she served as an Executive Assistant to the Secretary for the department and worked closely with the PDA team on the creation of Aging Our Way, PA. Gabrielle graduated from Georgia Southern University with a BA in International Studies and a BA in Spanish before going on to receive her MSc in Global Health Policy from the London School of Economics.
Kevin Hancock is a Special Advisor to the Secretary for the Pennsylvania Department of Aging. He has a long history of government service, including serving as Deputy Secretary for the Department of Human Services Office of Long-term Living, where he oversaw the implementation and operationalization of Pennsylvania’s Community Health Choices Program, the 15+ billion dollar, Medicaid-funded managed long-term services and supports program. He has also held executive and managerial level roles for the Commonwealth of Pennsylvania in health and human services, primarily supporting the Medicaid and long-term services and supports program. His work has primarily focused on organizational development, project and program management, program evaluation, quality assurance, information systems, and policy development. Kevin returned to state government service after three years as a professional consultant to manage the development of Aging Our Way, PA, the Commonwealth’s ten-year strategic plan to address gaps in services and infrastructure that support older adults. In addition to his work with the Department of Aging, Kevin is also completing a Sociology PhD focused on Administration and Leadership with Indiana University of Pennsylvania. He resides in the City of Harrisburg, PA.
Contact Information
Additional comments and feedback can be sent to agingplan@pa.gov.
Bishop & Pears | 40-51
Volume 12 ► Issue 4 ► February 2024
Aging, Health Care, Dementia, and IDD: The Intersection of Ageism and Ableism
Kathleen Bishop, Ph.D. and Kathryn Pears, MPPM
Abstract
Adults with intellectual and developmental disabilities (IDD) are more likely to experience health care inequities as they age. For older adults with IDD, it is the contention of the authors that not only ageism, but also ableism across the lifespan, impacts quality of health care and life. The authors provide examples with the desire that readers will come away as critical thinkers asking the question, ‘are there prejudices in the health care system that may be possible to change?’
Introduction
Adults with intellectual and developmental disabilities (IDD) are living longer, thanks to improvements in medical care for children and adults. (Janicki et al., 1999) Increased life expectancy increases the risk for the expression of age associated and age-related diseases, including Alzheimer’s disease and related dementias, as it does in the general population. (Perkins et al., 2010).
The increased risk for diseases and conditions for older adults with IDD increases the necessity for knowledgeable health care providers, screening, diagnosis, and interventions (Bishop et al, 2015; Moran et al, 2013). Recognition and appreciation of the increased life expectancy of adults with IDD is just now gaining recognition but has not kept pace with the needs of these aging adults. There are fewer health care providers who specialize in the care of adults with IDD and less research compared to the general population. (Institute of Medicine, 2007)
Research indicates health care providers are less likely to feel comfortable providing health care to people with disabilities. An example of such a study is cited by Gallegos (2021). In this study, 82% of survey respondents indicated their discomfort with providing health care to adults with disabilities, including adults with IDD, because of their concern over less information available. This same survey indicated many of the same respondents were reluctant to provide health care, partly due to a perception of a less likely positive outcome (Gallegos, 2021).
In this same article the author cites another study in which older adults with IDD were more likely to die from procedures or lack of accessibility to procedures, such as refusal to provide care during the height of the COVID epidemic (Gallegos, 2021). In yet another study, less than 50% of physicians felt adequate to provide health care to people with disabilities, including people with IDD (Iezzoni et al, 2021).
For aging adults with IDD, who are at risk of or who have developed a form of dementia, it is important that a proper differential diagnosis be conducted prior to labeling the individual as having dementia. “Dementia” is derived from the Latin word ‘demens’ meaning being out of one's mind, and is a general term used to describe a constellation of symptoms, such as personality change, cognitive impairment, and changes in memory. Although the word is frequently used as such, dementia is not an actual disease. Many conditions aside from Alzheimer’s (or one of the other related forms of irreversible dementia) can cause the symptoms we refer to generically as dementia. Therefore, determining the root cause of an individual’s symptoms through a thorough process of differential diagnosis, is imperative to identify the cause of cognitive decline and in providing appropriate interventions when possible (Alzheimer’s Association, 2024; Bishop et al, 2014; National Down Syndrome Society, 2019; Moran et al., 2013). It is the authors’ experience that the differential diagnosis process is rarely undertaken for people with IDD, and especially those with Down syndrome, when a medical assessment is undertaken for cognitive change.
