Positive Approaches Journal, Volume 13, Issue 2
| Site: | My ODP |
| Course: | My ODP |
| Book: | Positive Approaches Journal, Volume 13, Issue 2 |
| Printed by: | |
| Date: | Sunday, July 26, 2026, 12:00 PM |
Positive Approaches Journal | 6-9

Volume 13 ► Issue 2 ► September 2024
Understanding Trauma: Expressive Therapies
Introduction
We have been engaged in a long journey, helping folks to see the relationship between a person’s intellectual and neurological differences, mental health issues, challenging behaviors, and their experiences of complex and on-going trauma. In the 1980’s and 90’s our focus was on changing the professional and clinical opinions that individuals with intellectual disability (ID) “could not experience or suffer from the consequences of trauma”. Much headway has been made in changing that perception. We now acknowledge the high incidence of trauma and the wide range of sources of trauma in people with ID. However, there is still much to learn and share about best and promising practices to support people in recovering from trauma, to move forward with a fulfilling, joyful life.
In the early 2000’s, The PA Dual Diagnosis Initiative introduced eye movement desensitization and reprocessing (EMDR) as a useful tool to help people heal from trauma through the teaching of Andrew Seubert. Through a grant from the Office of Developmental Programs (ODP), we provided intensive EMDR training for practitioners. While many clinicians were trained, we were faced with skepticism, and didn’t train to the scale we had hoped for. There weren’t any studies at that time directly supporting the use of EMDR with people with ID. As a result, we decided to conduct preliminary research using case studies of EMDR practice with people we worked with having Dual Diagnosis, showing the positive effects on individuals with ID without requiring them to be articulate or verbal. 1 For each person to qualify for the study, they had to have experienced at least one significant trauma in their life and be referred to us for help with their challenging behaviors. We were able to identify the traumas each participant in the study experienced using a biographical timeline exploring the person’s life. Therefore, we did not need to rely on a verbal report of the trauma experienced by the participants. Each person in the study showed significant gains. Their challenging behaviors subsided, replaced by more pro-social behaviors. Some folks also showed dramatically improved memory and capacity to organize their thoughts. For example, one person was able to ask questions about issues that had bothered them for years but had been unable to articulate their questions before engaging in EMDR.
We saw that we could impact a person’s mind/body trauma loop through the EMDR practice, with special focus on bilateral stimulation as a significant aspect of the process. (This article continues to be cited in many countries and is still being used as a launching off point to explore a variety of promising practices supporting people with ID to heal from trauma).
Using EMDR and seeing the impact of bilateral stimulation on individuals, regardless of their verbal abilities, heightened our interest in pursuing other means to offer body-based interventions from Lifestyle changes, including movement and nutrition, to Mindfulness and stress reduction practices, as well as a host of body-based therapies, including Neurofeedback, Neuro Entrainment, Biofeedback, Havening, Tapping, Music, Art, Equine and Animal assisted Therapy, and an ever-evolving group of therapies. 2
No matter which approaches we use, their success is predicated on the person having a safe, trustworthy, fulfilling homelife. We must always keep our focus on developing and sustaining a healing lifestyle. Together we are in this for the long haul, and as they say, “life happens”. People have triggers and setbacks, new losses and fear inducing situations, but can rebound well when they are supported by people they trust and know truly care for them.
In this issue of the Positive Approaches Journal, we see that there have been important strides in identifying the prevalence of trauma and the complex consequences of trauma from multiple sources, including social adversity, abuse and neglect. The focus is on the importance of taking this into consideration on every level, from systems collaboration, to how we assess, diagnose, treat, and offer restorative environmental supports to individuals with intellectual disability and autism (ID/A).
Beth Barol, PhD, LSW, BCB, NADD-CC
References
1. Barol, B. & Seubert, A. (2010). Stepping stones: EMDR treatment of Individuals with intellectual and developmental disabilities and challenging behavior. Journal of EMDR Practice and Research.4(4), 156-169.
2. Barol, B. & Focht-New, G.(2023) Biofeedback: Harmonizing the Brain and the Body for a Happier Life. In Price, U. & Baker, D.(Eds.), The Good Stuff (pp. 509-557). NADD Press.
Positive Approaches Journal | 10-13
Volume 13 ► Issue 2 ► September 2024
Data Discoveries
The goal of Data Discoveries is to present useful data using new methods and platforms that can be customized.
In our last issue, [1] we shared definitions of trauma, the circumstances under which it may manifest, and common physical and psychological trauma responses, including cardiovascular issues and anxiety disorders. There is some evidence that autistic people may be more likely to experience potentially traumatic events (PTE) and to develop post-traumatic stress disorder (PTSD) compared to non-autistic people.1,2 Some studies have examined the prevalence of PTSD among autistic individuals using measures of self-reported frequency of exposure to trauma and self-reported PTSD symptoms. For example, one study found that 45% of individuals on the autism spectrum reported symptoms of trauma, indicating probable PTSD, compared to only 4.5% of the sample without autism.3
These quantitative studies exploring the prevalence of PTSD among individuals on the autism spectrum have been based on relatively small, homogenous samples that are not nationally representative. One avenue of discovery to address this data gap is to use large, population-based samples to explore prevalence of autism and co-occurring conditions. National Medicaid claims present a unique opportunity to do this and to identify trends across years and variations within subgroups.
