Positive Approaches Journal, Volume 13, Issue 2
Positive Approaches Journal | 10-13

Volume 13 ► Issue 2 ► September 2024
Data Discoveries
The goal of Data Discoveries is to present useful data using new methods and platforms that can be customized.
In our last issue, [1] we shared definitions of trauma, the circumstances under which it may manifest, and common physical and psychological trauma responses, including cardiovascular issues and anxiety disorders. There is some evidence that autistic people may be more likely to experience potentially traumatic events (PTE) and to develop post-traumatic stress disorder (PTSD) compared to non-autistic people.1,2 Some studies have examined the prevalence of PTSD among autistic individuals using measures of self-reported frequency of exposure to trauma and self-reported PTSD symptoms. For example, one study found that 45% of individuals on the autism spectrum reported symptoms of trauma, indicating probable PTSD, compared to only 4.5% of the sample without autism.3
These quantitative studies exploring the prevalence of PTSD among individuals on the autism spectrum have been based on relatively small, homogenous samples that are not nationally representative. One avenue of discovery to address this data gap is to use large, population-based samples to explore prevalence of autism and co-occurring conditions. National Medicaid claims present a unique opportunity to do this and to identify trends across years and variations within subgroups.
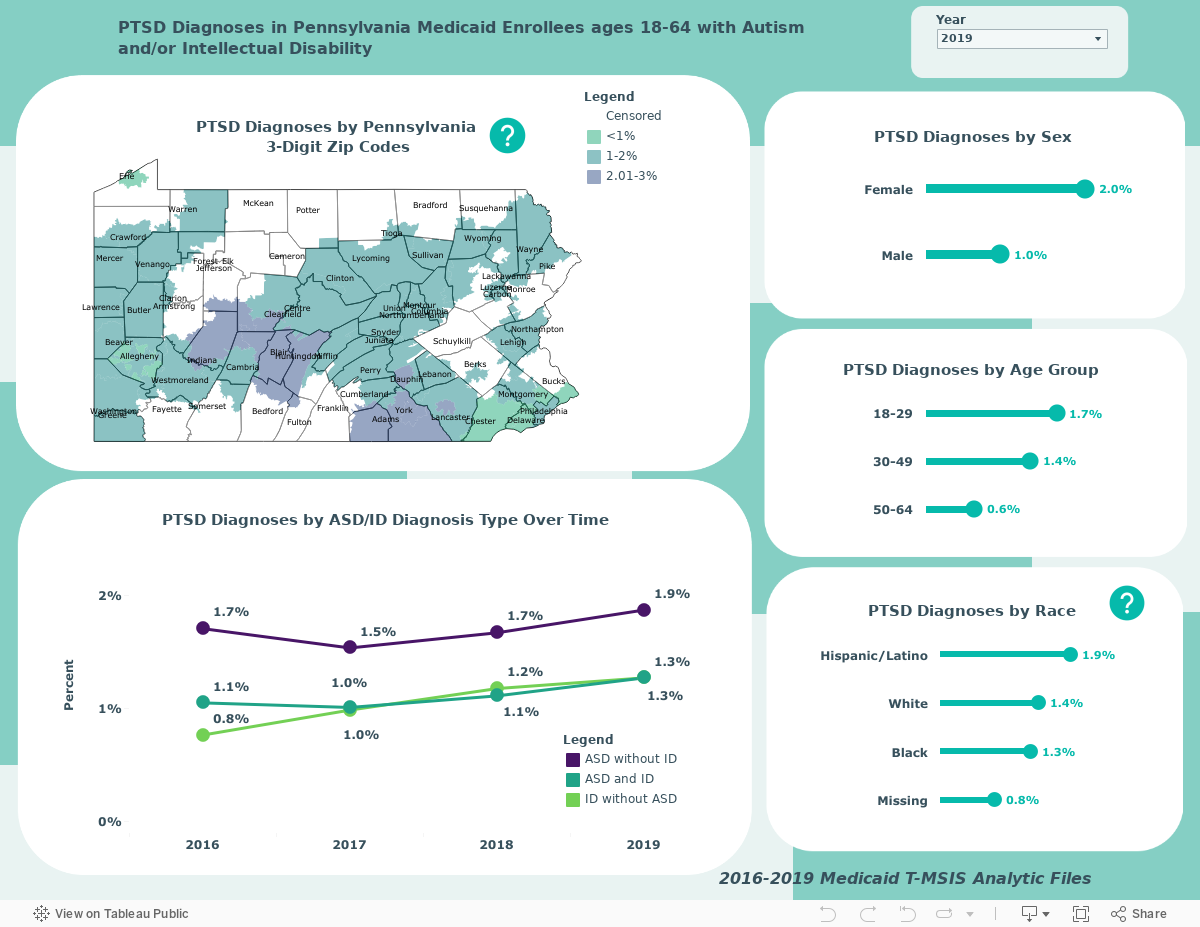
The dashboard below displays rates of PTSD among autistic Pennsylvania Medicaid enrollees between 18 and 64 years old with and without intellectual disabilities (ID) as well as enrollees with ID only. These rates differ from the small sample, self-reported studies because they do not measure PTSD in the same way. Using guidelines from the Chronic Conditions Data Warehouse, PTSD was defined here as having at least one inpatient or two other non-prescription claims associated with a PTSD diagnosis code. The benefit of this approach is that it allows for more reliable observations over time and between demographic groups. However, it is important to note that the data displayed here is derived from administrative claims data. [2] The overall sample sizes for each year are 49,675 (2016), 60,949 (2017), 62,719 (2018), and 61,191 (2019).
Data reflects Medicaid claims files from 2016-2019 and are derived from the Centers for Medicare and Medicaid Services (CMS) Transformed Medicaid Statistical Information System (T-MSIS) Analytic Files (TAF) personal summary and service claims files. Data may be filtered by year to explore changes in these rates over time and across Pennsylvania counties, sex, age group, and race.