Definition of Ageism and Abelism
According to the World Health Organization (WHO), ageism is defined as prejudice or discrimination based on a person’s chronological age. Ageism can affect older adults’ mental and physical health, as well as cause premature death (WHO, 2021). The discussion above, of less research focus on older adults with IDD and health care providers being less likely to provide care as compared to the general population, is at least partly indicative of widespread and pervasive ageism in health care (Gallegos, 2021).
Ableism is the mistaken belief that adults with disabilities are not as capable or valuable as people who do not have disabilities. This can result, as can ageism, in a lower quality of care and less potential for positive health outcomes from healthcare interventions (Smith, 2023). For example, a 2020 study found that approximately 83% of healthcare professionals studied viewed people with disabilities as already having a lower quality of life or being less healthy because of their pre-existing disability (Smith, 2023). Access to lab tests and other needed health care resources are often limited by lack of physical accessibility (Smith, 2023). These are all defined as implicit bias, that often those helping create the barriers, or the individual receiving services, are unaware of (Smith, 2023).
An estimated 7.39 million people in the United States had an intellectual/developmental disability in 2019, of whom three out of ten are adults. (Institute on Community Integration, 2019) The number of adults with intellectual and developmental disabilities aged >60 years is projected to nearly double from 641,860 in 2000 to 1.2 million by 2030 (Tinglen, 2013).
When you combine ageism with lifelong ableism, it doubles the negative impact of less access to knowledgeable health care for older adults with IDD (Altomara, 2022). Adults with IDD risk being treated differently because each is perceived as a person with a disability first and are defined by that perception (Altomara, 2022).
Ableism can be experienced in many
different forms. For the purposes of this paper, the form of ableism focused on
here is at the ‘Institutional level’, which includes medical ableism. Medical
ableism is defined as the attitude that intellectual/developmental disability
is perceived as a problem that needs fixing. This attitude can be taught in
medical schools and heightened in health policy that shapes the health care
system (Altomara, 2022). Some of this attitude can be seen in the lack of
relevant and appropriate assessment tools for screening for age-related
diseases such as Alzheimer’s disease and related dementias (ADRDs) in older
adults with IDD (Bishop et al, 2015; Esralew et al, 2009). This lack of
standardized assessment tools for aging adults with IDD increases the
likelihood that health care providers will not conduct a thorough differential
diagnosis, as is the standard practice used for the general population.
Persons with IDD, because of their underlying disability, have difficulty reporting symptoms and changes as well as understanding directions, thus making it difficult for health care providers to understand the changes taking place in the individual and to make informed decisions for proper evaluation and treatment. This can result in health care providers diagnosing cognitive impairment as an irreversible form of dementia and overlooking potentially treatable conditions.
The authors have selected three common types of IDD to illustrate how ageism and ableism come together to enforce stereotypes in older adults with IDD.
Down syndrome: Ageism and Ableism
Down syndrome (DS) is the most common genetic disorder and is caused by a partial (less than 100% of the body cells) or complete (affecting every cell of the body) triplication of chromosome 21 (Aldred et al, 2021). It is the most frequent cause of intellectual disability and is the most researched condition in relation to aging and dementia (Aldred et al, 2021; Bishop et al, 2015; National Task Group, 2012). Adults with DS experience what is termed, “accelerated aging,” and have higher mortality rates than the general population. (O’Leary, et.al., 2018)
People with DS also have an increased risk for developing Alzheimer’s disease and do so at an earlier age than in the general population or in the population of other adults with intellectual disabilities. About half of all people with DS will develop Alzheimer’s in their 60s (DeGraff et.al., 2017) compared to only five to six percent in the general population. (Mayo Clinic, 2022). Although beta-amyloid (Aβ) plaques and neurofibrillary tangles are typically observed by 40 years of age in adults with Down syndrome, the onset of symptoms does not typically occur until nearly a decade later. (Head et.al. 2017).
