Positive Approaches Journal, Volume 11, Issue 3
| Site: | My ODP |
| Course: | My ODP |
| Book: | Positive Approaches Journal, Volume 11, Issue 3 |
| Printed by: | |
| Date: | Wednesday, August 5, 2026, 6:46 PM |
Positive Approaches Journal | 6-7

Volume 11 ► Issue 3 ► November 2022
Access, Empowerment, and Independence: Employment for All
Introduction
Having a job is more than just getting a paycheck. It is also about connecting to others, making friends, learning new skills, having structure in your life, and making a contribution to society. Having a job, earning an income, and paying taxes provide a wonderful feeling of independence; a feeling of pulling your weight. As one person with serious mental illness who is quoted in one of the articles of this Positive Approaches issue says, empowerment is defined this way: "It's a decent paycheck at the end of the week."
This issue of Positive Approaches focuses on the importance of employment for individuals with a disability – whether it is a serious mental illness, a developmental disability, intellectual disability, deafness, or something else. The issue discusses the programs that exist in Pennsylvania to help chip away at the high unemployment rate of these individuals. The national percentage of people with disabilities participating in our workforce is just 22.5 percent.
Officials in state government say that is unacceptable. That is why the Employment First Act was signed by Governor Tom Wolf in 2018, making competitive integrated employment the first consideration and preferred outcome for people with disabilities by law.
There are programs in Pennsylvania in support of that law that help individuals with disabilities to get and keep employment. One is the Office of Vocational Rehabilitation (OVR), in the Pennsylvania Department of Labor and Industry, which holds the sole responsibility for administering the state-federal Vocational Rehabilitation Program is one of the few available resources to combat the issue of low employment rates among the deaf population.
Another program is the Medical Assistance for Workers with Disabilities (MAWD) program in the Department of Human Services (DHS). The MAWD program supports individuals with disabilities by keeping them covered by Medical Assistance after they obtain employment. MAWD is more than just medical coverage; Medical Assistance acts as a doorway to a host of varied third-party agencies and services that provide wraparound supports to build up individuals.
Additionally, supported employment (SE) is the primary tool used to assist those with serious mental illness (SMI) to gain employment. And research has shown that the SE version to work most effectively for those with SMI is the Individual Placement and Support model.
It is important for individuals to not only get a job, but to keep that job and to feel like they are valued and respected for their contributions. For the sake of employees’ mental health and to create continuous quality improvement, organizations need to foster an environment of psychological safety. As described in one of our articles, psychological safety is “a climate where people feel safe enough to take interpersonal risks by speaking up, and sharing concerns, questions, or ideas.” Actions to establish such an environment, along with things like the Employment First Law, OVR, MAWD and SE, help to overcome barriers to competitive integrated employment for individuals with disabilities.
This issue will provide insight into how we can continue this important work.
David Knauss
Retired Human Services Analyst
Office of Long-Term Living
Positive Approaches Journal | 8-15
Volume 11 ► Issue 3 ► November 2022
Data Discoveries
The goal of Data Discoveries is to present useful data using new methods and platforms that can be customized.
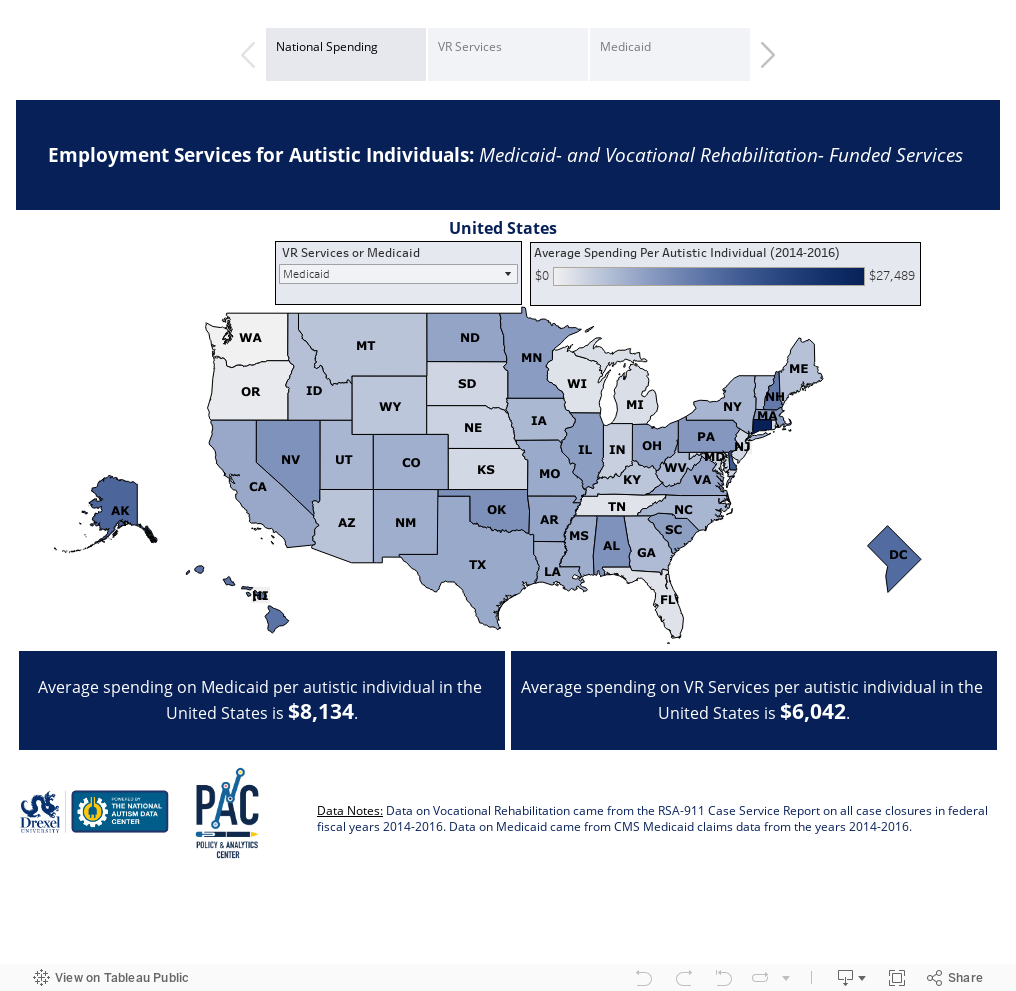
Employment is a critical aspect of everyday life. Employment has been shown to decrease the occurrence of mental health diagnoses and associated costs1 and also addresses the adverse effects of unemployment on standards of living, healthy behaviors, and financial hardship.2 Unfortunately, despite the known benefits to employment, there are high levels of unemployment, underemployment, and poverty among autistic individuals and other intellectual developmental disabilities (IDD).3-7 However, there are publicly funded services to support individuals with disabilities in preparing for, accessing, and maintaining employment including Vocational Rehabilitation (VR) and Medicaid home and community-based service (HCBS) waivers.8 The data dashboard below shows national and state-level data on spending and utilization of employment services funded through VR and through HCBS waivers.
Vocational Rehabilitation Services
Vocational Rehabilitation is available to job seekers with disabilities with a combination of state and federal funding. People with any numbers of disabilities who have demonstrated difficulty getting or keeping a job can be eligible for VR services. State-operated VR offices provide over 25 different services,9 which are offered based on the needs of the individual. Vocational Rehabilitation services include supports like career search, job placement, and on-the-job supports, in addition to training opportunity and supports in a postsecondary setting as preparation for employment. Data for this article came from all VR case closures in federal fiscal years 2014-2016 in the 50 states and Washington D.C. for applicants ages 14 and older. Highlights from these data include:
- 4.5% of all VR service users were individuals on the autism spectrum, ranging from 0.8% (Mississippi) to 9.5% (Minnesota).
- Of all individuals on the autism spectrum who applied to VR during this time, 70.0% went on to receive services from VR.
- VR spent a total of $227,649,019 on services and the average spending per autistic person during this period was $6,042.
Medicaid-funded Services
Medicaid HCBS waivers are commonly used by states as a mechanism to provide services and supports to people who are eligible on the basis of diagnosis, functional assessment, assets, and other areas as deemed by the state and approved in the application to the Centers for Medicare & Medicaid Services (CMS).17 Medicaid-funded employment services, which are largely provided through Medicaid HCBS waivers, include employment services that are focused both on prevocational preparation supports, often offered in segregated settings, and supported employment services including job search, placement, and on the job supports that occur in community settings. Data is from Medicaid claims for all 50 states and Washington D.C. for individuals on the autism spectrum in years 2014-2016. Additional criteria for inclusion in the analysis were being at least 14 years old and having been enrolled in Medicaid for at least nine months of a given year. Highlights from these data include:
- The national spending average on Medicaid for autistic individuals from the years was $8,134 per person.
- Average spending on employment services by Medicaid by state for autistic individuals varies from $677 (Oregon) to $27,489 (Connecticut).
- The national average for autistic Medicaid beneficiaries receiving employment services was 5.3%, ranging from 0.34% (Washington) to 24.83% (Delaware).
- The national average for autistic Medicaid enrollees receiving employment services had a co-occurring Intellectual Disability is 80%.
