
Positive Approaches Journal, Volume 10, Issue 1
Murray & Northridge | 51-61

Volume 10 ► Issue 1 ► May 2021
Social Skills for the “Real World”:
Lessons
Learned from the Autism Services, Education, Resources and Training (ASERT)
Social Skills Groups
Michael
J Murray, MD and Jesse Northridge, LCSW
Abstract
Social skills challenges are one of the core deficits associated with autism spectrum disorder (ASD) and have been consistently identified as an area of high need on the ASERT Needs Assessment. This article reviews important components of effective social skills intervention to help staff intervene and address identified challenges for those with ASD. The ASERT Social Skills Programs are discussed including some of the findings from the adult program. The article concludes with a “Top 10 Tips” list to consider when planning social skills interventions.
Social connectedness is an important factor in overall health and wellness. The COVID-19 pandemic has revealed the wide health disparities in our country and the enhanced vulnerability from poorly integrated social networks that many individuals with Intellectual and Developmental Disabilities (IDD) experience. This article reviews the structural and functional components of strong social networks, including a review of different types of social capital. Suggestions for evaluating and strengthening social networks according to an individual’s expressed goals are offered.
___
The 2011 Pennsylvania Autism Needs Assessment conducted by ASERT found social skills training as among the most commonly reported unmet core need across the lifespan.1 The updated 2018 Pennsylvania Autism Needs Assessment conducted by ASERT revealed an ongoing need for social skills training access, and found that only 43% of individuals spend some time with friends. Time spent with friends varied from a high of 6.8 hours per week for those 0-5 years old to a low of 3.9 hours per week for those 31-35 years old.2
Social skills differences are the core challenge for ASD. Differences with fluently decoding social information and executing appropriate responses can become more impairing as individuals with ASD age given the increase in demands of social interactions and the increasing expectation of mastery of these skills. Adolescents are particularly vulnerable to struggle with social connectedness with peers as their social environment rapidly changes with increased emphasis on social communication (both verbal and non-verbal). Despite these needs, there is little empirical evidence for best practices for improving social interaction skills for adolescents and adults with ASD.3
In recognition of the high need for improving service access and to establish treatment efficacy, ASERT developed manualized social skills interventions for adolescents (ages 13-18) and for young adults (ages 18-30). A literature review found a significant improvement in targeted social skills in 62.5% of studies with adolescents and young adults with ASD that utilized modeling, scripting, direct instruction, prompting, and role play as social skills interventions.4 In order to capitalize on these findings, the ASERT social skills groups employed direct instruction utilizing video modeling (both prepared and self-modeling) paired with peer generalization during naturalistic social activities. Outcomes included self-report, caregiver-report, and behavioral observations.
Video modeling is helpful in that it provides a visual representation of the skill in context to a situation. In other words, the discussion expands to not just talking about “how” to greet someone but also “when” and “why.” Verbal and non-verbal communication strategies can be highlighted. A variety of models can be presented demonstrating varying degrees of proficiency (e.g. some examples demonstrating skills done well and some examples where there could be improvement). These variations help the individual gain a deeper understanding of the mechanics of the interaction/social skills. Furthermore, demonstrating alternative skills based on different hierarchies/social roles (e.g. greeting your boss vs. greeting your uncle) and degree of familiarity (e.g. the more structured greeting for someone you are initially meeting vs the typically informal greeting for someone you know well) in the different examples helps develop mastery. Periodically obtaining and viewing self-models where participants watch videos of themselves executing different skills can lead to greater insight and self-monitoring.
Peer generalization not only provides “real-world” practice, it helps promote generalization of skills which can be a significant barrier to social skills intervention.5,6 Additionally, peer generalization allows for greater social validity
of instruction and targeted skills as peers can provide additional feedback to participants regarding the evolution of skills and social expectations. An example of this is the use of popular slang terms and idioms among the peer group.
Finally, targeted skills should match the participant’s goals. The ASERT social skills groups were aimed at individuals who desired more friendships and/or to feel more comfortable in social situations. All were able to use spoken language to maintain
conversations with others. This curriculum focused on verbal and non-verbal social conversation skills. This curriculum would not be appropriate for someone who communicated differently or whose goals were different such as learning to cope better
with sensory hypersensitivities in social interactions. Furthermore, outcome measures should reflect these goals. As improved non-verbal social communication was one of the things targeted in the pilot study of this intervention, amount of eye contact
in a 5-minute interaction with a novel peer was tracked as an outcome measure. As shown in Figure 1, the amount of eye contact—shown in green—did statistically and significantly improve (p=.002) for the 29 study participants from pre-intervention
(average of 144 seconds) to post-intervention (average of 177 seconds) to 3-month follow-up (average of 186 seconds).