Many health care providers are
familiar with early research conducted in the 1970s that referenced this finding
but misunderstood that research to mean that the presence of beta-amyloid meant
that the individual had clinical Alzheimer’s disease. We now know that the
presence of the pathology seen in the brain at age 40, does not necessarily
mean that the individual will develop clinical Alzheimer’s disease, as there
appears to be a sub-set of people with Down syndrome who do not develop
Alzheimer’s at any age. (Head et al 2017) This leads to a tendency to ignore
the importance of a differential diagnosis to identify and treat potentially
treatable causes of cognitive decline in older adults with DS and an assumption
that Alzheimer’s disease is the only cause of cognitive decline in any adult
with DS over the age of 40.
Autism, Aging, and Dementia
Autism was originally described as “childhood schizophrenia” or the result of “cold parenting.” Its use as a diagnostic term was first introduced in 1943 by Dr. Leo Kanner, who first used the term to describe a social and emotional disorder. The Centers for Disease Control and Prevention (CDC) recognizes autism as autism spectrum disorder (ASD) and a developmental disability, caused by differences in the brain for which there can be many causes. The first group of individuals diagnosed with autism are now in their 70s and 80s. Typical characteristics of people with autism include challenges with social skills, repetitive behaviors, speech, sensory processing impairments, and language impairments (Autism Speaks, 2021).
Little data is available on numbers of older adults with autism. (Autism Speaks, 2021). Equally little is known about the prevalence and incidence of dementia in ASD. A 2021 study reported on a sample of adults with ASD aged 30–64 years who were enrolled in Medicaid and found that adults with autism spectrum disorder were approximately 2.6 times more likely to be diagnosed with early-onset Alzheimer’s disease and related dementias compared to the general population. (Vivanti et al. 2021). A few studies have hypothesized that the cortical plasticity associated with ASD might confer a protective mechanism (Happe et al., 2012). While research on childhood issues related to ASD grows, research on aging and autism lags.
Risk factors associated with the risk of dementia in the general population, such as older age, depression, the presence of additional psychiatric conditions, and cardiovascular disease appear to be similar for adults with ASD. (Vivanti et al 2021) Access to informed health care for adults with autism is limited. For young adults without informed health care and data on risk factors, there is an increased likelihood that erroneous assumptions as to the presence of Alzheimer’s disease or a related dementia will be made, as adults with ASD age and develop age-associated decline.
Cerebral Palsy, Aging, and Dementia
Cerebral palsy (CP) is a group of motor disorders due to abnormal brain development or damage to the brain before, during, or after birth affecting the ability to control muscles (Center Disease Control, 2024). There are multiple types of CP with co-occurring conditions including epilepsy, intellectual disability, and motor disorders.
There are very few studies exploring the incidence and prevalence of dementia in adults with CP. In fact, a Google Scholar search of cerebral palsy and dementia only returned four references, one of which was a small 2021 study conducted in the United Kingdom on 72 people, that found no difference in the number of people with CP and control subjects who were diagnosed with dementia during the follow-up. (Smith et al 2021). It has been speculated that chronic inflammation in the brain is a possible increased risk factor for dementia in conjunction with other co-occurring conditions, but more research is needed (CDC).
Due to the pre-existing risk factors related to CP, adults with CP should receive regular medical care to monitor brain health and address risk factors for dementia, as well as other age-related diseases. As for other adults with IDD, adults with CP have a difficult time finding knowledgeable health care with physically accessible offices and equipment.
Summary and Recommendations
The authors have not attempted to prove that ageism and ableism are the cause for all health care inequities for adults with IDD challenged by dementia. It would be impossible to prove in this short article. However, the authors have attempted to demonstrate areas in which older adults with IDD and either a diagnosed or suspected dementia are likely impacted by these systemic and societal prejudices. We hope the readers will be critical questioners about the possibility and, with awareness, begin to apply day to day changes in their attitudes and practices.
We have no conflicts of interests to disclose.
Disclaimer: The opinions expressed in this article are solely those of the authors. They do not necessarily reflect the views or opinions of the publication or any other individuals or organizations. The authors are responsible for the accuracy, completeness, and validity of the information presented in the article. Readers are encouraged to critically evaluate the content and form their own opinions based on reliable sources and additional research.
