
Positive Approaches Journal, Volume 10, Issue 2
Zortman, Morris, & Vivaldi | 55-66

Volume 10 ► Issue 2 ► August 2021
Use of Remote Monitoring to Positively Impact Individuals by Removing the Struggle Between the Person and Their Supports
Anne Zortman, MS,
Timothy W Morris, and Meredith Vivaldi
Abstract
A common misconception in the field of Intellectual and Developmental Disabilities (IDD)/Dual Diagnosis is to automatically add supports and services when someone is engaging in maladaptive behaviors. However, for someone where the impetus for maladaptive behavior is driven by control and creating chaos in their environment, less support can be more impactful in effective change. This article will review how remote monitoring and other positive strategies can be implemented to support a person with Borderline Personality Disorder and IDD to remove the struggle taking place between the person and his supports.
[Borderline
Personality Disorder] occurs in the context of relationships. Unlike other
psychiatric diagnoses, if you put someone with schizophrenia on an island all
by themselves, their mental illness would still be evident. If you put someone
with BPD on an island, you wouldn’t necessarily see the symptoms — whatever
happens, happens in the context of [interacting] with someone else.
--Dr. Perry Hoffman1
___
Introduction
Supporting people diagnosed with both intellectual disabilities and mental health disorders often presents unique challenges. Those challenges can be increasingly complex when a personality disorder is present. The symptoms of personality disorders materialize in the context of relationships. More specifically, Borderline Personality Disorder is marked by interpersonal disturbances2. People diagnosed with Borderline-Personality-Disorder inherently display more argumentative, antagonistic, and less cooperative behaviors3. These behaviors can create barriers to functioning in social relationships, including relationships with those in a supportive role3. When a person engages in ongoing discord and hostility in their interactions with supportive services, the unique challenge becomes maintaining the therapeutic value of the support without becoming the source for conflict. This dynamic calls for an inventive approach to find that balance.
Case Study
Grayson was adopted at 14 months of age; however, not much else is known about his life prior to age 13. At the age of 13, he began a series of psychiatric inpatient hospitalizations and ongoing psychiatric care. During this time, he was diagnosed with mild intellectual disability (ID), borderline personality disorder (BPD), anxiety disorder (AD), and bipolar disorder (BD). When Grayson became an adult, he received services from multiple agencies, often changing providers as the result of unsuccessful discharges. His services varied from living in community homes to living independently with In-Home and Community Supports services. Grayson displayed a consistent pattern of high-risk aggressive behaviors including property destruction, physical assault, terroristic threats, and allegations against supporters. Although he is articulate and is independent across many areas of functioning, he could not effectively navigate or maintain healthy social relationships, including those with his adoptive family His relationships were marked by his volatile reactions to perceived mistreatment or lack of respect. These perceptions resulted in acts of vengeance in the form of physical aggression, homicidal threats, and allegations of abuse or neglect. In 2016 at the age of 35, Grayson was placed on probation for making terroristic threats. During this time he also returned to the care of his adoptive brother after being discharged from a community home due to physical and verbal aggression. Although he reports that he very much valued his relationship with his brother, he was not able to maintain a healthy relationship with him and manifested old patterns of behavior. He threated to “shoot up” his brother’s home and was incarcerated for 30 days following this threat. The court recommended that he be placed in a community home to address his ongoing behavioral support needs. Grayson moved into a community home in July 2018 but by June 2019, the provider determined they were no longer able to support him. He then chose to move into a community home with Person Directed Supports (PDS).