The data dashboard below shows national and state-level data on spending, service access, and utilization of employment services funded through VR and through Medicaid HCBS waivers.
The data dashboard below shows information on the prevalence of mental health conditions among the ID and ASD populations from peer reviewed research studies. The visual displayed on the first tab of the dashboard shows a timeline of publications from all peer-reviewed research focused on identifying mental health diagnosis occurrence among autistic individuals and individuals with ID. Each circle represents a publication, with the size and color indicating how often the article was cited by other research, which is an indicator of the impact or reach of that publication. To read the text, click on a circle to be directed to the abstract for each article and potential access options. The second tab shows the frequency of mental health condition co-occurrences among the respondents to the 2018 PANA. Together, these visuals demonstrate how research outside of Pennsylvania and among autistic Pennsylvanians has pointed toward understanding co-occurring diagnoses and supports how progress toward services for mental health diagnoses need to be accessed and delivered.
Conclusion
The Autism Services, Education, Resources, and Training Collaborative (ASERT) offers resources relevant to employment among individuals on the autism spectrum and with other IDDs. This includes the Employment Resource Collection which has a compilation of links focused on various aspects of employment and supports and #ASDNext Work Resources which are curated with a focus on transition age youth and young adults. One resource in particular, Employment Myths & Facts, is focused on clarifying commonly misunderstood areas of employment for people with disabilities. The Pennsylvania Office of Developmental Programs (ODP)’s MyODP web platform also offers employment resources centered around the Everyday Lives framework. Additionally, there are several National Autism Indicators Reports, published by the Life Course Outcomes Research Program at the AJ Drexel Autism Institute, with a focus on employment including the National Autism Indicators Report: Developmental Disability Services And Outcomes In Adulthood and the National Autism Indicators Report: Vocational Rehabilitation. Finally, the Additionally, there are several National Autism Indicators Reports, published by the Life Course Outcomes Research Program at the AJ Drexel Autism Institute, with a focus on employment including the National Autism Indicators Report: Developmental Disability Services And Outcomes In Adulthood and the National Autism Indicators Report: Vocational Rehabilitation. Finally, the State Employment Leadership Network hub is a network of state disability agencies and provides information, resources, and events focused on employment and Employment First policies.
Funding Statement
Data for this article are supported by funding from the National Institute of Mental Health (Grant Number: 5R01MH117653) and the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under cooperative agreement UT6MC45902 Autism Transitions Research Project. The information, content, and/or conclusions are those of the authors and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS, or the U.S. Government.
References
1. Bush PW, Drake RE, Xie H, McHugo GJ, Haslett WR. The long-term impact of employment on mental health service use and costs for persons with severe mental illness. Psychiatr Serv. Aug 2009;60(8):1024-31. doi:10.1176/ps.2009.60.8.1024
2. van der Noordt M, IJzelenberg H, Droomers M, Proper KI. Health effects of employment: a systematic review of prospective studies. Occupational and environmental medicine. 2014:oemed-2013-101891.
3. Stapleton DC, O'DAY BL, Livermore GA, Imparato AJ. Dismantling the poverty trap: Disability policy for the twenty‐first century. The Milbank Quarterly. 2006;84(4):701-732.
4. Whittle HJ, Palar K, Ranadive NA, Turan JM, Kushel M, Weiser SD. “The land of the sick and the land of the healthy”: disability, bureaucracy, and stigma among people living with poverty and chronic illness in the United States. Social Science & Medicine. 2017;190:181-189.
5. Shattuck PT, Narendorf SC, Cooper B, Sterzing PR, Wagner M, Taylor JL. Postsecondary education and employment among youth with an autism spectrum disorder. Pediatrics. Jun 2012;129(6):1042-9. doi:10.1542/peds.2011-2864
6. Shattuck PT, Lau L, Anderson KA, Kuo AA. A National Research Agenda for the Transition of Youth With Autism. Pediatrics (Evanston). 2018;141(Suppl 4):S355-S361. doi:10.1542/peds.2016-4300M
7. Zablotsky B, Black LI, Maenner MJ, et al. Prevalence and trends of developmental disabilities among children in the United States: 2009–2017. Pediatrics. 2019;144(4)
8. Hall AC, Freeze S, Butterworth J, Hoff D. Employment funding for intellectual/developmental disability systems. Journal of Vocational Rehabilitation. 2011;34(1):1-15.
9. Revision of PD-13-05 Vocational Rehabilitation Program Case Service Report (RSA-911) Data Elements (RSA-PD-14-101) (October 25, 2013).
10. Chen JL, Sung C, Pi S. Vocational Rehabilitation Service Patterns and Outcomes for Individuals with Autism of Different Ages. J Autism Dev Disord. Sep 2015;45(9):3015-29. doi:10.1007/s10803-015-2465-y
11. Nevala N, Pehkonen I, Teittinen A, Vesala HT, Pörtfors P, Anttila H. The Effectiveness of Rehabilitation Interventions on the Employment and Functioning of People with Intellectual Disabilities: A Systematic Review. J Occup Rehabil. 12 2019;29(4):773-802. doi:10.1007/s10926-019-09837-2
12. Nye-Lengerman K. Vocational rehabilitation service usage and outcomes for individuals with Autism Spectrum Disorder. Research in Autism Spectrum Disorders. 2017;41-42(July):39-50. doi:10.1016/j.rasd.2017.08.003
13. Nord DK, Stancliffe RJ, Nye-Lengerman K, Hewitt AS. Employment in the community for people with and without autism: A comparative analysis. Research in Autism Spectrum Disorders. 2016;24:11-16.
14. Migliore A, Timmons J, Butterworth J, Lugas J. Predictors of employment and postsecondary education of youth with autism. Rehabilitation Counseling Bulletin. 2012;55(3):176-184.
15. Kaya C, Chan F, Rumrill P, et al. Vocational rehabilitation services and competitive employment for transition-age youth with autism spectrum disorders. Journal of Vocational Rehabilitation. 2016;45(1):73-83.
16. Butterworth J, Migliore A, Timmons J. Services and outcomes for transition age young adults with autism spectrum disorders: Secondary analysis of the NLTS2 and RSA 911. 2010.
17. Shea LL, Koffer Miller KH, Verstreate K, Tao S, Mandell D. States' use of Medicaid to meet the needs of autistic individuals. Health services research. 2021;56(6):1207-1214. doi:10.1111/1475-6773.13671
Bush & Chambers | 16-22
Volume 11 ► Issue 3 ► November 2022
Medical Assistance for Workers with Disabilities (MAWD) in Action
Angelina Bush and Grady Chambers, Community Integrated Services
Pennsylvanians with disabilities who are in the workforce got some good news in July 2021, when Governor Wolf signed Senate Bill 156 into law as Act 69. Act 69 created Workers with Job Success (WWJS), an extension of the Medical Assistance for Workers with Disabilities program (MAWD), which helps working people with disabilities maintain their Medicaid-based insurance so they can continue to receive waiver services while earning significant income. The WWJS extension significantly increases the income limit for eligible individuals who are already enrolled in MAWD and eliminates any resource limit for those individuals. This enables workers with disabilities who receive Medicaid to earn a higher income without losing access to Medicaid coverage and the essential services that they receive from that benefit.
Community Integrated Services (CIS) is a supported employment provider operating in Southeastern Pennsylvania and the state of Delaware. We help people with disabilities find meaningful employment, connect them to a range of resources, and support them at work to help them succeed. The MAWD Program—and now the WWJS extension—is a useful though underutilized resource for the population we serve. The general knowledge is that people’s work income plus their benefits has to come out to $2,523 or less per month (the income limit to be eligible for Medicaid coverage). What people don’t often know is that if their combined income goes above that number, MAWD is a tool designed to help them in that very situation.
A little over
a year since Act 69 was signed, we are taking a look back to spotlight a couple
of ways MAWD and WWJS can be beneficial tools for working people with
disabilities, and to share a few takeaways we hope will be useful to other
service providers. Two brief stories drawn from the experiences of people we
serve nicely illustrate the efficacy of these resources.
Alex
One of the individuals we serve —we'll call him Alex—receives benefits counseling and on-site employment support from Community Integrated Services. He is also enrolled in the federal Ticket to Work program. Alex has significant medical needs, and his story underscores why the Medical Assistance for Workers with Disabilities Act is so critical. Alex was receiving $900 in Social Security Disability Insurance (SSDI) benefits prior to getting a new job as a Senior Analyst, which came with an annual salary of $97,000. Once Alex started working, his SSDI was terminated, and we faced the challenge of helping him find a way to maintain his Medicaid and waiver eligibility given his new and higher income bracket.
The MAWD program provided a
solution. Though Alex is earning nearly $30,000 more than the MAWD income limit
of around $68,000, we were able to show that, when accounting for Impairment
Related Work Expenses, his countable income would actually come out to less
than the cap, making him eligible for MAWD while protecting his access to
Medicaid. Without awareness of or access to this program, Alex would have been
forced to turn down the position or to ask for a significantly lower salary
than what he was offered for fear that his earnings would make him ineligible
for Medicaid, thereby losing accessing to the essential services he receives
from it. Because of the MAWD program, Alex is able to work full-time hours,
earn the salary his work deserves, all while maintaining access to vital
medical care through Medicaid. Once Alex is on MAWD for one calendar year, he
plans to move into the new Worker’s with Job Success extension enabled by Act
69, which will allow him to earn even more money than his starting salary while
maintaining his access to Medicaid.