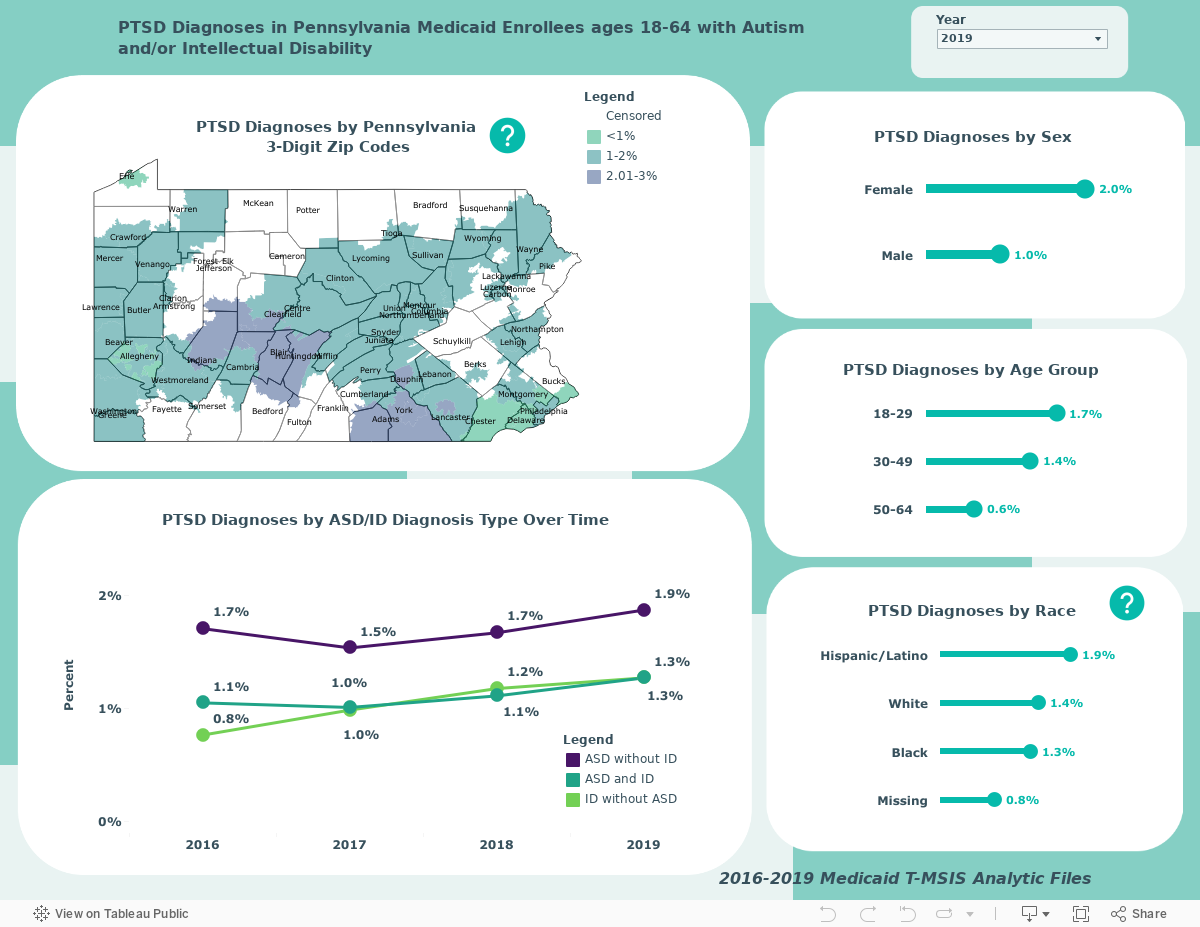
The dashboard below displays rates of PTSD among autistic Pennsylvania Medicaid enrollees between 18 and 64 years old with and without intellectual disabilities (ID) as well as enrollees with ID only. These rates differ from the small sample, self-reported studies because they do not measure PTSD in the same way. Using guidelines from the Chronic Conditions Data Warehouse, PTSD was defined here as having at least one inpatient or two other non-prescription claims associated with a PTSD diagnosis code. The benefit of this approach is that it allows for more reliable observations over time and between demographic groups. However, it is important to note that the data displayed here is derived from administrative claims data. [2] The overall sample sizes for each year are 49,675 (2016), 60,949 (2017), 62,719 (2018), and 61,191 (2019).
Data reflects Medicaid claims files from 2016-2019 and are derived from the Centers for Medicare and Medicaid Services (CMS) Transformed Medicaid Statistical Information System (T-MSIS) Analytic Files (TAF) personal summary and service claims files. Data may be filtered by year to explore changes in these rates over time and across Pennsylvania counties, sex, age group, and race.
Conclusions
While the data displayed here are exploratory, there are some noteworthy trends that indicate an urgent need for further research, clinician training, and increased awareness. Rates of PTSD ranged from 1-2% between 2016 and 2019 and there is a noticeable uptick in the rates among all groups and within subgroups. The highest rate of PTSD was observed in autistic people without ID (1.9% in 2019) and the lowest rate was observed in people with ID only (0.8% in 2016). Rates of PTSD were highest among women, those in the 18–29-year-old age group, and those who identified as Hispanic or Latino. Within Pennsylvania, among counties with data that is not censored, the highest rate of reporting PTSD was observed in Adams County in 2019 (3.6%).
It is also important to note the differences between the rates of PTSD observed here based on services claims and the rates found in other smaller studies that are based on self-reporting of PTSD symptoms. Results here may be an indication that autistic individuals are not receiving appropriate or sufficient support for PTSD. There are also important disparities within this sample that warrant further investigation: higher PTSD rates among women, those who are younger, and minoritized populations indicate a need to tailor services and treatment options to these groups. Researchers should prioritize analyses examining differences in rates of PTSD within these sub-populations of individuals with Intellectual and Developmental Disabilities (IDD). Findings can be translated into resources and training opportunities for providers and other clinicians, to improve understanding of trauma and how to best support individuals on the autism spectrum who are experiencing trauma and its effects.
The Autism Services Education Resources and Training Collaborative (ASERT) provides key trauma resources for providers, individuals, families, and communities (see the dashboard of key resources in the last issue of this journal). [3]
References
1. Ng-Cordell E, Wardell V, Stewardson C, Kerns CM. Anxiety and trauma-related disorders in children on the autism spectrum. Current psychiatry reports. 2022;24(3):171-180.
2. Peterson JL, Earl RK, Fox EA, et al. Trauma and autism spectrum disorder: Review, proposed treatment adaptations and future directions. Journal of child & adolescent trauma. 2019;12:529-547.
3. Rumball F, Brook L, Happé F, Karl A. Heightened risk of posttraumatic stress disorder in adults with autism spectrum disorder: The role of cumulative trauma and memory deficits. Research in Developmental Disabilities. 2021;110:103848.
Durgin | 14-22
Volume 13 ► Issue 2 ►September 2024
Creating a Trauma-Informed Human Services Workforce in Pennsylvania: A Successful Cross-Sector Collaboration.
Mark B. Durgin
PA Care Partnership, Pennsylvania
Abstract
This article provides an overview of grant-funded Trauma-Informed Care (TIC) training sponsored by the PA Care Partnership, in collaboration with Lakeside Global Institute (LGI), the Office of Mental Health and Substance Abuse Services (OMHSAS), and the Office of Children, Youth, and Families in Pennsylvania (OCYF). This work demonstrates the collaboration between the PA Care Partnership, OMHSAS, and OCYF, to successfully braid funding to contract and partner with Lakeside Global Institute to provide tuition-free comprehensive trauma training to over 20,000 human service professionals across the Commonwealth. By adopting Trauma-Informed Care in Pennsylvania, we are creating safe, supportive environments that promote healing and resilience for children and youth.
Introduction
This journal article will discuss the importance of Trauma-Informed Care in Pennsylvania, examine key initiatives and collaborations to promote trauma-informed practices, review trauma prevalence data specific to Pennsylvania, and provide practical steps for organizations to adopt TIC. It will conclude with a call to action for stakeholders and policymakers to prioritize the well-being of children and youth in Pennsylvania through trauma-informed approaches, using braided funding strategies, achieved through a collaborative System of Care.