References
1. Alldred MJ, Martini AC, Patterson D, Hendrix J, Granholm AC. Aging with Down Syndrome-Where Are We Now and Where Are We Going? Journal of Clinical Medicine. 2021 Oct 13;10(20):4687.
2. Altomara, D. (2022, September 22). Including People with Developmental Disabilities. WebMed. Including People with Developmental Disabilities.
3. Alzheimer’s Association. Differential Diagnosis. Alzheimer's Association: Differential Diagnosis.
4. Autism Speaks (2021). What Is Autism? Autism Speaks: What is Autism?
5. Bishop, K.M., Hogan, M., Janicki, M.P., Keller, S.M., Lucchino, R., Mughal, D.T., Perkins, E.A., Singh, B.K., Service, K., Wolfson, S., and the Health Planning Work Group of the National Task Group on Intellectual Disabilities and Dementia Practices. (2014). Guidelines for Dementia-Related Health Advocacy for Adults with Intellectual Disability and Dementia: National Task Group on Intellectual Disabilities and Dementia Practices. Retrieved from The National Task Group on Intellectual Disabilities and Dementia Practices.
6. Centers for Disease Control and Prevention (CDC) (2023, October) What is Cerebral Palsy? Centers for Disease Control and Prevention: What is Cerebral Palsy?
7. De Graaf G, Buckley F, Skotko BG. Estimation of the number of people with Down syndrome in Europe. Eur J Hum Genet. 2021 Mar;29(3):402-410. doi: 10.1038/s41431-020-00748-y. Epub 2020 Oct 31. Erratum in: Eur J Hum Genet. 2022 Oct;30(10):1199-1200. PMID: 33130823; PMCID: PMC7940428.
8. Esralew, L., Janicki, M., & Keller, S. (2009) National Task Group Early Detection Screen for Dementia (NTG-EDSD). In V. P. Rasher (Ed.), Neuropsychological Assessments of Dementia in Down Syndrome abd Intellectual Disabilities (pp 197 – 213). Berlin/Heidelberg, Germany: Springer.
9. Gallegos, A. J. (2021). Misperceptions of people with disabilities lead to low-quality care: how policy makers can counter the harm and injustice. Health Affairs Forefront. Misconceptions of People with Disabilities and How Policy Makers can Counter the Harm and Injustice.
10. Institute of Medicine (US) Committee on Disability in America. The Future of Disability in America. Field MJ, Jette AM, editors. Washington (DC): National Academies Press (US); 2007. PMID: 20669428. The Future of Disability in America.
11. Happé, F., & Charlton, R. A. (2012). Aging in autism spectrum disorders: a mini-review. Gerontology, 58(1), 70–78. Aging in Autism Spectrum Disorders: A Mini-Review.
12. Head, E., Phelan, M. J., Doran, E., Kim, R. C., Poon, W. W., Schmitt, F. A., & Lott, I. T. (2017). Cerebrovascular pathology in Down syndrome and Alzheimer disease. Acta neuropathologica communications, 5(1), 93. Cerebrovascular Pathology in Down Syndrome and Alzheimer Disease.
13. Iezzoni, L. I., Rao, S. R., Ressalam, J., Bolcic-Jankovic, D., Agaronnik, N. D., Donelan, K., ... & Campbell, E. G. (2021). Physicians’ Perceptions Of People With Disability And Their Health Care: Study reports the results of a survey of physicians' perceptions of people with disability. Health Affairs, 40(2), 297-306.Retrieved January 1, 2024.
14. Institute on Community Integration. (n.d.). Residential Information Systems Project 2019. People with IDD in the United States. Minneapolis: University of Minnesota, RISP, Research and Training Center on Community Living, Institute on Community Integration. People with IDD in the United States.
15. Janicki, M., Dalton, A. J., Michael Henderson, C., & Davidson, P. W. (1999). Mortality and morbidity among older adults with intellectual disability: health services considerations. Disability and rehabilitation, 21(5-6), 284-294.
16. Mayo Clinic (2022). Young-onset Alzheimer's: When symptoms begin before age 65. Young-onset Alzheimer's: When symptoms begin before age 65.