Another change brought by the
WWJS extension is relevant here: while there is a $10,000 resource limit for individuals
to be eligible for the MAWD program, there is no resource limit for individuals
who become eligible for the Workers with Job Success extension. This means that
the bank accounts of WWJS participants can reflect the full extent of their
resources without putting them at risk of losing access to Medicaid or risking
their eligibility for their waiver.
Winston
A second participant—we'll call him Winston—receives benefits counseling from CIS and employment support from a different provider. Winston has autism and an intellectual disability and receives $1,940 in Social Security Administrations (SSA) benefits based off his parents’ work record. Winston works at IKEA, where he earns about $1,250 per month. Winston also has significant medical needs and requires support to live in his community.
Prior to his knowledge of MAWD
or being connected to that program, Winston might have assumed that he couldn’t
earn more than $583 per month if he wished to remain eligible for Medicaid and
his waiver services, which would have made it impossible for him to accept the
job at IKEA. But thanks to MAWD, he was not only able to accept the offer they
made him, but also has a much higher ceiling with respect to his future
earnings potential. Now Winston is able to work all his hours, continue to
receive his SSA benefits, and maintain his eligibility for Medicaid and waiver
services. Winston’s experience underscores the need for greater outreach to
increase awareness of these programs, and the ways in which they enable
individuals with disabilities to seek full employment without putting them at
risk of losing access to vital medical care through Medicaid.
Takeaways and resources
For those who might be interested in utilizing MAWD or WWJS, we’d like to spotlight a few important components of the programs and some things to keep in mind.
- How to count income. For individuals who are using or want to utilize MAWD, income is based off that individual’s countable income, not gross income.
- The MAWD program has a $10,000 resource limit (the resident’s property and one automobile are not considered countable resources) which is a higher resource limit than many other Medical Assistance programs.
- The WWJS extension to MAWD has an unlimited resource limit.
- People who use MAWD can still access waiver services. There is a common misconception that participation in MAWD will risk one’s eligibility for their waiver, which is not typically the case.
- MAWD should be the first consideration whenever someone has income over the typical waiver limit, rather than looking to reduce earnings.
- We would recommend more education about the various types of Medicaid assistance that are available, and their corresponding limits, as we’ve seen providers suggest MAWD to individuals on SSI benefits in situations where it’s not appropriate. The Pennsylvania Health Law Project is a great resource (phlp.org), as is the Pennsylvania Department of Human Resources, who put out this brochure on MAWD.
- Accessing MAWD will look differently depending on whether you have a waiver or if you’re just receiving Medicaid. For someone who wants to utilize MAWD only, they should complete the MAWD application. For someone who is using MAWD and also has a waiver, they should complete the usual Medical Assistance application and then the MAWD supplement form, rather than the MAWD application.
- If you’re interested in MAWD but feeling overwhelmed, don’t worry! While it can take a little bit to get comfortable navigating the process, MAWD and the Workers with Job Success extension are opening the door to greater employment possibilities for people with disabilities. Once someone is on MAWD, it tends to be smooth sailing.
Biographies
Angelina Bush serves as Assistant Director of Benefits Counseling, Angelina oversees a team of benefits counselors that help people understand their benefits, access services and resources available to them, ad make informed choices about work. Angelina began as an Employment Specialist in 2007 and has an in-depth knowledge of both employment services and government systems. Angelina earned a BA in Psychology from Rutgers University and was certified as a Community Partner Work Incentive Coordinator (CPWIC) in 2011through Virginia Commonwealth University Program. Angelina was the winner of the National APSE's Professional Award in 2016, earned for her renowned expertise in benefits counseling and the many hundreds of people she has served.
Grady Chambers is the Communications Manager at Community Integrated Services (CIS). He is the organization's primary grant writer, and is responsible for the bulk of of CIS's external and internal communications, as well as managing and maintaining its social media accounts.
Contact Information
Angelina Bush
Community Integrated Services
Assistant Director of Benefits Counseling and Ticket to Work
Grady Chambers
Community Integrated Services
Communications Manager
grady.chambers@cisworks.orgCipriani | 23-27
Volume 11 ► Issue 3 ► November 2022
“Employment First” Matters
Laura Cipriani, Policy Supervisor
Every October we celebrate National Disability Employment Awareness Month (NDEAM). National Disability Employment Awareness Month serves as a time to nationally recognize people with disabilities for their contributions to, and their important role in, a diverse and inclusive workforce.1 Despite progress that has been made to better support and promote employment for people with disabilities, the national percentage of people with disabilities participating in our workforce continues to be far lower than that of people without disabilities. 2
In 2018 in Pennsylvania, the Employment First Act was signed by Governor Tom Wolf making competitive integrated employment the first consideration and preferred outcome for people with disabilities by law. Competitive integrated employment is when a person with a disability is earning minimum wage or higher and working in a community setting where there is interaction with people that do not have disabilities.
Pennsylvania’s Office of Developmental Programs (ODP) believes that all people with an intellectual disability and/or autism must be encouraged to pursue their vision for an everyday life, which might include working in competitive integrated employment. Employment First is important to people with disabilities beyond just being the law. Competitive integrated employment offers people of all abilities an opportunity to earn money, learn new skills, build self-confidence, make friends, and be a part of their communities. In addition, research has shown that people who are unemployed have a higher prevalence of poor health than their employed counterparts.3
Pennsylvania’s Office of Developmental Programs has done a substantial amount of work to promote Employment First, and some of the key highlights include:
- Adding two new employment-related services: Advanced Supported Employment and Benefits Counseling.
- Allowing up to $15,000 worth of employment services to be added to a person’s plan without counting towards the funding limit of their P/FDS waiver.
- Developing and implementing two Memorandums of Understanding (MOU) with the Office of Vocational Rehabilitation (OVR). One of these MOUs funds a contact person in each OVR district office specifically designated to assist individuals with an intellectual disability and/or autism. The other MOU allows data sharing across agencies to better streamline service delivery.
- Increasing provider qualifications in employment-related services to increase the quality of services for individuals with disabilities. To support providers to meet the qualifications, ODP obtained access to the College of Employment Services, an online course approved by the Association of Community Rehabilitation Educators (ACRE) board, as a cost-efficient alternative to in-person courses.
- Delivering training and technical assistance from nationally recognized experts to 25 providers of facility-based services on how to transform their business model to support competitive integrated employment.
- Establishing an ongoing data collection system for competitive integrated employment and an “employment dashboard” for easy access to data.
- Serving on the leadership team for the statewide Community of Practice on Secondary Transition.
- Securing a contract with Cornell University to deliver the Work Incentives Practitioner Training and Credential Program to fifty persons working for provider agencies to become qualitied to deliver Benefits Counseling through Pennsylvania’s ODP funding.
- Using funds from the federal American Rescue Plan Act to award providers grants to fund Business Associates in Industry.
In 2017, the total number of working age people (ages 18-64) enrolled with Pennsylvania ODP that had competitive integrated employment was 5,114. In August of 2022, that number was 7,706 people, an increase of 51%.
There are many successes, both small and large to be celebrated, and yet there is much more work to do. For people with disabilities and their families, there are barriers to competitive integrated employment that don’t exist for people without disabilities. For example, accessing transportation, or fear of losing financial or medical benefits. Pennsylvania’s Office of Developmental Programs is committed to Employment First and committed to eliminating barriers, where possible, for individuals to find and maintain competitive integrated employment.
If you or someone you know needs more information about how to access employment services, contact your Supports Coordinator or find information on the Department of Human Services’ website.
References
1. Disability: Part of the Equity Equation, Office of Disability Employment Policy, https://www.dol.gov/agencies/odep/initiatives/ndeam
2. August of 2022, Labor Force Participation Rate for People ages 16 and older; People with Disabilities = 22.5%; People without Disabilities = 68%. Source = Current Population Survey, Bureau of Labor Statistics, https://www.bls.gov/cps/home.htm, Accessed October 26, 2022.
3. Work Matters for Health, Issue Brief 4: Work and Health, Robert Wood Johnson Foundation, Commission to Build a Healthier America, http://www.commissiononhealth.org/PDF/0e8ca13d-6fb8-451d-bac8-7d15343aacff/Issue%20Brief%204%20Dec%2008%20-%20Work%20and%20Health.pdf, 2008, Accessed October 27, 2022.
Biography
Laura Cipriani has worked for the Office of Developmental Programs for 7 years. Laura was a Program Representative for the Bureau of Supports for Autism and Special Populations before joining ODP’s Policy Division in 2019, where she serves as a Policy Supervisor. Prior to working at ODP, Laura was the Director of the Child Residential and Mental Health Licensing Division for the Bureau of Human Services Licensing. She has more than 20 years of experience in human services and is proud to serve in Pennsylvania, an “Employment First” state for people with disabilities.