When Grayson started services with PDS, he presented with his historical behavioral patterns of verbal and physical aggression, terroristic threats, property destruction and allegations against supporters. An initial functional behavioral assessment was completed during his first 60 days of service with PDS. This initial assessment involved direct observation of Grayson by the behavior specialist, interviews with Grayson and his supporters, review of records related to his psychosocial and developmental history, and review of behavioral data collected daily by support staff. Behavioral data collected included the time each behavior occurred, duration of the behavior, what had occurred prior to the behavior, description of actual behavior, strategies used to address the behavior, the response to strategies, anything else that was effective in de-escalating the behavior, and what Grayson did once he was deescalated. The initial Functional Behavioral Assessment indicated that Grayson’s maladaptive behaviors serve social functions in the form of obtaining attention and escape/avoidance. Social attention was the most common outcome of his various provocative and threatening statements and the severity of his statements increased when attention was not immediately given. He also effectively utilized physical aggression and elopement to escape non-preferred situations and tasks. After several months of continued observation of Grayson, ongoing interviews with supporters, and analysis of the behavioral data, themes around his behaviors became evident. He sought control and a feeling of power in his dynamics with others and that interpersonal conflict with supporters facilitated that sense of control. He displayed hypervigilance against perceived mistreatment or not being respected by supporters. It was hypothesized that Grayson operates from a core belief that he lacks worth and will not be respected. The behavioral data indicated that he was creating this narrative with his direct support staff and it was evident that adding additional support resulted in increased conflict. In an effort to reframe how he views supports, our team at PDS began looking into ways to change the role of supporters and to change the form of supervision without reducing the level of support Grayson would require. Our goal was to shape supports in a way that he could value the relationship with his supporters instead of seeking conflict with them.
Initially, Grayson moved into a home with two other individuals and received 2:1 staffing supports. He immediately struggled sharing his living environment and expressed his desire to live more independently. He made ongoing attempts to turn support staff against one another to create discord. Police involvement, psychiatric inpatient hospitalizations, and numerous self-reported allegations of abuse and neglect increased. To mitigate the conflict, Grayson moved into a 1-person community home with PDS, and staffing supports were reduced to 1:1. Despite the change in environment and level of support, he continued his pattern of dysfunctional interpersonal dynamics. Supporters grew wary of working with him due to frequent self-reported allegations and investigations that required supporters to be on leave. It was evident that a different approach in supporting Grayson with his complex behavioral needs and strong desire for independence was needed. We hypothesized that continued reduction of in-person supports, while still accounting for safety, would lead to a balanced situation where he could focus on living his life independently and remain receptive to help from supports in doing so. This led us to investigate using technology to aid in supervision and reduce the amount of in-person support provided.
An independence plan designed to incrementally build up to remote monitoring was developed and proposed to Grayson. We also collaborated with our administrative entity, supports coordination organization, Pennsylvania’s Office of Developmental Programs’ (ODP), and state licensing staff to finalize the details of the plan. The plan started with staff engaging in active and passive staffing at varied timeframes to simulate the conditions of remote monitoring without removing staff from the property. During passive staffing conditions, staff remained in a designated area of the home and would only interact with Grayson if there was an emergent need. The intention of the incremental plan was to slowly back away in-person support without sudden change as transitions can be a trigger for him. Having staff remain on site but in a passive mode that was not accessible to Grayson created an unintended power struggle between him and staff likely due to perception of abandonment as the staff are still in the home but not interacting with him. This was an important observation, further confirming his interpersonal distortions and functions of his behaviors. The incremental nature of the initial plan also was difficult for him to follow and predict as there were contingencies attached. Multiple steps prevented him from settling into the plan and kept his focus on the power struggles and changes versus making progress and skill acquisition. The focus remained on chaos in relationships. In order to address Grayson’s continued desire for full independence while also considering his need for clear, predictable relationship boundaries, we created a more concrete, structured plan that went directly into remote monitoring.
The remote monitoring plan combined
direct in-person supervision with off-site virtual supervision. To achieve
this, video cameras were installed near the ceilings in all common areas of the
home. Cameras were not installed in the bedroom or bathroom. Video was provided
continuously but not recorded. During remote monitoring hours, support staff
monitored the video feed at another home located approximately 15 minutes from
Grayson’s home. Grayson was also able to access supporters on a cell phone
designated for calls during times of remote monitoring. To develop the schedule
for in-person supervision hours in the home, multiple factors were considered.