Pennsylvania's approach to supporting children, youth, young adults, and their families who face behavioral health challenges is grounded in the System of Care (SOC) philosophy. The PA Care Partnership, in collaboration with the state's Department of Human Services (DHS) and OMHSAS, has embraced this framework, which values equality, trust, and cooperation among youth, caregivers, providers, and systems. The SOC approach builds upon each community's unique strengths and culture to create a spectrum of effective, community-based services and supports that are organized into coordinated networks, address cultural and linguistic needs, and build meaningful partnerships with families and youth.
Since 2009, OMHSAS has received four grants from the Substance Abuse and Mental Health Services Administration (SAMHSA), enabling the Commonwealth to establish an SOC framework. This philosophy does not seek to replace existing services, but rather fosters a way of working together among families, youth, government agencies, private providers, and communities. The flexibility and adaptability of SOC make it suitable for any context, with the ultimate goal of helping families function better at home, in the community, and throughout life.
Pennsylvania has increasingly recognized the importance of TIC in contemporary practice, particularly within human services, behavioral health, and child welfare, as well as in education. The adoption of TIC has been driven by a growing awareness of the prevalence of trauma and its long-term consequences, as well as a commitment to promoting resilience and well-being. Through the support of OMHSAS and the work of the PA Care Partnership, Pennsylvania has successfully implemented trauma training initiatives funded by SAMHSA’s System of Care grants and braided funding from OCYF.
What is Trauma-Informed Care?
Trauma-Informed Care is a framework that involves realizing the widespread impact of trauma, recognizing the signs and symptoms of trauma, and responding by integrating knowledge about trauma into policies, procedures, and practices. The core principles of TIC include safety, trustworthiness, peer support, collaboration, empowerment, humility, and responsiveness. TIC involves creating safe environments and being sensitive to cultural, racial, and historical contexts that shape individuals' experiences of trauma. Safety, both physical and emotional, is essential for individuals who have experienced trauma. Trustworthiness and transparency are crucial for building relationships, promoting healing, and recognizing the ongoing nature of trauma recovery.1 The shift from asking "What's wrong with you?" to "What happened to you?" is a fundamental aspect of TIC.2 This shift acknowledges that individuals' behaviors and challenges are often rooted in their experiences of trauma, rather than personal failings or deficits. The core principles of TIC provide a foundation for creating trauma-informed environments and practices.
Pennsylvania's Trauma-Informed Care Evolution
Pennsylvania has made significant strides in implementing TIC through various initiatives and collaborations. The PA Care Partnership has been instrumental in promoting trauma-informed practices, working closely with OCYF.3 OCYF has also been a driver of TIC implementation in Pennsylvania. OCYF has integrated trauma-informed principles into its policies and practices and has provided training and resources to support the adoption of TIC in child welfare and juvenile justice systems. This has included the development of a trauma screening tool4, the implementation of evidence-based trauma interventions5, and the promotion of family engagement and youth voice in decision-making processes.6 Efforts to promote safe, stable, and nurturing relationships and environments for children and families, as well as targeted support for youth at highest risk, are crucial in mitigating the negative impacts of trauma and promoting resilience and well-being.7
Trauma Training in Pennsylvania
Trauma training is a critical component of TIC in Pennsylvania for professionals serving children, youth, and young adults under age 26, Our shared goal is to help establish a trauma informed System of Care and Commonwealth in Pennsylvania.
The PA Care Partnership had previously established a strong working relationship with Lakeside Global Institute (LGI), a trauma training and education provider from Pennsylvania, and a leading provider of trauma training and consulting services.8 Beginning in 2019, the PA Care Partnership contracted with LGI to provide trauma-informed care workshops and training and development for the Trauma 101 Workshop Train the Trainer. They offer a range of trauma workshops designed to enhance professionals' understanding of trauma and equip them with practical skills for implementing trauma-informed practices when working with children and youth.8 These workshops are grounded in the latest research on trauma and resilience, and incorporate interactive, experiential learning activities to promote skill-building and application.
Examples of LGI's trauma workshops include:
Trauma 101: An Overview of Trauma-Informed Care, Trauma 102: Basic Skills of Trauma-Informed Care, Trauma 103: Recognizing Vicarious & Secondary Trauma for Caregivers, Trauma 104: Grief and Trauma, Trauma 105: Intro to Trauma for Parents & Caregivers, Trauma 106: An Introduction to Trauma for Youth, Trauma 107: Trauma-Informed Cultural Sensitivity, Trauma 108: Trauma and Racism, Trauma 109: Trauma in a Pandemic, Trauma 110: The Impact of Social Media.
Through PA Care Partnership’s funding throughout June of 2021, about 14,430 individuals received trauma training using LGI’s training workshops.
In Fiscal Year 2023, the PA Care Partnership, OCYF, and OMHSAS collaborated to provide comprehensive trauma training for professionals in Pennsylvania's child welfare system.3 By leveraging existing contracts, resources, and braided funding, these organizations maximized their impact and reached to effectively support children and families impacted by trauma.
By building upon their existing partnership with LGI, the PA Care Partnership, OCYF, and OMHSAS efficiently and effectively implemented a series of Trauma Workshops and Enhanced Trauma Training sessions tailored to the needs of child welfare professionals. This collaboration resulted in 10,150 individuals participating in 369 workshops, each lasting two-four hours, between FY21 and FY24.
In addition to these workshops, LGI offers intensive trauma courses that allow participants to earn certifications as Trauma-Sensitive Professionals. These courses include:
- Enhancing Trauma Awareness (ETA), Deepening Trauma Awareness (DTA), Applying Trauma Principles (ATP), Train the Trainer to Deliver Trauma Workshops and Trauma-Sensitive Certification (TSC).
These intensive courses deepen participants' understanding of trauma and equip them with practical skills to apply trauma principles in their work with children and youth. Between FY21 and FY24, 1,064 participants attended 81 intensive trauma course workshops. The impact of this collaboration and braided funding approach has been significant. The wide reach and effectiveness of the training initiative demonstrate the commitment of all involved parties to promoting trauma-informed care within the child welfare system. As the collaboration continues into FY24, the PA Care Partnership and OCYF remain dedicated to expanding access to trauma training.
This collaborative effort between the PA Care Partnership, OCYF, OMHSAS, and LGI serves as a model for how organizations can come together to address the complex needs of trauma-impacted children and families. By leveraging existing partnerships, braiding funding, and working towards a common goal, these organizations have demonstrated the power of collaboration in creating a more trauma-informed and responsive child welfare system in Pennsylvania.
Conclusion
Adopting Trauma-Informed Care requires a commitment from organizations and individuals to create safe, supportive environments that promote healing and resilience for children and youth in Pennsylvania. As the Commonwealth continues to lead the way in TIC implementation through collaborative initiatives, it is crucial for stakeholders and policymakers to invest in trauma-informed practices that support the well-being of young Pennsylvanians. By investing in trauma-informed initiatives and collaborating across sectors, Pennsylvania can create a more compassionate, resilient, and economically robust Commonwealth that supports the healthy development and thriving of all its young residents.