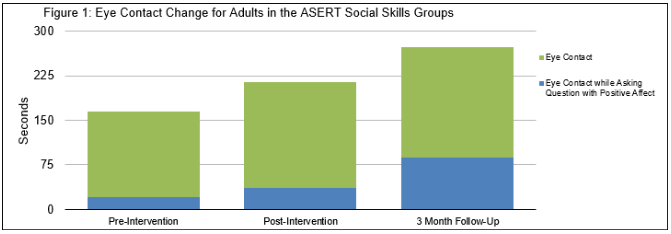
However, when thinking of communication and social impact, eye contact is even more important when you are asking a question during
a social interaction. Furthermore, doing so while having a positive affect (smiling or conveying interest) is even more impactful as it lets the other person know there is interest in their response. This reflects the “when” and “why” of social skills
mentioned previously. This high-impact eye contact—shown in blue—also demonstrated statistically and significant (p=<.001) growth across the three 5-minute observation periods. Preintervention the study participants averaged 21 seconds of
this high-impact communication. This increased to an average of 37 seconds and, perhaps most encouraging, this increased to an average of 87 seconds at the 3-month follow-up observation. These findings demonstrate that there was substantial growth
in this skill following their participation in the group and indicate successful generalization of skills.
Though this data requires a lot of time and effort to collect and analyze, its principles can be applied to clinical practice. For instance, if an individual has identified improving their ability to maintain social conversations as a goal, measuring
the length of conversation with peers would provide some feedback on progress—the “how.” However, working through the “when” and “why” of this goal with the individual may reveal hopes to use this skill to develop more friendships. In that situation,
a more nuanced— “high-impact”—way of measuring progress might be determined which would not take a lot of extra effort. Progress and success could be measured through the length of dialogue and number of open-ended questions the individual asked peers.
Increasing both conversation duration and the number of asked open-ended questions may effectively convey interest in the other person. Similarly, increasing conversation duration but declining number of asked questions may provide the individual
with valuable information as to what may be going wrong in their attempts at establishing friendships.
The following are suggestions for enhancing the impact of social skills interventions. While they are based on the experience of the ASERT team conducting social skills groups for adolescents and adults with ASD, most—if not all—of them are generalizable
to other social skills challenges not related to ASD.
Top 10 Tips for Leading an Effective Social Skills Group
1.
Break it down. Break it down. Break it down.
a. Social interactions are incredibly complex. There are hundreds of muscles throughout the body and over forty in the face. Subtle movements in these muscles can communicate important details in the course of a conversation. For example, Guillaume Duchenne documented how two facial muscles, the zygomatic major muscle and the orbicularis oculi muscle, work together to communicate genuine joy and amusement.7 When these muscles are not engaged, others have a propensity to view it as simply a “polite” smile. For an individual on the autism spectrum, recognizing these subtleties can be a Herculean task. When trying to help someone learn or improve social skills, it is frequently necessary to break down skills and concepts into smaller components. Individuals can then be instructed how to interpret situations based on which social cues are present.
2. Emphasize a take-away point.
a. For many individuals on the spectrum, there can be too much information to absorb within the timeframe of a group therapy session. For individuals who have difficulty in this type of learning environment, identifying a key message or concept for them to remember can be helpful for content retention. This concept should be reviewed several times throughout the session in order to promote learning through repetition. Even if other information is forgotten, emphasizing a take-away point can help increase the likelihood that key concepts are remembered and practiced.
3. Include more socially proficient peers.
a. There is a sizable difference between awareness of a skill and being able to use it effectively. The appropriate application and generalization of social skills can be incredibly challenging for individuals with autism. When groups are limited to others with social challenges, individuals may not recognize how the use or misuse of skills would impact social interactions outside of the group. The addition of more socially proficient peers for the purposes of practice and generalization can be highly impactful. Furthermore, many group participants have self-reported that opportunity to practice with peers is highly valuable and appealing.
4. Manipulate dyads.
a. When including peers and planning activities for social skills practice, consider how personalities and skill levels can be manipulated for growth. For example, pairing individuals who are both naturally shy could potentially motivate one of them to become more active in the interaction. Encouraging someone with significant social deficits to work with someone with strong interpersonal and leadership skills can be a great way of helping to further develop social communication skills. All dyads will have benefits and drawbacks. Be mindful of these dynamics and consider how you can manipulate them to promote skill development.
5. Allow individuals to critique their own interactions.
a. Upon viewing a recording of their social interactions, most individuals invariably notice aspects about their verbal and non-verbal communication they were unaware of in the moment. For example, some may recognize the overuse of verbal commentary or that they have a highly rigid body posture. Because social interactions are so complex, it can be difficult for individuals—particularly individuals with autism— to recognize all of the cues present in a situation. They also may not recognize how their own non-verbal cues are influencing the interaction. Although few individuals enjoy scrutinizing videotaped recordings of themselves, these recordings provide great opportunities to gain insight into skill strengths and needs. Depending on the skills being targeted, it may be beneficial to construct situations where these skills are needed. For example, individuals learning about effective interview skills could be videotaped during a mock interview. After the recording is complete, group leaders can help the individual to identify social cues present in the interaction as well as review which skills were used effectively/ineffectively.