17. Moran, J. A., Rafii, M. S., Keller, S. M., Singh, B. K., & Janicki, M. P. (2013, August). The National Task Group on Intellectual Disabilities and Dementia Practices consensus recommendations for the evaluation and management of dementia in adults with intellectual disabilities. In Mayo Clinic Proceedings (Vol. 88, No. 8, pp. 831-840). Elsevier.
18. National Down Syndrome Society. (2019). Alzheimer’s Disease & Down Syndrome A Practical Guidebook for Caregivers. Washington, DC: NDSS. Alzheimer’s Disease & Down Syndrome: A Practical Guide for Caregivers.
19. National Task Group on Intellectual Disabilities and Dementia Practice. (2012). ‘My Thinker’s Not Working’: A National Strategy for Enabling Adults with Intellectual Disabilities Affected by Dementia to Remain in Their Community and Receive Quality Supports.
20. Perkins EA, Moran JA. Aging adults with intellectual disabilities. JAMA. 2010;304(1):91–2.
21. Institute on Community Integration. (n.d.). Residential Information Systems Project 2019. People with IDD in the United States. Minneapolis: University of Minnesota, RISP, Research and Training Center on Community Living, Institute on Community Integration. People with IDD in the United States.
22. Smith, Anna (August 23, 2023). Medical News Today. Biases in Health Care: An Overview. Retrieved January 7, 2024, from Biases in Healthcare: An Overview.
23. Smith, K. J., Peterson, M. D., Victor, C., & Ryan, J. M. (2021). Risk of dementia in adults with cerebral palsy: a matched cohort study using general practice data. BMJ open, 11(1), e042652.
24. Tinglin, C. (2013). Adults with intellectual and developmental disabilities: a unique population. Today’s Geriatric Medicine, 6(3), 22.
25. Vivanti, G., Tao, S., Lyall, K., Robins, D. L., & Shea, L. L. (2021). The prevalence and incidence of early‐onset dementia among adults with autism spectrum disorder. Autism Research, 14(10), 2189-2199.
26. World Health Organization (18 March 2021). Ageing: Ageism. Retrieved January 1, 2024, at Word Health Organization-Ageing: Ageism.Biographies
Kathleen M. Bishop, Ph.D. has 40 years of experience in the IDD field and 30 as a Gerontologist with a specialty in aging with IDD. She has a BS from SUNY at Geneseo, MS in Special Education and a Ph.D. from Syracuse University in aging with disabilities. Dr. Bishop is a consultant for organizations in the aging and IDD networks and teaches online for Utica University, retired from the University of Rochester School and the NYS OPWD as well as VP of the National Task Group on ID and Dementia Practices. Dr. Bishop is Chair of the NTG Education and Training committee and VP for the NTG. Dr. Bishop presents the two-day NTG Dementia Capable Care for Adults with ID and the Third Day Train-the-Trainer with over 3000 attendees for the two-day and 800+ the Third Day. In her personal life, Dr. Bishop under the pen name of Mary Kathleen McKenna is author of the Women with Wisdom Series, two of which were published in 2023.
Kathryn Pears, MPPM Director of Operations, National Task Group on ID & Dementia Practices Principal, Dementia Care Strategies Kathryn is Director of Operations for the National Task Group on Intellectual Disabilities and Dementia Practices (NTG). Prior to accepting the staff position at the NTG she was Co-Vice President of the NTG’s Board of Directors and co-chair of the NTG’s Training and Education Committee. Kathryn is a nationally recognized expert on dementia who trains and consults with families, health care and long-term care professionals and facilities, and disability service providers. She specializes in the non-pharmacologic management of the challenging behaviors that occur with dementia. Personally and professionally involved in the field of dementia for over 30 years, her interest in dementia began in 1981 when her father was diagnosed with Early Onset Alzheimer’s disease at the age of 56. She was Director of Policy and Programs for the Alzheimer’s Association, Maine Chapter for 15 years. She also served as the registered lobbyist for the chapter and led the effort to make Maine one of the first states in the country to require special care unit disclosure for nursing homes, mandated training on dementia for nursing home staff, and a Silver Alert to mobilize law enforcement and the public when a person with dementia wanders and goes missing. In 2011 Kathryn started her own training and consulting company, Dementia Care Strategies. Kathryn lives in Aiken, South Carolina.