References
1. Substance Abuse and Mental Health Services Administration. (2014). SAMHSA's Concept of Trauma and Guidance for a Trauma-Informed Approach. HHS Publication No. (SMA) 14-4884. Rockville, MD: Substance Abuse and Mental Health Services Administration. SAMHSA’s Concept of Trauma and Guidance for a Trauma-Informed Approach.
2. Harris, M., & Fallot, R. D. (2001). Envisioning a trauma‐informed service system: A vital paradigm shift. New directions for mental health services, 2001(89), 3-22. Envisioning a Trauma-Informed Service System: A Vital Paradigm Shift Journal Article.
3. PA Care Partnership. (2024). Trauma-Informed Training. PA Care Partnership's List of Trauma-Informed Trainings.
4. Creating Trauma-Informed and Healing Centered Residential Care. Pennsylvania Department of Human Services. Available from: An Organizational Assessment Tool for Human Service Providers in Pennsylvania.
5. Family First Prevention Services Act Presentation. PA CASA. Available from: Family First Prevention Services Act Presentation by Jonathan Rubin, Deputy Secretary of the Office of Children, Youth, and Families (OCYF).
6. OCYF Launches Pennsylvania Meaningful Family Engagement Toolkit. Pennsylvania Providers. Available from: Family Engagement Toolkit /Bartlett, J. D., & Steber, K. (2019). How to implement trauma-informed care to build resilience to childhood trauma. Child Trends. Building Resilience to Childhood Trauma.
7. Lakeside Global Institute. (2024). Trauma Workshops. Lakeside Training Workshops.
8. Health Care Toolbox (n.d.) Health Care Toolbox: Helping Children and Families Cope with Illness and Injury.
Biography
Mark B. Durgin, B.S. Criminal Justice, has 20+ years in PA's child-serving systems. A certified trainer in Coach Approach to Adaptive Leadership, Adaptive Leadership for System Change, and Trauma Workshops, he champions coaching and leadership to empower individuals and improve mental/behavioral health and substance use coordination. As PA Care Partnership Project Director, Mark oversees the statewide System of Care Grant, fostering collaboration. His advocacy promotes the system of care philosophy and enhances communication at all levels. An Associate Partner at Coach Approach Partners and Keystone Leadership Coaching President, Mark influences through coaching, training, and presenting. Initiatives like the Statewide Grant Directors Community of Practice reflect his belief in understanding diverse viewpoints.
Beck | 23-32
Volume 13 ► Issue 2 ► September 2024
Trauma and Social Adversity in Autism: Considerations and Directions for Clinicians and Researchers
Kelly B. Beck
Keywords: Autism, trauma, post-traumatic stress disorder (PTSD), minority stress, trauma-informed care, assessment
Autism spectrum disorder is a neurodevelopmental disability characterized by differences in social communication and behaviors that is associated with lifelong challenges in social relationships, independence, and emotional well-being. In particular, autistic people have very high rates of lifetime mental health diagnoses, with two to ten times higher rates of co-occurring mental health diagnoses compared to non-autistic people. Death by suicide is the leading cause of premature mortality among autistic adults without intellectual disability.1,2 These negative trajectories start early, with some autistic children first attempting suicide as young as seven years old.3 1,4 Despite these alarming statistics, autistic people are frequently denied or removed from care due to the complexity of their psychiatric challenges, and some adults have reported that the lack of appropriate mental health supports has led them to consider suicide.5,6 As such, autism has been described as the “blind spot in mental healthcare”.7
Only recently has autism research begun to consider the powerful influence of the environment on mental health outcomes among autistic people. Published prevalence estimates of traumatic events (i.e. exposure to actual or threatened death, serious injury, sexual violence8) vary but are uniformly high in autism.9–11 Autistic youth are two to three times more likely to experience peer victimization, violence, and neglect than non-autistic peers.9,12 Specifically, autistic children are bullied and approximately 40% experience sexual victimization.10 Among adults, one recent study found that 75% of autistic adults reported having experienced physical or sexual abuse in their lifetime, and another study found that 84% of autistic people experience multiple forms of adverse childhood experiences, such as abuse and victimization.11 Reasons for this heightened risk are not well understood, but several mechanisms have been suggested. Differences in communication and social behaviors likely increases vulnerability for peer victimization by non-autistic peers and/or caregivers.10,13,14 Further, many autistic youth have clinically elevated emotion dysregulation (i.e. difficulty managing emotions) that is associated with the need for crisis services, involuntary hospitalizations, and police interactions, ultimately creating more opportunities to experience traumatic events.15
Autistic people also experience reoccurring social adversity (e.g. social contextual stressors, including excess stress people from marginalized groups experience, as a result of their inferior social status16), which may further compound the impact of exposure to potentially traumatic events.17–19 Examples of social adversity include experiences of discrimination, prejudice and stigma, invalidation, and social rejection.17 Inherent to autism is difficulty adhering to social and communication norms set by the neurotypical majority. Given this, it is not surprising that autistic youth and adults report to frequently experiencing social adversity in the form of stigma, discrimination, invalidation, and social rejection because of their autistic traits and lower social status.19,20 Discrimination and stigma among autistic people is significantly associated with more emotion dysregulation, higher suicidality, lower self-esteem, and lower quality of life.18,21 In a recent study with autistic adults, discrimination was a key contributor to emotion dysregulation, which led to some potentially traumatic events of involuntary sedation, termination of healthcare services, and police involvement.22 Another recent study found that reoccurring trauma and social adversity exposure had a cumulative effect on trauma symptom presentation among autistic people, demonstrating the importance of considering the additive nature of social adversity experienced by autistic people.23,24 Further, many autistic people cope with social adversity by attempting to mask or hide their autistic traits in order to meet neurotypical social norms, which we know to be predictive of worse mental health outcomes and heightened risk for suicide.25–28 Taken together, autistic people are both at heightened risk for traumatic exposure and experience reoccurring social adversity, which likely contributes to their alarming rates of suicidal thoughts and behaviors.
Despite these disparities in exposure to trauma and social adversity, it remains unclear how many autistic people develop post-traumatic stress disorder (PTSD).13,29,30 Some recent research suggests that autistic people are more likely to develop PTSD following adverse childhood experiences and traumatic events than neurotypical peers, though the research is still emerging and mechanisms why that may occur are unknown.13,14 Recent work suggests an overlap in symptoms and neurobiological networks impacted by both autism and PTSD.31,32 Others posit that challenges with neurocognitive and affective processes (e.g. working memory, cognitive inflexibility, rumination) and social perception common in autism increases vulnerability for both PTSD and suicidality following trauma and adversity.24,33–35 Further, autistic people appear to have reduced resiliency to the impact of adverse childhood experiences and traumatic events due to restricted social networks and difficulty maintaining relationships.