Contact Information
Laura Cipriani
Pennsylvania Office of Developmental Programs
Policy Supervisor
lcipriani@pa.govDavis-Moulfair | 28-38
Volume 11 ► Issue 3 ► November 2022
The Importance of Medical Assistance for Workers with Disabilities
Ashley Davis-Moulfair
Introduction
Working and maintaining essential medical benefits and supportive services can be a delicate balancing act for individuals with disabilities. Medical Assistance is often not only an essential layer of medical coverage, but the gateway criteria for individuals to receive third party services that foster the skills, confidence, and independence necessary to garner success in the workforce. Unfortunately, that same success has the potential to threaten their eligibility for Medical Assistance and the crucial supportive services they need due to strict income requirements.
Background
The Medical Assistance for Workers with Disabilities (MAWD) program in Pennsylvania is a unique program that works to keep individuals with disabilities covered while allowing them to further themselves in their employment journey and build financial stability. Supporting people with disabilities while they gain a strong foothold in the working world not only fosters independence and self-sufficiency for recipients of MAWD, but also contributes to an inclusive workforce and a decreased need for long-term public assistance.
The MAWD program was established in Pennsylvania through the options provided in the federal Ticket to Work and Work Incentives Improvement Act (TWWIIA) of 1999 (Public Law 106-170). Pennsylvania subsequently passed Act 77 of 2001, which provided the state share of funds necessary to implement MAWD.
What is MAWD?
The MAWD program boasts higher income thresholds than many other Medical Assistance categories in Pennsylvania and pairs this flexibility with a modest monthly premium based on the recipient’s net income. To qualify for MAWD, an individual must be between the ages of 16 and 65, have a disability that adheres to Social Security Administration’s (SSA) requirements or the department’s disability review criteria, be employed and receiving compensation with countable monthly income (after allowable deductions) equal to or less than 250% of the Federal Poverty Income Guidelines (FPIG), and have countable household resources totaling no more than $10,000. MAWD recipients pay a monthly premium calculated at 5% of their countable income.
Figure 1: MAWD Income and Resources Limits by Household Size
Note: The figures below are actual income limits based on either a household size of one (only the MAWD recipient) or a household size of two (a MAWD recipient and their spouse).
|
Household Size |
2022 250% FPIG Monthly Income Limit |
2022 250% FPIG Annual Income Limit |
Resource Limit |
|
1 |
$2,832.00 |
$33,975.00 |
$10,000.00 (None, if they received Workers with Job Success) |
|
2 |
$3,815.00 |
$45,775.00 |
$10,000.00 (None, if they received Workers with Job Success) |
The MAWD umbrella also encompasses two sub-category groups with the intent to extend coverage for workers as they progress. The first is the Workers with a Medically Improved Disability category, which serves MAWD recipients whose disability has improved to the point where they no longer qualify under SSA or the department disability review criteria. Most of the eligibility criteria for this category mirrors that of MAWD, but with the key distinction of requiring that the individual work at least 40 hours per month earning at least minimum wage.
Pennsylvania further expanded MAWD in December 2021 by creating the new Workers with Job Success (WJS) category with the passage of Act 2021-69 of July 1, 2021 (P.L. 374). WJS is unique in its flexibility with income eligibility, allowing MAWD recipients to advance professionally while maintaining access to Medical Assistance coverage and the crucial services facilitated by their eligibility. In order to qualify, an individual must have at least 12 previous consecutive months of enrollment in a MAWD category and countable income that is over 250% of the FPIG and less than or equal to 600% of the FPIG. Although individuals must also adhere to the $10,000 resource limit required of the other MAWD categories, they are able to accumulate resources beyond that threshold in the MAWD program once enrolled in WJS.
Figure 2: MAWD WJS Income and Resource Limits by Household Size
Note: The figures below are actual income limits based on either a household size of one (only the MAWD WJS recipient) or a household size of two (a MAWD WJS recipient and their spouse).
|
Household Size |
2022 600% FPIG Monthly Income Limit |
2022 600% FPIG Annual Income Limit |
Resource Limit |
|
1 |
$6,795.00 |
$81,540.00 |
$10,000.00 at initial eligibility, then disregarded |
|
2 |
$9,155.00 |
$109,860.00 |
$10,000.00 at initial eligibility, then disregarded |
The premium structure for recipients of WJS is also unique in contrast to its counterpart categories. Individuals enrolled in this category pay a monthly premium that is 7.5% of their countable monthly income if that income is between 250% and 450% FPIG. However, if the individual’s countable income is above 450% FPIG and their annual adjusted gross income reported on their federal 1040 tax form is at or more than $75,000 compounded with Social Security cost-of-living adjustments since 2000 ($125,944.84 in 2022), the individual is responsible to pay a full cost monthly premium as determined by the department (currently $948).
The Impact of MAWD
The MAWD program has a domino effect on its recipients and the overarching support they receive, and Medical Assistance eligibility has distinctly personal implications for individuals with disabilities. We spoke with two working adults with disabilities and their families to explore how MAWD influences their access to services and the ripple effects that drive their personal success.
Amelia
Amelia is 45 years old and resides with her mother, Lillian. Amelia was diagnosed with pervasive developmental disorder and autism spectrum disorder (ASD), and she has low support needs that allow her to be fairly independent in her day-to-day responsibilities. In addition to her Medical Assistance benefits, Amelia also receives supportive services from Pennsylvania’s Adult Community Autism Program (ACAP), a managed care program available across four counties, which has provided her with key life skills as well as transportation to and from work. Of utmost importance is the face-to-face time furnished by a Community Supports Provider (CSP) who offers individualized hands-on interaction that helps Amelia practice skills such as cooking, shopping, and scheduling doctor’s appointments. Working with her CSP has also built Amelia’s confidence and independence to the point where she was able to live independently in her own apartment for five years. The services afforded by ACAP and the CSP have been key in improving Amelia’s communication skills and in keeping her active outside the home, which is something Lillian proclaims is especially challenging.
Amelia has been working since she graduated from high school and spent 25 years of her employment tenure at a local grocery store performing various duties including bagging groceries, stocking shelves, and collecting shopping carts. When Amelia’s father passed away in 2017, she was awarded a Social Security survivor’s benefit on top of her Social Security disability (SSD) payment. Combined with her wages from her grocery store employment, Amelia was suddenly over the income limit for her current Medical Assistance program. At that point, she made the seamless transition into the MAWD program and saw no changes to her coverage or eligibility for supportive services beyond the addition of a monthly premium.
Amelia’s mother, Lillian, said that if not for MAWD, Amelia may have lost her Medical Assistance once she received her survivor’s benefit in 2017. Lillian asserts that if that had happened, “She would not have her support with the ACAP program, which to me means that I would have had to figure out what to do for her for support. Up until we found the ACAP program, we really didn’t have support for her. My husband and I figured out how to help her on our own.”
During the pandemic, Amelia had to step back from her work at the store in order to safeguard her health. After a while, she officially ended her employment with the grocery store and became self-employed from home. Amelia now performs household duties such as cleaning, helping her mother and neighbors with the trash, and other miscellaneous tasks for several hours a month. This change, although unplanned, has proven a positive change for Amelia as she has noticed a reduction in physical and emotional stress, more flexibility, and an improvement to her diabetes management. She still meets the requirements for MAWD and has experienced no alterations in the medical care or supportive services that assist her.
Steven
Steven is a 49-year-old man with ASD who lives independently with low support needs. Although he exerts significant autonomy in traveling to events by bus, carrying his own cell phone, and managing his schedule, Steven still requires the assistance provided by ACAP. His CSP helps him continue to build social and basic life skills, offers general advice, and provides companionship. ACAP also provides Steven with a behavioral health specialist and his CSP provides reliable transportation to and from Steven’s counseling sessions as well as his job. Steven’s mother, Carol, who says she is well into her 70s, states that the services afforded by ACAP help relieve her mental burdens about what will happen to her son when she is no longer around. Carol also asserts that ACAP also advocates for the individuals they serve by working to educate doctors and other public servants on how to treat and interact with people with disabilities.
Steven joined the workforce in his late 20s and is currently employed part-time at a hotel doing general housekeeping duties within the common areas. He has been working at the hotel two to three days per week for over seven years, and he has never been late or taken a sick day. Steven enjoys the routine and social interaction of his employment, although previous stints working full-time proved to be overwhelming and caused him anxiety.
In reflecting on the benefits of MAWD and the necessity of Medical Assistance/Medicaid for her son Steven, Carol said, “It’s good to have MAWD, because if he started working more hours then he could be in MAWD and get Medicaid. And that is a very good thing.”
Steven became eligible for the MAWD program by virtue of his combined wages and Social Security income. Since becoming a MAWD recipient, his Medical Assistance coverage has remained consistent and has allowed him to access the full extent of ACAP services he needs to remain successful in his personal and professional life.
More Than Just Medical Assistance
Supporting individuals with disabilities is a holistic endeavor, and the true impact of the MAWD program goes far beyond that of medical coverage. In fact, Medical Assistance acts as a doorway to a host of varied third-party agencies and services that provide wraparound supports to build up individuals. Additionally, a Medical Assistance program that is directly geared toward keeping recipients gainfully employed and even promotes professional advancement while maintaining the same level of medical coverage, fosters growth and independence without fear of losing the very supports that help individuals succeed.