6. Get everyone involved.
a. Many individuals who participate in social skills groups prefer discussion-style format, but this style of instruction can present challenges. Some group members may become overly passive and others may try to dominate the conversation. However, over-direction questions to group members may dissuade an individual from sharing relevant information or even sustaining their attention until it is “their turn.” To deal with this, it is recommended that group leaders periodically shift the target of their questions between specific individuals and the larger group.
b. Group leaders should also utilize different types of questions. For example, open-ended questions can be a great way of inviting ideas, general observations, and discussion of personal experience. However, some individuals may feel these questions are too broad and difficult to answer. Conversely, closed-ended questions are typically much simpler to answer, but may limit the amount of discussion on a topic. Group leaders can also use probing questions to help group members identify appropriate social information or hypothetical questions to consider how skills could be applied in alternative situations.
7. Give the group some control.
a. Group members tend to be more interested and engaged if they have a sense of ownership over the group. Seek feedback from group members about their preferences and allow the group to make decisions whenever possible. For example, there could be many different scenarios and activities available for individuals to practice targeted skills. Allowing the group to decide the activity will provide another “real-world” social communication opportunity and may lead to greater investment in the practice.
8. Tailor materials to the group.
a. All therapy interventions, particularly those which are highly manualized, carry concerns about fidelity. Significant modifications to the curriculum may weaken the effectiveness of the intervention. However, rigid adherence to the manualized treatment risks group members not understanding key concepts and skills. Sometimes, modifications can be helpful and appropriate if group members are struggling to understand material. Some group members may need additional review of core concepts. At times, group members may raise questions not directly related to the curriculum but may be highly relevant to their needs and/or experiences. By staying attuned to the group’s abilities and interests, group leaders can help members stay engaged with the material and maximize their learning.
9. When possible, try to use at least two group leaders.
a. Having a second group leader allows for easier multitasking and addressing any emerging needs during the session. As one leader leads the discussion, the other group leader can prepare the next activity. If an individual in the group requires one-on-one attention, support can be given without disrupting the entire group process.
10. Consider the benefits of snacks.
a. Abraham Maslow described a hierarchy of needs and described physiological needs as a necessity before other human motivations can take place. 8 Indeed, when hunger and other needs are not met, it can be difficult for individuals to focus on other tasks. Providing snacks is an easy way of helping individuals stay in a proper headspace during sessions.
Conclusion
In summary, social skill interventions are an area of high need for many individuals with ASD and other neurodevelopmental needs, and these needs typically persist across the lifespan. Additionally, social skills increase in complexity and nuance as individuals age; skills interventions need to reflect this. Helping individuals understand the proper context of skills expression—the “when” and “why”—can help promote generalization and adaptive functioning. Consider the power of video modeling, the critical benefit of peer generalization and other social exposures, and crafting outcome measures which truly reflect the skill’s socially valid expression when working on social skills. These efforts are time well-spent. Improved socially functioning can be a critical factor in increasing adaptive behaviors, greater community participation, more robust person-centered goal-setting, and risk reduction for victimization.
References
1. Pennsylvania Autism Needs Assessment: A Survey of Individuals and Families Living with Autism, Report #2: Service Needs. ASERT website. https://needs.paautism.org/wp-content/uploads/2020/05/Needs-Assess_ServiceNeeds_Sept-2011_M.pdf. Published 2011. Accessed May 4, 2021.
2. Pennsylvania Autism Needs Assessment: A Survey of Individuals and Families Living with Autism, Explore the Data: Social & Spirituality. ASERT website. https://needs.paautism.org/explore-the-data/social-spirituality/. Published 2018. Accessed May 4, 2021.
3. Reichow B, Volkmar F. Social skills Interventions for individuals with autism: Evaluation for evidence-based practices within a best evidence synthesis framework. J Autism Dev Disord. 2010;40(2):149-166.
4. Roth M, Gillis J, DiGennaro RF. A meta-analysis of behavioral interventions for adolescents and adults with autism spectrum disorders. J Behav Educ. 2013;23(1):258-286.
5. Rao P, Beidel D, Murray M. Social skills interventions for children with Asperger’s syndrome or high-functioning autism: A review and recommendations. J Autism Dev Disord. 2008;38(2):353-361.
6. White S, Keonig K, Scahill L. Social skills development in children with autism spectrum disorders: A review of the intervention research. J Autism Dev Disord. 2007;37(10):1858-1868.
7.
Duchenne GB. The Mechanism of Human Facial
Expression. New York, NY: Cambridge University Press; 1990. Maslow AH. A theory of human motivation. Psychol Rev. 1943;50(4):370–396.
8. Maslow AH. A theory of human motivation. Psychol Rev. 1943;50(4):370–396.
Biography
Michael Murray, MD is an associate professor of Psychiatry and Behavioral Health at Penn State College of Medicine. He is the director of the division of Autism Services for Penn State Health and the director of the central region ASERT collaborative. He is the creator of the Multi-Media Social Skills Program for Adolescents and the Multi-Media Social Skills Program for Adults—the ASERT social skills curriculums.
Jesse Northridge, LCSW is a licensed clinical social worker. He is part of the clinical team at the Autism and Developmental Disorders Clinic in the Department of Psychiatry for Penn State Health. In addition, he is a team member for the central region ASERT collaborative. He is the lead therapist for the ASERT social skills groups.
Contact Information
Michael J. Murray, MD
Penn State Health / Central ASERT
717-531-1115