Assessment remains a key barrier to identifying and treating PTSD among autistic people. Differential diagnosis is challenging, as several key symptoms of PTSD overlap with core autistic features, and autism traits impact the presentation of trauma symptoms.14 For example, decreased attachment, flattened affect, repetitive play or speech, and withdrawal are all symptoms of PTSD and common social behaviors among autistic children and adults.14,36 Autistic adults without intellectual disability most commonly report symptoms of re-experiencing and hyper-vigilance.14 Yet symptom identification among autistic people with co-occurring intellectual disability remains difficult due to communication challenges, with aggressive behavior and running away being the most common responses following sexual trauma.29,30 While the field lacks validated tools for differential diagnosis, providers can refer to recently published tools and checklists by Michna and colleagues.23 Upon intake, clinicians should explore histories of exposure to traumatic events and ongoing social adversity, given that exposure to traumatic events and discrimination heightens risk for both PTSD and suicidal thoughts and behaviors.37 Providers are encouraged to assess the timing of symptom presentation (i.e. following a traumatic event or during a developmental period) and consider any sudden regression of skills that an autistic child or adult previously had (e.g. sudden loss of communication or increased withdrawal or aggression).23,30 In a recent study by Kerns and colleagues, ten key indicators of PTSD in autism were identified, including: physiological reactivity after trauma reminders, avoidance of trauma reminders, involuntary or intrusive memories, increase in emotion dysregulation, persistent avoidance, increased irritability or aggression, persistent trauma related emotions, increased suicidality, and new or worsened sleep disturbance.36
Trauma-informed care for autistic people remains a critical area for further exploration among clinicians and researchers alike. While intervention research on trauma in autism is still emerging, trauma-focused cognitive behavioral therapy and mindfulness interventions have growing evidence as appropriate options for autistic people with trauma histories or symptoms.38,39 Providers should individualize these interventions to meet the unique cognitive, sensory, and communication needs of each autistic client, as some of those treatments were not designed for neurodivergent needs.38,40 Further, several transdiagnostic treatments focusing on emotion regulation were designed specifically for autistic people and their caregivers.41 While these interventions have yet to be tested for PTSD symptom reduction specifically, there is strong evidence that these interventions improve shared symptomology.41 Thus, autism specific emotion regulation interventions are likely a good fit for autistic people that are experiencing social adversity and have trauma histories. In regard to social adversity, clinicians should also consider focusing on practical and realistic ways for autistic people to manage ongoing social adversity. For example, working with autistic people to identify and advocate for easily accessible safe places (e.g. quiet, sensory friendly space to go when dysregulated, feeling sensory overwhelm, or to use coping methods) and supporting people in all contexts of their daily living.22 Clinicians may also consider working with autistic people to identify internal signals of increasing distress, needing to safely cope and seek support.22 Finally, social connectedness and belonging are robust protective factors for trauma, social adversity, and suicidality in other populations.42–44 Supporting autistic clients to find autism-affirming social spaces, and form safe, social relationships online or in person should be a focus, regardless of therapeutic approaches.
In sum, it is imperative for clinicians and researchers to consider the impact of trauma and social adversity among children and youth on the spectrum, and related implications on their social and emotional wellbeing.
This manuscript was supported by the NICHD under Award Number L30HD109969, NIH under Award Numbers 1 P50 MH130957-01. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
References
1. Hirvikoski T, Mittendorfer-Rutz E, Boman M, Larsson H, Lichtenstein P, Bölte S. Premature mortality in autism spectrum disorder. Br J Psychiatry. 2016;208(3):232-238.
2. Joshi G, Wozniak J, Petty C, et al. Psychiatric comorbidity and functioning in a clinically referred population of adults with autism spectrum disorders: a comparative study. J Autism Dev Disord. 2013;43(6):1314-1325. doi:10.1007/s10803-012-1679-5.
3. Schwartzman J, Mcmorris C, Williams Z, et al. Elevated Suicidal Thoughts and Behaviors and Self-Injury in Autism Across the Lifespan: A Multinational Study.; 2024. doi:10.13140/RG.2.2.11256.66568.
4. Kirby A V., Bakian A V., Zhang Y, Bilder DA, Keeshin BR, Coon H. A 20-year study of suicide death in a statewide autism population. Autism Res. 2019;12(4):658-666. doi:10.1002/aur.2076.
5. Camm-Crosbie L, Bradley L, Shaw R, Baron-Cohen S, Cassidy S. ‘People like me don’t get support’: Autistic adults’ experiences of support and treatment for mental health difficulties, self-injury and suicidality. Autism. 2019;23(6):1431-1441. doi:10.1177/1362361318816053.
6. Maddox BB, Crabbe S, Beidas RS, et al. “I Wouldn’t Know Where to Start”: Perspectives from Clinicians, Agency Leaders, and Autistic Adults on Improving Community Mental Health Services for Autistic Adults. Autism Int J Res Pract. 2020;24(4):919-930. doi:10.1177/1362361319882227.
7. Lipinski S, Boegl K, Blanke ES, Suenkel U, Dziobek I. A blind spot in mental healthcare? Psychotherapists lack education and expertise for the support of adults on the autism spectrum. Autism. Published online November 26, 2021:13623613211057973. doi:10.1177/13623613211057973.
8. Diagnostic and Statistical Manual of Mental Disorders: DSM-5TM, 5th Ed. American Psychiatric Publishing, Inc.; 2013:xliv, 947. doi:10.1176/appi.books.9780890425596.
9. Holden R, Mueller J, McGowan J, et al. Investigating Bullying as a Predictor of Suicidality in a Clinical Sample of Adolescents with Autism Spectrum Disorder. Autism Res. 2020;13(6):988-997. doi:10.1002/aur.2292.
10. Trundle G, Jones KA, Ropar D, Egan V. Prevalence of Victimization in Autistic Individuals: A Systematic Review and Meta-Analysis. Trauma Violence Abuse. 2023;24(4):2282-2296. doi:10.1177/15248380221093689.
11. Reuben KE, Stanzione CM, Singleton JL. Interpersonal Trauma and Posttraumatic Stress in Autistic Adults. Autism Adulthood. 2021;3(3):247-256. doi:10.1089/aut.2020.0073.
12. Hartley G, Sirois F, Purrington J, Rabey Y. Adverse Childhood Experiences and Autism: A Meta-Analysis. Trauma Violence Abuse. Published online December 1, 2023:15248380231213314. doi:10.1177/15248380231213314.
13. Haruvi-Lamdan N, Horesh D, Golan O. PTSD and autism spectrum disorder: Co-morbidity, gaps in research, and potential shared mechanisms. Psychol Trauma Theory Res Pract Policy. 2018;10(3):290-299. doi:10.1037/tra0000298.