The Pennsylvania Department of Human Services (DHS) holds the MAWD program in high regard as a crucial safety net for individuals with disabilities. Although the program currently covers approximately 29,430 individuals, it is believed that there is a significant population who are not aware of the program and its flexibilities. The MAWD program should be shared amongst the community of entities who serve individuals with disabilities to help ensure that people are not stunted in their desire to work for fear of losing their benefits. Individuals, their families, our communities, and our workforce will be better served if the goals and ambitions of those with disabilities are fully supported.
Information about the MAWD program can be found on the DHS website (www.dhs.pa.gov/MAWD). Individuals can apply for Medical Assistance and other public assistance programs via Pennsylvania’s online application portal, COMPASS, (www.compass.state.pa.us) or at any County Assistance Office (www.dhs.pa.gov/Services/Assistance/Pages/CAO-Contact.aspx).
References
1. Medical Assistance Eligibility Handbook. services.dpw.state.pa.us. Accessed October 4, 2022. http://services.dpw.state.pa.us/oimpolicymanuals/ma/index.htm#t=Title_Page.htm
2. Department of Human Services, Office of Income Maintenance. Introduction of a New Medical Assistance for Workers with Disabilities (MAWD) Eligibility Group - Workers with Job Success (WJS). PA Department of Human Services. Published July 1, 2022. Accessed October 4, 2022. http://services.dpw.state.pa.us/oimpolicymanuals/ma/Introduction_of_a_New_MAWD_Eligibility_Group_-_Workers_with_Job_Success_(WJS).pdf
Biography
Ashley Davis-Moulfair has worked for the Office of Income Maintenance (OIM) as Communications Coordinator for over four years. Prior to this position, she spent two years as an Income Maintenance Caseworker with OIM processing public assistance benefits. She received a Bachelor of Science in (English) Education from Millersville University.
Contact Information
Ashley Davis-Moulfair
Communications Coordinator
PA Department of Human Services, Office of Income Maintenance
adavismoul@pa.gov
Goddard | 39-48
Volume 11 ► Issue 3 ► November 2022
Available Employment Supports for Individuals who are Deaf, Hard of Hearing, or DeafBlind with Additional Disabilities
Russell L. Goddard, Jr., MRC, CRC
According to the National Deaf Center on Postsecondary Outcomes, only 53% of deaf individuals in 2017 participated in the labor force, compared to almost 76% of those without hearing loss.1 However, this statistic takes into consideration the entirety of the deaf population, including race, gender, and the presence of other disabilities. If only considering deafdisabled people, defined in the report as those who are deaf and with at least one other disability, such as cognitive disabilities, autism, mental illness, and physical disabilities, that statistic drops to only 39%.1 Within the category of deafdisabled individuals, those who are deafblind report the highest employment rates, while those requiring assistance with personal care or independent living report the lowest employment rates. In addition, more deafdisabled people (33.4%) work part-time than those who are deaf without additional disabilities (23.2%). Depending on the type of additional disabilities a deafdisabled person may have, there is a pay disparity of as much as $10,000 between those who are deafdisabled and those who are deaf with no additional disabilities. In addition to having the greatest disparity in income, those who are deafdisabled with independent living difficulties report an employment rate of only 19.9%, compared to 71.9% for deaf individuals with no additional disabilities.
One of the few available resources to combat the issue of low employment rates among the deaf population is through the state-federal vocational rehabilitation (VR) program. This program has existed in one form or another for over a hundred years. The US government created the vocational rehabilitation system in 1918 through the Smith-Sears Veterans Rehabilitation Act to provide vocational rehabilitation services for veterans who became disabled during World War I. Two years later, the Smith-Fess Act was passed to bring vocational rehabilitation services to the civilian population. The 1920 Smith-Fess Act initially provided vocational rehabilitation services only to those with physical disabilities, and only provided vocational counseling and guidance, training, occupational adjustment, prosthetics, and placement services. Over the next several decades, a series of amendments and new legislation expanded the scope of VR services to include those with cognitive disabilities, developmental disabilities, sensory disabilities, and those with drug and alcohol addiction. In addition, the menu of services expanded to include physical and mental restoration services, supported employment services, and rehabilitation technology and engineering. The VR system is currently operating under the 1973 Rehabilitation Act as amended by the 2014 Workforce Innovation and Opportunity Act (WIOA), which added additional emphasis on high school students with disabilities to obtain critical pre-employment transition services. Other federal legislation, including the Americans with Disabilities Act (ADA), the Education for All Handicapped Children Act, and the Social Security Act, all supported the concept of employment for individuals with disabilities through their own regulations.
Highly individualized services for the deaf, hard of hearing, and deafblind populations is a relatively new phenomenon. Between 1964 and 1965, there was a worldwide epidemic of rubella, also known as German measles. Babies who were born with German measles tended to be born deaf. As this population of deaf individuals grew up and were starting to access vocational rehabilitation services, VR agencies across the nation needed guidance on providing services to this population to address their vocational needs. To address potential shortcomings in providing VR services for this population, the Model State Plan for Vocational Rehabilitation Services for Deaf People (MSP) was first developed in 1973, with several revisions and expansions to the MSP happening in the years since. The MSP provides guidance on VR services that were thought to be effective with this population, including sign language interpreters, technology such as TTYs, and VR agency staff and personnel who are charged with implementing portions of the MSP in their agencies. The latest iteration of the MSP was published earlier this year, and this author is one of the contributors for this document.2
While a formal set of guidelines for serving the deaf, hard of hearing, and deafblind populations were established almost 50 years ago, it wasn’t until the last 25 years when additional attention was paid toward deafdisabled individuals who are receiving Office of Vocational Rehabilitation (OVR) services. In 1999, a publication by the Institute on Rehabilitation Issues, an institute funded by the US Department of Education’s Rehabilitation Services Administration (RSA), “Serving Individuals Who Are Low-Functioning Deaf,” provided additional technical guidance on serving those who are deafdisabled. In this report, several characteristics that identify individuals who are low-functioning deaf include inadequate communication skills, deficiencies in behavioral, emotional, and social adjustment, deficiencies in independent living skills, and deficiencies in educational and transitional skills.3 Combined with functional limitations in communication, other additional disabilities such as autism, mental health issues, intellectual disabilities, and other developmental disabilities impose additional unique challenges that require a highly individualized and personalized set of VR services designed to help the individual achieve competitive integrated employment.
Within the Commonwealth of Pennsylvania, the Office of Vocational Rehabilitation (OVR), an office located within the Pennsylvania Department of Labor and Industry (L&I), holds the sole responsibility for administering the state-federal VR program. The Office of Vocational Rehabilitation receives federal matching funds through RSA to administer the statewide VR program for Pennsylvanians with disabilities. In addition, OVR develops partnerships with other agencies and organizations, such as the PA Office of Developmental Programs (ODP), the PA Office of Mental Health and Substance Abuse Services (OMHSAS), and the Bureau of Juvenile Justice Services (BJJS) to enhance service delivery to those who need additional services beyond what OVR may provide in-house.
Vocational Rehabilitation services are available to those with any eligible person with a disability or disabilities. To receive VR services, a person must have an impairment that imposes functional limitations on their ability to obtain, retain, or advance in competitive integrated employment (CIE), must require VR services to overcome such functional limitations, and must benefit from VR services. Individuals with disabilities who apply for VR services are presumed to benefit in terms of an employment outcome unless there is clear and convincing evidence that the individual cannot benefit from VR services. Those who receive certain SSA benefits due to their disabilities are presumed to be eligible for VR services unless there is clear and convincing evidence that they cannot benefit from VR services.
Once an individual is made eligible for OVR services, the VR counselor and the customer start discussing the customer’s Individualized Plan for Employment (IPE). The OVR may provide a wide range of individualized services that may include college training, short-term training, job coaching, hearing aids, sign language interpreters, tools and clothing for employees, and counseling and guidance from the VR counselor, to name a few possible services. To assist with the development of the IPE, the VR counselor may obtain additional information from a service coordinator, educational staff, and/or the customer’s family or legal guardians, as well as any treating medical professionals and personnel within the criminal justice system such as a parole officer or probation officer, to name a few. The purpose of obtaining additional information is to help the VR counselor paint a more complete picture of the customer, including their abilities and disabilities, their available resources, transportation options, their interests, options for services and service providers, and their legal status with the criminal justice system. Once all the necessary information is gathered and analyzed by the VR counselor, an IPE is then developed and agreed upon between the VR staff and the customer. The VR counselor then follows along with the customer in ensuring the services that are delivered to the customer assist them with achieving, retaining, or advancing in their regular jobs. In some cases, waiver funding may be used for extended supported employment services after OVR closes their case after 90 days on the job.
The Office of Vocational Rehabilitation relies on its relationships and connections with the various non-profit organizations, Commonwealth agencies, and businesses that provide medical services to deliver individualized services for customers to assist them with achieving competitive integrated employment. As an example of the type of cooperation needed to assist individuals who are deafdisabled, below is an actual case story from M. Cook, MA (email communication, September 2022) that illustrates how OVR works with other agencies to assist this customer with complex medical needs with achieving competitive integrated employment.