Contact Information
Kathleen M. Bishop
Email: kathiebishop@the-ntg.org
Kathryn Pears
Email: Email: bisbur1@earthlink.netShepard & Kertesz | 52-62
Volume 12 ► Issue 4 ► February 2024
Medicare and Coverage of Mental Health & Substance Use Disorders
Matthew Shepard and Kata Kertesz
Everyone has heard of Medicare, but very few people know the ins-and-outs of the program. This is especially true for those who are approaching Medicare eligibility and perhaps hadn’t considered how important the program will be to them. This article will provide some basics on Medicare, as well as discussing its coverage of mental health and substance use services.
What is Medicare?
Medicare is the national health insurance program to which all Social Security recipients who are either over 65 years of age or permanently disabled are eligible. In addition, individuals receiving railroad retirement benefits and individuals living with end stage renal disease are eligible to receive Medicare benefits.
Medicare for People with Disabilities
To qualify for Medicare by virtue of disability, before the age of 65, a person must have been eligible for Social Security Disability Insurance (SSDI) benefits for at least 24 months. The first 24 months is the waiting period for Medicare coverage. If the person returns to work, they can get up to 93 more months of premium-free hospital and medical insurance after the trial work period if they still have a disabling impairment. After the premium-free coverage ends, beneficiaries can purchase Medicare hospital and medical insurance if they continue to have a disability, but premiums can be prohibitively expensive.[i]
Medicare Versus Medicaid
“Medicare” is often confused with “Medicaid” – and some are eligible for both - but these are very different programs. Medicaid is an income-based program that is funded by the federal government but administered by individual states, and eligibility and coverage rules can vary greatly by state. A person’s income and assets are not a consideration for Medicare eligibility or benefit payment – though they can affect some cost-sharing. Medicare is a national program and rules should not vary significantly from state to state for those in the traditional program. Medicare coverage is similar to that provided by private insurance companies: it pays a portion of the cost of medical care. Generally, deductibles and co-insurance - which are partial payment of initial and subsequent costs - are required of the person receiving services.
The “Parts” of Medicare
Medicare has three substantive coverage components, Part A, Part B and Part D. Medicare Part A covers inpatient hospital care, hospice care, inpatient care in a skilled nursing facility, and home health care services. Part B covers medical care and services provided by doctors and other medical practitioners, durable medical equipment, and some outpatient care and home health services. Part D is prescription drug coverage, which was added to Medicare in 2006. Medicare drug coverage is only available through private plans – either a stand-alone Part D plan, or a private “Medicare Advantage” plan, discussed below.
Part A of the program is financed largely through federal payroll taxes paid into Social Security by employers and employees. Part B is financed by monthly premiums paid by Medicare beneficiaries and by general revenues from the federal government. In addition, Medicare beneficiaries themselves share the cost of the program through copayments and deductibles that are required for many of the services covered under both Parts A and B. Medicare Part C, the missing letter from the list above, is a bit different. An increasing number of beneficiaries (over 30 million nationwide)[ii] are receiving Medicare services through private, for-profit managed care plans. This is what Medicare Part C refers to – Medicare managed care.
As noted above, Medicare managed care is currently referred to as “Medicare Advantage” or “MA”. While it is different from the traditional Medicare program, by law MA plans must have coverage that is at least as good as that of traditional Medicare. In practice however, receiving that coverage is often more difficult, as MA plans often have limited provider networks, use strict requirements for coverage like Prior Authorization, and can terminate providers from their networks at will.
Medicare Coverage of Alcohol and Substance Use Disorders
Medicare covers certain screenings, services, and programs that aid in the treatment and recovery of mental health and substance use disorders (SUD):[iii]
- Alcohol misuse screenings – Free once per year from primary care provider for those who don’t meet the criteria for dependency.
- Counseling to prevent tobacco use & tobacco-caused disease - Medicare Part B covers up to eight smoking and tobacco-use cessation counseling sessions in a 12-month period.