The in-person hours needed to be during times when Grayson would want to
participate in activities inside and outside of the home and when it made sense
to have a supporter present to assist with tasks. The behavioral data was reviewed
to ascertain if there was an average length of time supporters were able to
work with Grayson before maladaptive behaviors occurred. Based on these
considerations, it was determined that he would receive a total of 8 hours of
in-person support each day. The 8 hours were divided into three separate
in-person shifts: 5:30 AM-7:30 AM, 11:00 AM-2:00 PM, and 5:00 PM-8:00 PM. These
timeframes encompassed medication administration times, his preferred times for
meals, and times when he would typically want to go out into the community. If
appointments were not able to be scheduled during the set in-person support
hours, supporters would leave the remote monitoring site to provide
transportation and assist with the appointment. After the appointment, he would
be transported home and supporters would return to the remote monitoring site
until the next in-person support time. Grayson often stated a desire to live
more independently. When developing the remote monitoring plan with him,
emphasis was placed on how replacing in-person supports with remote supports
created an environment for him to build those independent living skills while
supporters were not in the home with him. This helped him buy into the plan. Again,
we collaborated with the administrative entity, supports coordination
organization, ODP, and state licensing to ensure the team was in agreement and
all factors had been considered. Maintaining ongoing communication with this
larger team was vital to implementing the plan.
When the remote monitoring plan was launched, Grayson’s behaviors demonstrated a near immediate change. (See Figure 1 and Figure 2.)