John is a 22-year-old young man with an intellectual disability, profound bilateral sensorineural hearing loss, and visual challenge to both eyes with significantly decreased vision mostly to the left eye due to CHARGE syndrome, a genetic disorder which can affect multiple organs in the body. Several years ago, while a student at the Pennsylvania School for the Deaf (PSD), he applied for OVR, and he wanted to work in a competitive work environment upon graduation. Through vocational counseling and guidance, he and his VR counselor narrowed his vocational choices to hospital patient transporter, stocking, and bakery. It was clear during the initial interview and IPE development that John is hard worker, determined, motivated, curious, and has good endurance. He was a student at PSD from September 2005 until December 2020, following an adapted academic program, but stayed at PSD as he was on the ACT 22 program until end of August 2022. He completed paid work experience (PWE) in the spring of 2022 with job coaching support at Weis Markets in Macungie, completing his tasks in bakery and stocking/re-shop. He also received orientation and mobility (O&M) services provided by the school district.
John has applied to this location as the general manager expressed interest in hiring him as a part-time employee. The general manager, upon acknowledging John’s commitment to Weis through years of volunteer service at Weis through services provided by the Lehigh Valley Center for Independent Living’s Living Independently for Everyone (LVCIL LIFE) program, has offered him the potential opportunity to transition from being a Weis volunteer to a Weis paid part-time employee. His work tasks are bakery and front end-re-stop. He has a Licensed Registered Nurse (LRN) that accompanies him in the community to support him with any medical needs when he is working.
At PSD, in addition to an American Sign Language (ASL) interpreter, he was encouraged to use Proloquo2Go on his iPhone and iPad, but he indicated his preference to use an ASL interpreter. In discussing employment, his parents were notified that OVR will not pay for interpreters for his career life. He was referred for an assistive technology (AT) evaluation to see if he could have accommodations for his work. As a result of the evaluation, OVR purchased an iPad and Prolongo2 software so he can be as independent as possible in the community. The plan is to trial video remote interpreting services (VRI) to allow him to connect with an interpreter while in the community, thus increasing his independence. Funds from the Consolidated Waiver will fund the VRI service.
John completed two community-based work assessments (CBWA) on the job to identify work environment issues and concerns as well as identify supports needed moving from PWE to part time employment working twenty hours per week. The Office of Vocational Rehabilitation has funded phase 1 and 2 of supported employment services for him to begin his employment at Weis. He receives services from ODP and has a consolidated waiver. Pennsylvania’s Office of Developmental Programs is working to add interpreter services to their list of services provided, however, this is expected to take some time. In the interim, OVR will fund an interpreter while John is working with a job coach. The OVR will transition the supported employment services and ASL interpreter services to waiver funding and move case to a successful closure once customer is stable for 90 days at Weis and when either waiver funding is in place to provide an interpreter, or it is determined that the trial of VRI is successful and meets the customer’s communication needs. Additionally, John will be evaluated for the need for additional O&M services should that be required on the job. John is very excited to begin his part-time employment at Weis.
Thanks to the services available through OVR and their many collaborative partners, OVR customers like John can access specialized employment supports and have a chance to experience competitive integrated employment in a community setting. More importantly, the services provided to customers like John promotes independent living, self-determination, and greater participation in their local communities.
*=the term deaf is used in an all-inclusive manner, to include people who may identify as deaf, deafblind, deafdisabled, hard of hearing, late-deafened, and hearing impaired.
References
1. Garberoglio, C.L., Palmer, J.L., Cawthon, S., & Sales, A. Deaf People and Employment in the United States: 2019. Washington, DC; U.S. Department of Education, Office of Special Education Programs, National Deaf Center on Postsecondary Outcomes; 2019. https://www.Deaf People and Employment in the United States: 2019 (nationaldeafcenter.org)
2. Deaf Professionals Network. CSAVR Model State Plan for Vocational Rehabilitation Services for Deaf People. Council of State Administrators of Vocational Rehabilitation (CSAVR); Washington, DC; 2022. https://www.MSP for Deaf Services | csavr, Accessed October 20, 2022
3. Dew, D. W., Lucas, L. H., & Tomlinson, P. A. Serving Individuals Who Are Low-Functioning Deaf. 25th Institute on Rehabilitation Issues, The George Washington University, Regional Rehabilitation Continuing Education Program; 1999. Washington, DC.
Biography
Russell L. Goddard, Jr. works for the PA Office of Vocational Rehabilitation as the Statewide Coordinator of Deaf, Hard of Hearing, and Deafblind Services. In his position, Russ provides technical assistance to OVR field staff and central office staff with issues related to the provision of services for deaf, hard of hearing, and DeafBlind OVR customers. Russ has a total of 23 years of experience in vocational rehabilitation, first as a rehabilitation counselor for the deaf and hard of hearing in the state of Ohio, then continuing in the same capacity for PA OVR before assuming the role of his current position. Russ himself has a hearing loss, bringing into this position a wealth of personal and professional knowledge about adult services, and educational and transition services for high school students with hearing loss.
Contact Information
Russell L. Goddard, Jr., MRC, CRC
Pennsylvania Office of Vocational Rehabilitation
Statewide Coordinator of Deaf, Hard of Hearing, and DeafBlind Services
rgoddard@pa.govLoss | 49-59
Volume 11 ► Issue 3 ► November 2022
Employment Services Designed for Individuals with Serious Mental Illness (SMI)
Randall Loss, M.A., C.R.C.
Abstract
The Individual Placement and Support (IPS) supported employment model has considerable research conducted to show it’s an evidenced based practice (EBP) for individuals with serious mental illness (SMI). Additionally, this supported employment service is designed for use with individuals ages 16 and older. This article describes IPS as an EBP including focus on data and programs such as Assertive Community Treatment (ACT), First Episode Psychosis (FEP) and Clubhouse that use this tool as part of a larger continuum of services. This description draws from published and nonpublished material about definitions, impact, and the best use of IPS service. While IPS is an EBP, implementation requires collaboration between state vocational rehabilitation and mental health offices in collaboration with county mental health offices to fund and support.
Are there opportunities within the mental health system for people to truly improve their lives? Are there a range of affordable, normal housing situations from which people can choose a place to live? Is there work available? A person who just recently went back to work after many years of hospitalization said to me, "What's all this talk about empowerment? I can tell you the definition of empowerment: "It's a decent paycheck at the end of the week". 1
The previous paragraph is a quote from Dr. Pat Deegan delivered at a conference in 1996. Despite its age, it’s a powerful statement regarding empowerment as seen through the eyes of an individual with serious mental illness (SMI). Also, it is an essential starting point to discuss the role employment has for those with SMI. Employment is a significant wellness component and a clear indicator of an individual being on a successful mental health recovery path.
Serious mental illness is defined as a mental, behavioral, or emotional disorder resulting in serious functional impairment, which substantially interferes with or limits one or more major life activities. 2 Further, there are a few more definitions that are needed before continuing the discussion on the impact of employment in the lives of those living with an SMI. “Wellness is a broad concept. Think of wellness as being healthy in many dimensions of our lives.” 3 Recovery is defined “as a process of change through which individuals improve their health and wellness, live self-directed lives, and strive to reach their full potential.” 4
According to the United Nations Universal Declaration of Human Rights of 1948, Article 23, “Everyone has the right to work, to free choice of employment, to just and favorable conditions of work, and protection against unemployment.” 5 Even with the right to work in place, a job seeker with a disability is not guaranteed they will be able obtain employment unless supports are provided that address disability-related challenges in finding and keeping work. Data suggests that people with severe and persistent mental illness have low employment rates ranging from 13–55%. 6,7
Holding a job is the central hub from which many other areas of functioning emanate. For this reason, employment is considered one of the most important factors in promoting recovery and social inclusion. It not only provides financial independence but also structure and purpose, opportunities for socializing and developing new relationships, a sense of identity, self-worth, and meaning in life.7 The onset of mental health conditions is associated with more than double the risk of leaving employment compared to other health conditions or impairments. Evidence suggests that unemployment is a risk factor for the development or exacerbation of mental health conditions and misuse of substances. Unemployment also results in decreased social networks and loss of structure, purpose, and identity. 7
Having a job is important to the mental well-being of any individual but, as identified above, even more so for persons with SMI. Many individuals with SMI do successfully gain employment through applying directly to employers or using public resources like the PA CareerLink or JobNET. On the other hand, there are times when supports specifically designed to address the nature of SMI are needed to help an individual seek, obtain, and maintain employment. When multiple SMI-related issues need to be simultaneously addressed for a job seeker, there are a few programs that incorporate supported employment alongside other mental health interventions. The reader may now ask, what is an available tool to assist those with SMI in gaining community-based employment? Additionally, what mental health service programs use these tools to assist an individual towards an effective recovery path? The remainder of this article identifies the most successful evidence-based practice (EBP) employment service for individuals with SMI and which mental health programs could include this service as a resource.