- Opioid use disorder treatment services[iv] - Medicare covers treatment received from an opioid treatment program provider who's enrolled in Medicare and meets other requirements at no cost, EXCEPT in Medicare Advantage, as plans are allowed to charge a co-pay. The Part B deductible also still applies for supplies and medications you get through an opioid treatment program provider. Coverage includes:
- Approved medication-assisted treatment;
- Substance use counseling you get in person or virtually;
- Individual and group therapy you get in person or virtually;
- Toxicology testing; Intake activities;
- Periodic assessments you get in person or virtually;
- Opioid antagonist medications (like naloxone) approved for the emergency treatment of known or suspected opioid overdose;
- Overdose education you get along with opioid antagonist medication.
- Behavioral health integration services – For conditions including depression, anxiety and more, Medicare may pay your provider to help manage the condition. You pay a monthly fee and part B cost-sharing applies.
Medicare Coverage of Mental Health Care
- Inpatient – Part A covers services for those admitted as a hospital inpatient, but Part B covers services received from other providers while in the hospital. In 2024 there is a $1632.00 deductible. Days 1-60 are free and days 61-90 have a $408.00 co-pay per day. There are 60 “lifetime reserve days” after 90 days, at $816.00 per day. After those, nothing is covered for the stay. There’s no limit to the number of benefit periods you can have, whether you’re getting mental health care in a general or psychiatric hospital. However, if you're in a psychiatric hospital (instead of a general hospital), Part A only pays for up to 190 days of inpatient psychiatric hospital services during your lifetime.[v]
- Outpatient[vi] - Medicare pays for outpatient substance use disorder treatment as described above. In addition, it will cover:
- One free depression screening per year in a primary care doctor’s office or primary care clinic.
- Individual and group psychotherapy.
- Family counseling if the main purpose is to help with your treatment.
- Testing to verify services are needed and effective.
- Psychiatric evaluation.
- Medication management.
- Certain prescription drugs that aren’t generally drugs you would take on your own, like some injections.
- Diagnostic tests.
- Partial hospitalization.
- A one-time “Welcome to Medicare” preventive visit. This visit includes a review of your possible risk factors for depression.
- A yearly “Wellness” visit. Talk to your doctor or other health care provider about changes in your mental health since your last visit.
- Starting January 1, 2024 - Intensive outpatient program services.
- In traditional Medicare, costs for services other than depression screening will be 20% of whatever amount Medicare decided for the cost of that service (the “Medicare Approved Amount”) after the full Part B deductible has been met.
- Intensive outpatient services - Just started in January 2024, Medicare Part B covers intensive outpatient program services you get at a hospital, community mental health center, Federally Qualified Heath Center, or Rural Health Clinic. These services are “a level of mental health care between traditional once-weekly therapy or counseling, and inpatient psychiatric care.”[viii] Services may include group and individual therapy sessions. As with partial hospitalization, you pay a percentage of the Medicare-approved amount for each service, and once the Part B deductible is met, there is also coinsurance for each day of intensive outpatient program services you get.
- Telehealth[ix] –Telehealth services at any location in the U.S., including your home are available for services to treat a substance use disorder or a co-occurring mental health disorder (sometimes called a "dual disorder"), or for the diagnosis, evaluation, or treatment of a mental health disorder.
Conclusion
An estimated 1.7 million Medicare beneficiaries are living with a diagnosed substance use disorder (SUD) and one in four[x] Medicare beneficiaries are living with a mental health condition. While Medicare covers a broad array of treatment services for those with mental illness and substance abuse disorders, special rules limit coverage and reimbursement. Medicare’s coverage of services for mental health, behavioral health and substance abuse disorders is not as extensive as its coverage for other services. Medicare does not cover the full continuum of services recognized by the American Society of Addiction Medicine, nor the range of providers and settings needed for effective, evidence-based treatment. Medicare is not subject to the Mental Health Parity and Addiction Equity Act (Parity Act), which protects people with SUD and mental health conditions from insurance inequities. As a result, millions of Americans who depend on Medicare are unable to receive the life-saving treatment they need and deserve.