14. Haruvi-Lamdan N, Horesh D, Zohar S, Kraus M, Golan O. Autism Spectrum Disorder and Post-Traumatic Stress Disorder: An unexplored co-occurrence of conditions. Autism Int J Res Pract. 2020;24(4):884-898. doi:10.1177/1362361320912143.
15. Conner CM, Golt J, Shaffer R, Righi G, Siegel M, Mazefsky CA. Emotion Dysregulation is Substantially Elevated in Autism Compared to the General Population: Impact on Psychiatric Services. Autism Res. 2021;14(1):169-181. doi:10.1002/aur.2450.
16. Meyer IH. Prejudice, Social Stress, and Mental Health in Lesbian, Gay, and Bisexual Populations: Conceptual Issues and Research Evidence. Published online 2007.
17. Botha M, Frost DM. Extending the Minority Stress Model to Understand Mental Health Problems Experienced by the Autistic Population. Soc Ment Health. 2020;10(1):20-34. doi:10.1177/2156869318804297.
18. Botha M, Dibb B, Frost DM. “Autism is me”: an investigation of how autistic individuals make sense of autism and stigma. Disabil Soc. Published online October 6, 2020:1-27. doi:10.1080/09687599.2020.1822782.
19. Han E, Scior K, Avramides K, Crane L. A systematic review on autistic people’s experiences of stigma and coping strategies. Autism Res. 2022;15(1):12-26. doi:10.1002/aur.2652.
20. Beck JS, Lundwall RA, Gabrielsen T, Cox JC, South M. Looking good but feeling bad: “Camouflaging” behaviors and mental health in women with autistic traits. Autism. 2020;24(4):809-821. doi:10.1177/1362361320912147.
21. Han E, Scior K, Avramides K, Crane L. A systematic review on autistic people’s experiences of stigma and coping strategies. Autism Res. n/a(n/a). doi:10.1002/aur.2652.
22. Beck KB, MacKenzie KT, Kumar T, et al. “The world’s really not set up for the neurodivergent person”: Understanding emotion dysregulation from the perspective of autistic adults. Autism Adulthood. Published online 2024.
23. Michna GA, Trudel SM, Bray MA, et al. Best practices and emerging trends in assessment of trauma in students with autism spectrum disorder. Psychol Sch. 2023;60(2):479-494. doi:10.1002/pits.22769.
24. Rumball F, Brook L, Happé F, Karl A. Heightened risk of posttraumatic stress disorder in adults with autism spectrum disorder: The role of cumulative trauma and memory deficits. Res Dev Disabil. 2021;110:103848. doi:10.1016/j.ridd.2020.103848.
25. Cassidy S, Bradley P, Robinson J, Allison C, McHugh M, Baron-Cohen S. Suicidal ideation and suicide plans or attempts in adults with Asperger’s syndrome attending a specialist diagnostic clinic: a clinical cohort study. Lancet Psychiatry. 2014;1(2):142-147. doi:10.1016/S2215-0366(14)70248-2.
26. Cassidy SA, Gould K, Townsend E, Pelton M, Robertson AE, Rodgers J. Is Camouflaging Autistic Traits Associated with Suicidal Thoughts and Behaviors? Expanding the Interpersonal Psychological Theory of Suicide in an Undergraduate Student Sample. J Autism Dev Disord. 2020;50(10):3638-3648. doi:10.1007/s10803-019-04323-3.
27. Higgins JM, Arnold SR, Weise J, Pellicano E, Trollor JN. Defining autistic burnout through experts by lived experience: Grounded Delphi method investigating #AutisticBurnout. Autism. 2021;25(8):2356-2369. doi:10.1177/13623613211019858.
28. Raymaker DM, Teo AR, Steckler NA, et al. “Having All of Your Internal Resources Exhausted Beyond Measure and Being Left with No Clean-Up Crew”: Defining Autistic Burnout. Autism Adulthood. 2020;2(2):132-143. doi:10.1089/aut.2019.0079.
29. Kildahl AN, Bakken TL, Iversen TE, Helverschou SB. Identification of Post-Traumatic Stress Disorder in Individuals with Autism Spectrum Disorder and Intellectual Disability: A Systematic Review. J Ment Health Res Intellect Disabil. 2019;12(1-2):1-25. doi:10.1080/19315864.2019.1595233.
30. Kildahl AN, Helverschou SB, Bakken TL, Oddli HW. “If we do not look for it, we do not see it”: Clinicians’ experiences and understanding of identifying post‐traumatic stress disorder in adults with autism and intellectual disability. J Appl Res Intellect Disabil. 2020;33(5):1119-1132. doi:10.1111/jar.12734.
31. Song Y, Zhao Y, Baranova A, Cao H, Yue W, Zhang F. Causal association of attention-deficit/hyperactivity disorder and autism spectrum disorder with post-traumatic stress disorder. Psychiatr Genet. 2024;34(2):37. doi:10.1097/YPG.0000000000000357.
32. Kitamura S, Matsuoka K, Takahashi M, et al. Association of adverse childhood experiences and cortical neurite density alterations with posttraumatic stress disorder symptoms in autism spectrum disorder. Front Psychiatry. 2023;14:1215429. doi:10.3389/fpsyt.2023.1215429.
33. Allen KJD, Bozzay ML, Edenbaum ER. Neurocognition and Suicide Risk in Adults. Curr Behav Neurosci Rep. 2019;6(4):151-165. doi:10.1007/s40473-019-00189-y.
34. Miranda R, Valderrama J, Tsypes A, Gadol E, Gallagher M. Cognitive inflexibility and suicidal ideation: Mediating role of brooding and hopelessness. Psychiatry Res. 2013;210(1):174-181. doi:10.1016/j.psychres.2013.02.033.
35. Williams ZJ, McKenney EE, Gotham KO. Investigating the structure of trait rumination in autistic adults: A network analysis. Autism. 2021;25(7):2048-2063. doi:10.1177/13623613211012855.
36. Kerns CM, Robins DL, Shattuck PT, Newschaffer CJ, Berkowitz SJ. Expert consensus regarding indicators of a traumatic reaction in autistic youth: a Delphi survey. J Child Psychol Psychiatry. 2023;64(1):50-58. doi:10.1111/jcpp.13666.
37. Shaff J, O’Keefe VM, Atkin AL, Wang X, Wilcox HC. Examining the unique impacts of Potentially Traumatic Experiences (PTE) and discrimination events on Post-Traumatic Stress Disorder (PTSD) and suicidal thoughts and behaviors among Multiracial/ethnic adults in the United States. J Affect Disord. 2024;347:51-56. doi:10.1016/j.jad.2023.11.035.
38. Peterson JL, Earl RK, Fox EA, et al. Trauma and Autism Spectrum Disorder: Review, Proposed Treatment Adaptations and Future Directions. J Child Adolesc Trauma. 2019;12(4):529-547. doi:10.1007/s40653-019-00253-5.