It is the experience of this author that the primary tool to assist individuals with SMI to gain employment is supported employment (SE). Supported employment is a universal service designed to assist those with disabilities to successfully enter the workforce. Research has shown the SE version to work most effectively for those with SMI is the Individual Placement and Support (IPS) model. Individual placement and support is an EBP and is the heart of the Substance Abuse and Mental Health Services Administration (SAMHSA) supported employment toolkit for assisting those with SMI in pursing employment. Individual placement and support embodies the following principles: (1) competitive employment, (2) eligibility based on client choice, (3) integration of rehabilitation and mental health services, (4) attention to client preferences, (5) personalized benefits counseling, (6) rapid job search, (7) systematic job development and (8) time unlimited and individualized support. 6 Although relatively more effective than traditional supported employment services, IPS employment rates still show that it’s not effective for everyone. What research does indicate is that IPS is moderately more effective for those with SMIs, schizophrenia spectrum disorders, and a low symptom severity.8
The competitive employment rate outcomes of gainful community employment for IPS are on average 58–60% successful versus 23–24% of the traditional train-and-place supported employment . In addition, Loveland et al. point out that almost three-quarters of people using IPS require additional services such as cognitive, psychosocial skills, and illness management training. 6
The best application of the IPS SE service as a stand-alone service or in conjunction with a larger program is when it follows the IPS Fidelity Scale. This tool is a measurement of how closely the service provider is following the EBP of IPS. The closer the provider follows the IPS program fidelity, the better the employment outcomes for the job seekers with SMI who are receiving SE services. This tool can easily be found online and at no cost for any employment service provider interested in using this resource to enhance its employment programming.
One mental health services program that assists individuals with SMI by using IPS SE, along with other mental health treatment services, is the Assertive Community Treatment (ACT) team. ACT teams in Pennsylvania must include the following: a psychiatrist, nurse, peer specialist, substance abuse specialist, vocational specialist along with MH clinical staff and many staff require Masters’ level degrees. Assertive Community Treatment services are designed for individuals with SMI who have had at least two psychiatric hospitalizations in the past 12 months and who are at least 18 years of age. There are currently 43 ACT programs in 26 counties across Pennsylvania. Assertive Community Treatment is a person-centered approach to care for adults that aims to lessen or eliminate symptoms of mental illness; minimize or prevent recurrent episodes of illness; enhance an individual’s ability to live independently within his or her own community; and lessen the family’s burden of providing care. What follows are widely accepted, essential-features of the model to reduce symptoms of mental illness: a multi-disciplinary ACT team with small case-loads (typically staff: patient ratios between 1:10 and 1:12) providing high intensity integrated services and a team approach to sharing responsibility for the whole caseload. The ACT team is assertive in its attempts to engage patients for whom the team has continuous responsibility 24 hours a day, 7 days a week.9 The ACT teams which should have more successful employment outcomes are the ones that have the employment specialist function distinctly from the mental health treatment team. Basically, the employment specialist does employment supports only for the ACT client.
Another program that assists individuals with SMI in a comparable fashion to the ACT program is the First Episode Psychosis (FEP) program. There are currently nine FEP sites in Pennsylvania with five only serving one to four counties each and four programs serving all of Pennsylvania. The premise of the FEP program is based on coordinated specialty care (CSC), which is a recovery-oriented treatment program for people with first episode psychosis (FEP). CSC promotes shared decision making and uses a team of specialists who work with the client to create a personal treatment plan. The specialists offer psychotherapy, medication management geared to individuals with FEP, family education and support, case management, and work or education support, depending on the individual’s needs and preferences.10 Approximately 100,000 adolescents and young adults in the United States experience FEP each year. With a peak onset occurring between 15-25 years of age, psychotic disorders such as schizophrenia can derail a young person’s social, academic, and vocational development and initiate a trajectory of accumulating disability.10 Ideally, the FEP employment specialist that uses and adheres to the IPS Fidelity Scale can increase successful employment outcomes for program participants.
Clubhouse is another program that can potentially use IPS supported employment. The big difference when compared to ACT and FEP is the approach staff take in helping individuals with SMI, known as Clubhouse members, realize their employment potential. The daily activity of a Clubhouse is organized around a structured system known as the work-ordered day (WOD). Members and staff work side by side as colleagues to perform the work that is important to their community. Instead of traditional talk therapy, members and staff share responsibility for running every aspect of the Clubhouse. By sharing responsibility for critical work, members and staff build relationships focused on each other’s strengths and gifts, rather than weaknesses and liabilities.11 One theme that emerged throughout a research study’s interview sessions of Clubhouse members was the value of having ‘‘things to do.’’ Although participants were either regularly working for WOD or at their own community-based jobs at the time of the study, their stories revealed that they had virtually no involvement in activities that they felt were ‘‘meaningful,’’ ‘‘constructive,’’ or ‘‘productive’’ before they had come to the Clubhouse. Work ordered day can also mean preparation for a job to live independently. L., a member from Ohio, compared the Clubhouse to school. Work-ordered day, then, may be classroom. While WOD chores are needed to run the clubhouse, they also serve to help members learn a wealth of job skills that can serve as initial steps toward more complex tasks. This study illustrated peer-to-peer collaboration, side by side during the WOD and personal peer relationships—how they emerge and develop as secondary to WOD participation—revealing various self-help effects including feelings of ‘‘we are not alone’’ and what has been described as the ‘‘helper therapy’’ whereby people feel they are being helped themselves by their efforts to help others.11 It is important to note that once a member is ready to seek competitive community-based employment, a staff whose focus is on employment support can potentially use the IPS supported employment model to assist that member obtain a job using the WOD foundation from which that member learned while at the Clubhouse.
So, what does the information shared above mean for employment supports to those with SMI? The fact that IPS supported employment is seen as the center of the EBP SAMHSA toolkit and the employment tool for most mental health programs such as ACT, FEP and Clubhouse, speaks volumes to its use as the best method of helping those with SMI get and keep employment. The biggest challenge IPS has is that of funding which will likely be an ongoing barrier into the foreseeable future. Many states that have implemented IPS statewide typically use braided funding between the state vocational rehabilitation agency and the state office of mental health. These state offices of mental health have used various funding ranging from grants, rehabilitation options of Medicaid waivers, Mental Health Block Grant funds, among others.12 Solid IPS supported employment funding requires many partners collaborating for the benefit of those with SMI. The benefit is individuals with SMI having a job that offers a decent paycheck is not only employment but empowerment and independence.
References
1.
Labor Day, Work, and Recovery from Psychosis. ISPS.
https://isps-us.org/blog/reflections-on-labor-day-and-the-role-of-work-in-recovery-from-psychosis/.
Accessed
September 28, 2022.
2.
Serious Mental Illness Definition. Bing. https://www.bing.com/search?q=serious%2Bmental%2Billness%2Bdefinition&form=ANNNB1&refig=34
a6c355e85f438ea9be843e2b77726c&sp=2&qs=AS&pq=serious%2Bmental
%2Bill&sk=PRES1LS1&sc=10-18&cvid=34a6c355e85f438ea9be843e2b77726c.
Accessed September 28, 2022.
3.
Creating A Healthier Life – A Step by Step Guide to Wellness.
https://store.samhsa.gov/sites/default/files/d7/priv/sma16-4958.pdf.
Accessed September 28, 2022.
4.
Recovery and Recovery Support.
https://www.samhsa.gov/find-help/recovery#overview.
Accessed September 28, 2022.
5.
Universal Declaration of Human Rights. United Nations.
https://www.un.org/en/about-us/universal-declaration-of-human-rights.
Accessed September 28, 2022.
6. Dewa, C, Loong, D, Trojanowski, L & Bonato, S. (2017). The Effectiveness of Augmented Versus Standard Individual Placement and Support Programs in Terms of Employment: A Systematic Literature Review. Journal of Mental Health. 27. 1-10. doi:10.1080/09638237.2017.1322180.
7. Rinaldi, M, Killackey, E, Smith, J, Shepherd, G, Singh, S & Craig, T. (2010). First Episode Psychosis and Employment: A Review. International Review of Psychiatry (Abingdon, England). 22. 148-62. doi:10.3109/09540261003661825.
8. de Winter, L, Couwenbergh, C, van Weeghel, J, Sanches, S, Michon, H & Bond, G. (2022). Who Benefits from Individual Placement and Support? A Meta-analysis. Epidemiology and Psychiatric Sciences. 31. 1-24. doi:10.1017/S2045796022000300.
9. Fiander, M, Burns, Mchugo, G & Drake, R. (2003). Assertive Community Treatment Across the Atlantic: Comparison of Model Fidelity in the UK and USA. The British Journal of Psychiatry: the Journal of Mental Science. 182. 248-54. https://www. Assertive community treatment across the Atlantic: Comparison of model fidelity in the UK and USA (researchgate.net).
10.
What is Coordinated Specialty Care (CSC)? National Institute of Mental Health.
https://www.nimh.nih.gov/health/topics/schizophrenia/raise/what-is-coordinated-specialty-care-csc#:~:text=Coordinated%20specialty%20care%20%28CSC%29%20is%20a%20recovery-oriented%20treatment,the%20client%20to%20create%20a%20personal%20treatment%20plan. Accessed
September 28, 2022.
11. Tanaka, K, & Davidson, L. (2014). Meanings Associated with the Core Component of Clubhouse Life: The Work-Ordered Day. The Psychiatric Quarterly. 86. doi:10.1007/s11126-014-9330-6.