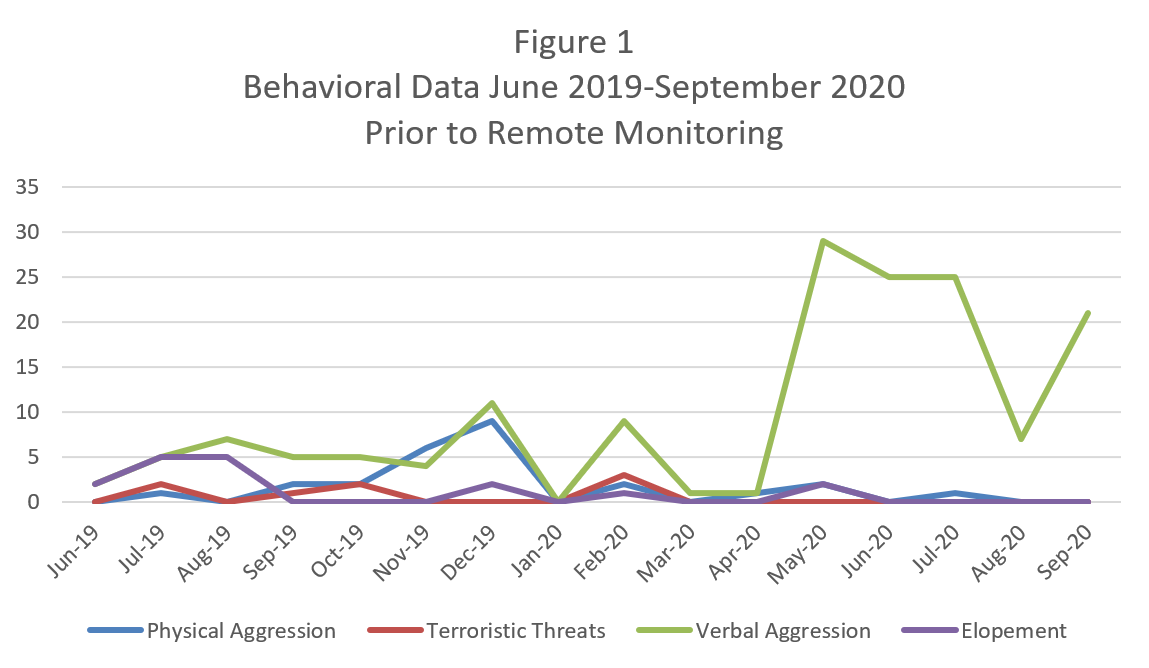
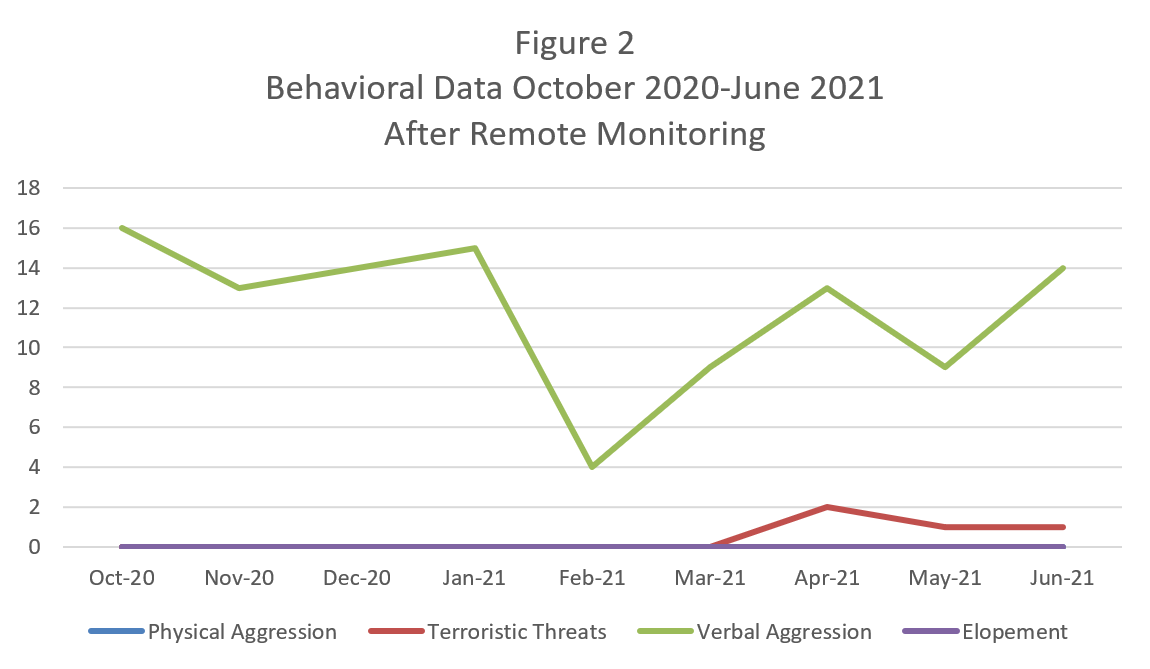
He stopped all terroristic threats toward his direct support staff. He no longer engaged in property destruction, eloped from the home, or made threats to harm himself. In the 9 months since the remote monitoring plan started, he has only engaged in physical aggression on one occasion and it was noted that this occurred during a period when staff were not able to utilize remote monitoring and had to implement the passive staffing schedule while on the property. Grayson continued to utilize some provocative language with the suspected function to obtain a reaction from his supporters. Instead of verbal threats to harm supporters, he shifted to making sexual comments, often in the form of jokes or songs, to see how supporters would respond. Supporters were consistently successful in redirecting him from his commentary and in-person staffing hours have been used with more intention and purpose. Interestingly, Grayson did not completely shed his narrative around his perception of not receiving respect and his related need to retaliate against that perception. He shifted his focus to members of the management team within PDS. This manifested in ongoing unsubstantiated allegations against those team members but not allegations against his supporter. In making PDS administrators the focus of his discontent, he has been more successful in navigating relationships with his supporters and building skills and interests that foster his independence. As intended, use of remote monitoring helped remove the conflict between Grayson and his supporters and created an opportunity for him to value his supporters in a way that had not previously occurred to him.