39. Hopwood TL, Schutte NS. A meta-analytic investigation of the impact of mindfulness-based interventions on post-traumatic stress. Clin Psychol Rev. 2017;57:12-20. doi:10.1016/j.cpr.2017.08.002.
40. White SW, Conner CM, Beck KB, Mazefsky CA. Clinical Update: The Implementation of Evidence-Based Emotion Regulation Treatment for Clients with Autism. Evid-Based Pract Child Adolesc Ment Health. 2021;6(1):1-10. doi:10.1080/23794925.2020.1796551.
41. Beck KB, Conner CM, Breitenfeldt KE, Northrup JB, White SW, Mazefsky CA. Assessment and Treatment of Emotion Regulation Impairment in Autism Spectrum Disorder Across the Life Span. Child Adolesc Psychiatr Clin N Am. 2020;29(3):527-542. doi:10.1016/j.chc.2020.02.003.
42. Mournet AM, Wilkinson E, Bal VH, Kleiman EM. A systematic review of predictors of suicidal thoughts and behaviors among autistic adults: Making the case for the role of social connection as a protective factor. Clin Psychol Rev. 2023;99:102235. doi:10.1016/j.cpr.2022.102235.
43. Elbogen EB, Molloy K, Wagner HR, et al. Psychosocial protective factors and suicidal ideation: Results from a national longitudinal study of veterans. J Affect Disord. 2020;260:703-709. doi:10.1016/j.jad.2019.09.062.
44. Malone KM, Oquendo MA, Haas GL, Ellis SP, Li S, Mann JJ. Protective Factors Against Suicidal Acts in Major Depression: Reasons for Living. Am J Psychiatry. 2000;157(7):1084-1088. doi:10.1176/appi.ajp.157.7.1084.
Biographies
Kelly Beck, Ph.D., LPC, CRC, is an Assistant Professor of Psychiatry at the University of Pittsburgh. She is a rehabilitation scientist and Licensed Professional Counselor that works clinically with individuals with disabilities across the lifespan. Her specialty is using participatory research methods to design and test mental health interventions for autistic people. Dr. Beck is a co-developer of the Emotion Awareness and Skills Enhancement Program (EASE), a mindfulness-based intervention for autistic adolescents and young adults with and without co-occurring intellectual disability. She studies the impact of social adversity and trauma on mental health outcomes among autistic people. Dr. Beck is the Director of the Pittsburgh Adult Autism Research Community Collaborative for the Pitt Autism Center of Excellence that focuses on understanding mental health and suicide risk in autistic adults. She also leads the Schools Unified in Neurodiversity project, a community research project that designed a training program on fostering inclusive public-school environments for neurodivergent children. Dr. Beck received her Ph.D. in Rehabilitation Science from the University of Pittsburgh.
Contact Information
Kelly B. Beck, Ph.D.
Department of Psychiatry
School of Medicine
University of Pittsburgh
406 Sterling Plaza
201 North Craig Street
Pittsburgh, PA 15213
Phone: 1-412-383-6727
Email: kellybeck@pitt.edu
Hall & Do | 33-40
Volume 13 ► Issue 2 ► September 2024
Utilization of Art Therapy in Processing Overwhelming Emotions for Individuals with Autism Spectrum Disorder
Caitlyn M. Hall & Jennifer Do
Art Therapy and Trauma
Within the realm of trauma, art therapy has been clinically proven to support the processing and healing of trauma. Expressive art therapy allows individuals to tell their stories of stressful and traumatic events through non-verbal communication by allowing the senses and body to be a part of treatment.1 Often, talking about a traumatic event can be overwhelming for individuals, particularly children, who may also lack the language to describe what is happening to them. Art “provides emotional distance from the actual event and provides an alternative outlet to confront unresolved trauma memories through the use of symbols and media” (p. 8)2. In other words, art acts as a buffer between the individual and the traumatic event experienced, creating a safe environment.2 This is also true for individuals with Autism Spectrum Disorder (ASD) and/or neurodivergence. Art therapy allows for a mind-body connection and healing through movement and the senses.1
A study was conducted to examine the impact that art therapy has in processing traumatic events for those diagnosed with post-traumatic stress disorder (PTSD), primarily those who have experienced combat.3 The study found that there was a trend in reduced depression and PTSD symptoms for these individuals after art therapy sessions.3 Other studies looked at the impact of art therapy on young school-aged children who have had experience with trauma in a variety of contexts, including bullying and domestic violence.4 They found that early intervention utilizing art therapy can help prevent or lessen the chances of suicide and addiction later in life and reduce trauma symptoms.4 These findings support the conclusion that art therapy is beneficial in processing traumatic events.
Case Example
This case study took place at the Watson Institute Social Center for Academic Achievement (WISCA) Program. The Watson Institute has long served students with disabilities and their families. The Watson Institute is a specialized school that provides support for a diverse population of individuals ranging from ASD, down syndrome, physical disabilities, and other related mental disabilities. Each student enrolled has an Individualized Education Program (IEP) that supports their individual needs, capabilities, and growth. The Watson Institute’s mission is to “help children with special needs achieve their fullest potential in all aspects of their lives.”5 While at the school, individuals partake in daily living skills, executive functioning development, social skill groups, and academics.
The Watson Institute Social Center for Academic Achievement (WISCA) is a specialized program within the Watson Institute that is tailored to support individuals with ASD. The goal of this program is to integrate individuals who are neurodivergent, specifically children, teens, and young adults diagnosed with ASD or a pervasive developmental disorder (PDD), back into the traditional school setting. Individuals within the program can have co-occurring mental disorders such as attention deficit hyperactivity disorder (ADHD), obsessive compulsive disorder (OCD), oppositional defiant disorder (ODD), receptive and expressive language disorders, and anxiety. Due to our students' unique needs and our program's therapeutic goals, we permit specialized therapeutic activities, including specific types of drawing and interactions, to be integral components of our program. Mental health services, including art therapy, were provided to these students within the programming and are supervised by Jennifer Do, MEd, MA, ATR-BC, LPC. Rachel Gagen, MA, AT, LPC, provided Caitlyn with on-site supervision.
The following is a case example of Clover.
“Clover,” pseudonym, is a 14-year-old cisgender male who was diagnosed with a primary disability of emotional disturbance and secondary disabilities of ASD and speech impairment. Clover struggled with emotional regulation and appropriate expression of emotions. When experiencing unpleasant emotions, such as anger or becoming emotionally heightened, he would engage in verbal and, at times, physical aggression. Clover struggled with expressing his internal world and processing situations verbally. Clover also had experience with bullying, which he expressed greatly affected him. He expressed that some were so severe that it has caused him trauma and to be untrusting of others.