In 2022 the Center for Medicare Advocacy along with partners Legal Action Center and Medicare Rights Center released a set of principles to guide expansions in Medicare coverage.[xi] The principles would apply the Parity Act to Medicare Parts A, B, C and D, authorize coverage of the full continuum of evidence-based SUD treatment services, authorize coverage of community-based SUD treatment settings, authorize coverage of all licensed and certified mental health and SUD treatment providers, and establish adequate reimbursement rates.
Additional Resources for Information and Assistance
1. National Institute of Mental Health (NIMH), National Institutes of Health (NIH)
Visit: National Institute of Mental Health.
Call: 1-866-615-6464. TTY users can call 1-301-443-8431.
Email: nimhinfo@nih.gov.
2. Substance Abuse and Mental Health Services Administration (SAMHSA)
Visit: Substance Abuse and Mental Health Services Administration. To find treatment facilities in your area, visit Find Treatment.
Call: 1-877-SAMHSA-7 (1-877-726-4727). TTY users can call 1-800-487-4889.
3. Mental Health America
Visit: Mental Health America.
Call: 1-800-969-6642.
4. National Alliance on Mental Illness (NAMI)
Visit: National Alliance on Mental Illness.
Call or text the Information Helpline at 1-800-950-NAMI (1-800-950-6264).
5. National Council for Mental Wellbeing
Visit: thenationalcouncil.org.
Call: 1-202-684-7457.
Email: Communications@thenationalcouncil.org.
6. Legal Action Center
Visit: Legal Action Center.
Call: (212) 243-1313.
Email: lacinfo@lac.org.References
1. Social Security Administration. Medicare Information. Medicare Information.
2. Ochieng, N., Clerveau, G., Cubanski, J., & Neuman, T. (December 13, 2023). A snapshot of sources of coverage among medicare beneficiaries. KFF. A Snapshot of Sources of Coverage Among Medicare Beneficiaries.
3. Medicare.gov. Mental health and substance use disorder services. Mental Health & Substance Use Disorder Services.
4. Center for Medicare & Medicaid Services. Opioid treatment programs. (October 2022). Opioid Treatment Programs.
5. Medicare.gov. Mental health care (inpatient). Medicare and Mental Health Care for Inpatient Treatment.
6. Medicare.gov. Mental health care (outpatient). Medicare and Mental Health Care for Outpatient Treatment.
7. Medicare.gov. Mental health care (partial hospitalization). Medicare and Mental Health Care for Partial Hospitalization.
8. Medicare.gov. Mental health care (intensive outpatient program services). Medicare and Intensive Outpatient Program Services for Mental Health Care.
9. Medicare.gov. Telehealth. Medicare Part B (Medical Insurance) covers certain telehealth services. Medicare and Telehealth.
10. Parish, W. J., Mark, T.L., Weber, E.M., Steinberg, D. G. (August 2022). National Library of Medicine. Substance Use Disorders Among Medicare Beneficiaries: Prevalence, Mental and Physical Comorbidities, and Treatment Barriers.
11. McGinty, B. (July 9 2020). Medicare’s mental health coverage: How COVID-19 Highlights gaps and opportunities for improvement. (July 9, 2020). Medicare’s Mental Health Coverage: How COVID-19 Highlights Gaps and Opportunities for Improvement.
12. Parity principles to optimize medicare coverage of mental health and substance use disorder care. (July 2022). Legal Action Center. Optimizing Medicare Coverage of Mental Health and Substance Use Disorder Care.
Biography
Kata M. Kertesz, joined the Center for Medicare Advocacy in 2014 as a Policy Attorney. Her legal work focuses on the rights of those dually eligible for Medicare and Medicaid, the Affordable Care Act, the Medicare Savings Programs, and other matters regarding access to health care for lower-income people. Prior to joining the Center, Ms. Kertesz worked on Medicare issues at the National Council on Aging (NCOA), a non-profit agency that focuses on health care and consumer protection issues for older adults. While at NCOA, Ms. Kertesz engaged in administrative and legislative advocacy through coalitions of consumer protection groups. Ms. Kertesz earned her B.A. degree from Georgetown University and her J.D. degree from Georgetown University Law Center. She is admitted to the bars of the District of Columbia and Maryland, and the U.S. District Court for the District of Columbia.