Conclusions
While the data displayed here are exploratory, there are some noteworthy trends that indicate an urgent need for further research, clinician training, and increased awareness. Rates of PTSD ranged from 1-2% between 2016 and 2019 and there is a noticeable uptick in the rates among all groups and within subgroups. The highest rate of PTSD was observed in autistic people without ID (1.9% in 2019) and the lowest rate was observed in people with ID only (0.8% in 2016). Rates of PTSD were highest among women, those in the 18–29-year-old age group, and those who identified as Hispanic or Latino. Within Pennsylvania, among counties with data that is not censored, the highest rate of reporting PTSD was observed in Adams County in 2019 (3.6%).
It is also important to note the differences between the rates of PTSD observed here based on services claims and the rates found in other smaller studies that are based on self-reporting of PTSD symptoms. Results here may be an indication that autistic individuals are not receiving appropriate or sufficient support for PTSD. There are also important disparities within this sample that warrant further investigation: higher PTSD rates among women, those who are younger, and minoritized populations indicate a need to tailor services and treatment options to these groups. Researchers should prioritize analyses examining differences in rates of PTSD within these sub-populations of individuals with Intellectual and Developmental Disabilities (IDD). Findings can be translated into resources and training opportunities for providers and other clinicians, to improve understanding of trauma and how to best support individuals on the autism spectrum who are experiencing trauma and its effects.
The Autism Services Education Resources and Training Collaborative (ASERT) provides key trauma resources for providers, individuals, families, and communities (see the dashboard of key resources in the last issue of this journal). [3]
References
1. Ng-Cordell E, Wardell V, Stewardson C, Kerns CM. Anxiety and trauma-related disorders in children on the autism spectrum. Current psychiatry reports. 2022;24(3):171-180.
2. Peterson JL, Earl RK, Fox EA, et al. Trauma and autism spectrum disorder: Review, proposed treatment adaptations and future directions. Journal of child & adolescent trauma. 2019;12:529-547.
3. Rumball F, Brook L, Happé F, Karl A. Heightened risk of posttraumatic stress disorder in adults with autism spectrum disorder: The role of cumulative trauma and memory deficits. Research in Developmental Disabilities. 2021;110:103848.