Antecedent Event
During a group therapy session, Clover became emotionally overwhelmed after another student destroyed his most prized possession, a stuffed plushie, which had previously been a source of bullying for him. While participating in a group art therapy activity, the other student drew on Clover's plushie with a black permanent marker. This triggered Clover's fight or flight response, causing him to become highly distressed and leave the classroom.
Behavior
When Clover became emotionally overwhelmed, he attempted both verbal and physical aggression toward the targeted student. While students gave Clover space, he was still visibly distressed and continued to pace, make threats, and destroy property, displaying trauma responses like hypervigilance, emotional explosiveness, and difficulty concentrating. He expressed feelings of being trapped in a recurring pattern, likening the situation to past experiences of bullying. Despite attempts by the therapist to communicate verbally, Clover was unreceptive due to his heightened emotional state. After time and space were given, the therapist introduced art materials with kinesthetic and somatic properties to help him process his emotions non-verbally, as art therapy can offer a safe way for individuals with trauma to express themselves without words.2
Use of Art Therapy
Art therapy allowed Clover to express and work through his emotions in a non-verbal, kinesthetic way, which aided in his processing of what he was experiencing. Art therapy allows the unconscious to surface while creating and discussing what came up for them through art. To begin, the therapist presented Clover with a kinesthetic outlet by presenting him with paper and number two pencils to rip and break. This allowed Clover to physically release some of the energy he was experiencing, a catharsis. However, Clover was becoming increasingly angrier with each tear and break. Utilizing the artistic properties of fixed art materials, such as colored pencils and markers, which allow the individual to have more control over what they are creating and manage anxiety, the therapist presented paper and markers.6
Clover drew four images using black and red markers. Each image Clover drew showcased a different way of him seemingly inflicting harm on the other student. Though the images may appear violent, it was essential to allow Clover to express himself authentically and fully process what was occurring for him, past and present. Once the images were drawn, Clover processed them with the therapist. However, before beginning, Clover found a box and placed his plushies inside it. He then repeatedly wrapped the box with tape to seal it from further harm. This tied to the connection between mind and body as the repetitive wrapping of the tape gave him a sense of control and safety through kinesthetic movement.
The first image showcases Clover cutting the student in half, with himself protecting his LightBulb plush. The second image showcases himself ripping the heart out of the other student to allow them to feel what he felt: heartbroken. When discussing this, he expressed that he could defend LightBulb but, at the same time, blame them for what happened. The therapist and Clover discussed who was responsible for what happened, a way to channel and focus those feelings on what occurred, and aid in the ability to process the trauma and feelings.
Overall, Clover has made noticeable progress in managing his emotions and processing traumatic experiences through art therapy. While discussing the images he created, Clover shared that drawing his feelings allowed him to process them more effectively than using words, likely influenced by his ASD diagnosis. He found that expressing his frustrations through art provided an alternative outlet that words could not, and he appreciated the sense of control and pressure the markers gave him, especially when he felt internally out of control. Seeing his emotions visually represented on paper helped him reflect on his experiences, enabling him to distance himself from the event while discussing it and developing coping strategies for future intense emotions.
Clover's ability to return to an emotional baseline while drawing, along with his self-reported improvement after creating the four images, demonstrates the effectiveness of art therapy in his case. This approach has not only supported the processing of his current intense feelings and trauma responses but has also begun to challenge his perspectives on similar situations. Through art therapy, Clover has learned to express himself in ways that words alone could not achieve, fostering a mind-body connection that has been crucial in his emotional regulation. The sense of control he gained through the use of markers has empowered him to manage his emotions better and respond more constructively in the future. In many ways, this therapeutic process has helped him begin to address and heal from the current incident and past traumas, marking a significant step forward in his emotional development and resilience.
Conclusion
Art Therapy can impact the processing of intense, overwhelming emotions and past traumas. Specifically, how impactful it can be for individuals who are neurodivergent. The way a neurodivergent brain processes emotional stimuli is structurally and functionally different, takes longer to process, and requires different modes of communication and skills to support them in processing experiences.7 Art therapy allows clients to access unconscious material, which can aid in the processing and resolving of past and present experiences, as well as intense emotions. The case of Clover highlighted how art can help support understanding and working through these experiences in a non-verbal, non-threatening way, a way that words alone would be unable to do.
References
1. Malchiodi, C. (2020). Trauma and expressive arts therapy: Brain, body & imagination in the healing Process. Guilford Press.
2. Ong, K. & Smith, J. (Sep 2023). Developments in art therapy for mental health. Seattle Anxiety Specialists – Psychiatry, Psychology, and Psychotherapy. Retrieved from Developments in Art Therapy for Mental Health.
3. Campbell, M., Decker, K. P., Kruk, K., & Deaver, S. P. (2016). Art Therapy and
Cognitive Processing Therapy for Combat-Related PTSD: A Randomized Controlled
Trial. Art Therapy, 33(4), 169–177.
4. Helping Kids Cope with Trauma. (October 20, 2017). Cedars-Sinai. Art Therapy Helps Children Cope with Trauma | Cedars-Sinai.
5. The Watson Institute. (2022). Mission, vision, and values. Retrieved from The Watson Institute.
6. Mehlomakulu, C. (Jan 2013). Media choices in therapy. Creativity in Therapy. Retrieved from Creativity in Therapy.
7. Shyman, E. (2017). Please wait, processing: A selective literature review of the neurological understanding of emotional processing in ASD and its potential contribution to neuroeducation. Brain Sciences, 7(11), 153. doi: 10.3390/brainsci7110153.
Biographies
Caitlyn M. Hall, MA, ATR-P, is a Mental Health Therapist at the Watson Institute's WISCA Program, where she has dedicated the last three years to working with individuals with Autism. With a total of four years of experience in the field, Caitlyn has developed a deep understanding of the unique challenges and strengths of her clients. She earned her Master’s degree in Art Therapy with a Specialization in Counseling from Seton Hill University, following her undergraduate studies at West Virginia University, where she received a Bachelor of Science in Psychology with a Minor in Ceramics. Caitlyn is passionate about integrating creative therapeutic approaches into her work, and she considers her current article to be her most significant professional accomplishment to date.
Jennifer Do, MEd, MA, ATR-BC, LPC, Thew Watson Institute WISCA Program, Program Director, WISCA, has a Bachelor of Arts Degree in Art Therapy from Mercyhurst University and a Master’s Degree in Art Therapy with Counseling Specialization from Seton Hill University. She obtained her Master’s Degree in Education with her Certification in Special Education from Carlow University. She is currently a doctoral student in Special Education at Slippery Rock University. She began her career as a mobile therapist working with individuals on the autism spectrum. She later moved into outpatient therapy and seeing individuals through private practice.
Contact Information
Caitlyn M. Hall
Phone: 412-914-8800
Email: CaitlynH@thewatsoninstitute.org
Jennifer Do
Phone: 412-741-1800, ext. 6444
Email: jenniferdo@thewatsoninstitute.org