Conclusion
Grayson’s story demonstrates the
opportunity for increased innovations in supporting individuals with complex
behavioral presentations. High risk behaviors often seen in people with
Borderline Personality Disorder are rooted in social function and present a
unique challenge as the physical presence of support often provides the trigger
as well as the reinforcement. Additionally, these high-risk behaviors can
prevent an individual from achieving levels of independence they are otherwise
capable of achieving, resulting in increased frustrations with the levels of
support in place and making the supporter the target of that frustration. It is
often the case that as high-risk behaviors increase, the presence of support
also increases. With Grayson’s diagnosis of borderline personality disorder,
this only exacerbated his feelings of resentment toward his supporters and lead
to behaviors that not only stunted his progress but put him and his supporters
at further risk of harm.
The collaborative efforts of the state administrative entity, supports coordination organization, ODP, and licensing were key in designing this plan. Team meetings were held while designing the plan and then quarterly meetings were held once the plan was implemented. Email updates were also provided on an as needed basis. Keeping the team informed each step of the way ensured we were all on the same page and could problem-solve from an informed place. Taking a person-centered approach in addressing Grayson’s complex needs proved paramount to the overall success of the remote monitoring. Seeking to understand Grayson rather than participate in his narrative of opposition and conflict led to an outcome where he is able to engage in supportive services without putting himself or others at risk of harm. This experience is an example of not only how remote monitoring can be used to enhance the independence of people in supportive services, but also how it can restructure services for those who struggle with the interpersonal dynamics of support.
References
1. Villiant M. Most accurate article on BPD we have read—kudos. Borderline Personality Disorder.org website. https://www.borderlinepersonalitydisorder.org/most-accurate-article-on-bpd-we-have-recently-read-kudos/. Accessed June 10, 2021.
2. Hoffman
PD, Fruzzetti AE, Buteau E. Understanding and engaging families: an education,
skills and support program for relatives impacted by borderline personality
disorder. Journal of Mental Health 2007; 16 (1): 69-82.
3. Schmahl C, Herpertz SC, Bertsch K, et al. Mechanisms
of disturbed emotion processing and social interaction in borderline
personality disorder: state of research
agenda of the German clinical research unit. Borderline Personality Disorder
and Emotional Dysregulation 2014; 1(12);1-17. https://doi.org/10.1186/2051-6673-1-doi:10.1186/2051.6673.1.12. Published: September 2014. Accessed: June 10,
2021.
Biographies
Anne Zortman, M.S. is the Clinical Director of Behavioral Health Services for Person Directed Supports, Inc. She earned her Master’s in Clinical Psychology at Millersville University. Anne has worked in various areas of the mental health system including Adult Community Living Arrangements, Partial Hospitalization, Outpatient Therapy, and Behavioral Health Rehabilitative Services.
Timothy W Morris, graduated Manga Cum Laude from Shippensburg University with a Bachelor of Science, Major in History, Minor in Psychology. He has worked with adjudicated youth, as a Crisis Counselor at the Carlisle General Hospital, and has been with Person Directed Supports for over 19 years working with individuals with IDD and Dual Diagnosis. He also has two amazing sons, Layne and Tristan, who help him hone his behavior modification techniques as they continue to grow into fine young men.
Meredith Vivaldi is the Executive Director of Person Directed Supports. She has been with PDSI for almost 8 years and in the field for over 20 years. Meredith started working with children with varying disabilities and then moved into the adult population with PDSI. She is National Association of Developmental Disabilities (NADD) certified and specializes in dual diagnosis individuals. Outside of work Meredith enjoys traveling and being with family.
Contact Information
Anne Zortman
azortman@persondirectedsupports.com
717-729-3388
Tim Morris
tmorris@persondirectedsupports.com
717-372-8540
Meredith Vivaldi
mvivaldi@persondirectedsupports.com
610-509-7115