12.
IPS Supported Employment Funding in the United States.
https://ipsworks.org/wp-content/uploads/2018/03/funding_graphic.pdf.
Accessed September
28, 2022.
Biography
Lisa Morgan, founder and co-chair of the Autism and Suicide committee of the American Association of Suicidology, is an autistic self-advocate in crisis supports for autistic people. Lisa has a master’s degree in Special Education and is a certified autism specialist. Owner of Lisa Morgan Consulting LLC, Lisa helps autistic people utilize their autistic strengths to have a better quality of life. Lisa’s books, articles, and resources can be found at http://www.autismcrisissupport.com.
Contact Information
Randall E. Loss’ vocational rehabilitation (VR) career spans 30 years, starting in 1991 as a wilderness camp counselor for adjudicated youth. He next worked with students in an alternative schooling program. His role in both settings was to help these students learn socially appropriate and pre-vocational skills in preparation for community and public-school reintegration. He then transitioned to assisting individuals with intellectual disabilities, first in a sheltered workshop, then as a supports coordinator and finally as a job coach until 1999. He subsequently became a field operations manager for the Experience Works older-adult employment training program with a staff of seven program participants. In 2002 he started at OVR in the contracts and grants division as a specialist overseeing letters of understanding and grant management. He then moved into policy and program development until he left OVR in 2017. While in policy he supported a variety of disability populations and program areas including: Supported Employment, Vehicle/Home Mods, Assistive Technology, Farm and Ranch, ID, MH, TBI and Veterans. In 2008 he became focused on working with criminal justice system involved individuals and was the lead policy staff on several projects to improve employment outcomes for this population. In 2017, he led Memorandum of Understanding (MOU) efforts with the Pennsylvania Bureau of Juvenile Justice Services (BJJS) to connect students in the juvenile justice system with positive employment outcomes. In 2018 he left OVR to provide technical assistance to VR agencies nationwide as a Senior Technical Advisor with the Youth Technical Assistance Center (Y-TAC). He was a subject matter expert on Mental Health peer mentoring and guiding VR agencies’ work with youth and students in the juvenile justice system, and/or were in foster care, were homeless or were out of school. Since late 2018 he returned to Commonwealth service as the policy employment lead for the PA Office of Mental Health and Substance Abuse Services (OMHSAS). In addition to employment services, he led certified peer, suicide prevention, COVID-19 emergency funding, Fairweather Lodge, supported education and Veterans program development. He lives in Camp Hill with his wife and has two sons. His favorite sport teams are the Steelers and Penguins. He also is very active in local ministries serving those with criminal records and mental illness.
Contact Information
Randall E. Loss
Pennsylvania Office of Mental Health and Substance Abuse Services
Human Service Analyst
rloss@pa.govPrice | 60-69
Volume 11 ► Issue 3 ► November 2022
The Contribution of Psychological Safety to Employees Mental Health
Kate Price, D. Clin. Psych, Organizational Culture Consultant, Author
Introduction
The issue of mental health in the workforce is increasingly coming to the fore in the wake of the pandemic. We are seeing huge numbers of employees changing jobs, suffering from stress, anxiety, burnout and even leaving the workforce entirely.
In 2019, the World Health Organization updated its definition of burnout as a syndrome resulting from unsuccessfully managed workplace stress.1 The American Institute of Stress tells us that within the US, 83 percent of workers suffer from work-related stress, 53 percent are disengaged, and one million miss work each day due to stress.2 This has a huge cost to organizations, with depression-induced absence alone, costing US businesses $51 billion a year and billions more in healthcare costs.
With chronic stress being a predisposing factor for mental ill health, as well as substance abuse and other diseases, this is clearly a major cause for concern.
Perhaps the biggest question this raises is, where does the responsibility for mental health lie? Is it an individual issue or a systemic one? What role does our environment play? And what responsibility do employers have to support the well-being of their employees?
Organizations and society as a whole tend to view mental health as an individual issue, suggesting those who are not in perfect mental health are somehow deficient or weak. As a clinical psychologist, I would instead suggest that it is the environments in which we expect people to live and work that bear at least some of the responsibility.
To exemplify this idea, I would like to introduce you to Jeff, a client of mine that had two very different experiences in the workplace.
A Tale of Two Workplaces
As an employee of a large hierarchical organization, Jeff felt that he was unable to express his views or tell anyone when he noticed problems in work processes. The culture was one of blame from the top down and layoffs were becoming the norm. He described feeling unable to be himself at work. He felt he was always having to present the right image to avoid being judged, criticized, or potentially even being demoted or losing his job. Over time he shut down and became more and more withdrawn. He interacted less with his colleagues and felt that he was unable to ask for help with either work tasks or personal needs.
Without any support in the environment where he spent a large part of his waking hours, he began to fear going to work where he felt alone and at times despairing. His sleep was affected leading to, not just a reduced capacity to manage his workload, but also a reduced ability to manage his emotions, which at times felt overwhelming. As he withdrew, his boss assumed Jeff was disengaged and his criticism increased. His boss’s comments in front of Jeff’s colleagues and team provoked feelings of shame and doubt in his own abilities. As his stress levels mounted and he attempted to deal with his toxic work environment, his feelings of anxiety and depression increased. Jeff’s risk of a serious mental health crisis increased significantly.
When I first met Jeff, he had reached out for help after finding none was available within his organization. As we discussed what was happening, he came to the realization that his workplace was toxic. He was struggling to make changes within a system that did not care about his needs but was instead focused solely on business output and efficiencies. In the midst of his emotional and mental struggles, Jeff had put the blame firmly on himself and had not recognized the impact his environment was having on him. Within a couple of months, he was able to find a new job. His new organization supported and invested in his coaching relationship with me. Initially, Jeff was fearful of offending his new boss and held back in case he said something wrong. He made an effort to fit in with his new colleagues but did not want to stand out and so did not share his creative ideas or challenge the status quo. In the past, his confidence enabled him to challenge existing beliefs and team norms and he reflected that people had appreciated his original thoughts.
So why was he holding himself back? The fears and self-doubt that are created in a toxic environment, and the associated stress and anxiety do not magically disappear when we find ourselves in a new and more positive situation. The effects of feeling shame, unvalued, or at risk of rejection linger. We must learn to trust that our new environment is different. As Jeff was encouraged by his new colleagues, treated with empathy, and accepted by the group, he began to share his thoughts and ideas. He gained confidence in reporting mistakes knowing this would lead to solutions, could ask questions, and expect to receive thoughtful answers. He came to trust and respect his colleagues and know they felt the same about him. When his mother died, he didn’t hesitate to tell his coworkers and boss and received both the practical and emotional support he needed in that moment.
In this workplace, unlike his previous one, Jeff felt psychologically safe.
What is Psychological Safety?
Psychological safety is a term used by William Kahn in 1990 as “being able to show and employ oneself without fear of negative consequences to self-image, status or career."3 It has since been researched in depth by Amy Edmondson, a Harvard professor, who describes it in her book The Fearless Organization as "a climate where people feel safe enough to take interpersonal risks by speaking up, and sharing concerns, questions, or ideas." 4
If we consider Jeff’s first experience, it is easy to see his fear of negative consequences if he spoke up and how this discouraged him from taking risks. In his second, psychologically safe workplace, we see how despite the negative impact of his former environment, Jeff rebounded and felt confident to be himself at work, knowing that his voice and diverse perspectives would be valued and that he was accepted by his colleagues. If we can create environments where people can be themselves, feel accepted, and be able to speak up then we reduce emotions that lead to both stress and other serious mental health issues.
Is Mental Health an Individual or a Systemic Issue?
I believe it is both and therefore must be addressed at both levels, as well as changing perceptions of mental illness at a societal level. As we saw with Jeff, the same person in two different environments can either thrive or struggle to survive. His situation was not just about individual resilience, it was about the impact the environment around him had on his ability to function, the way he felt about himself, and how he built relationships with others. These factors are core to our well-being and if we could design psychologically safe workplaces then we would be taking positive steps to preserve our employees’ health and well-being, as well as reducing the pressure on the mental healthcare system. From a business perspective, we would be facilitating productivity, collaboration, and business success which are typically the ultimate goals of most organizations.
If we think specifically about the pandemic, we can see the impact that the environment and our external circumstances have on our mental well-being. A high percentage of people struggled as we were forced to remain isolated, cooped up in our homes with huge uncertainty and fear about what was happening in the world, not knowing the risks to ourselves or our loved ones. As the pandemic continued, we saw increasing rates of mental health problems as a result of anxiety, loneliness, and isolation, as we were denied our usual outlets for self-care and relieving stress.
This is certainly not to say that the workplace, stress, or our environment are the only factors at play in mental health issues. Mental health is complex, with many and varied disorders, which have a multitude of underlying causes and factors in play. What I think is true to say is that our environment and negative experiences can contribute to, or exacerbate, the development of mental ill health.
A decline in an individual’s mental health affects many things including: their experience of and enjoyment of life; relationships with families and work colleagues as their ability to handle stress and emotions alters; work performance may suffer; and the levels of compassion for clients, patients and others whom we come into contact with - a condition often known in healthcare as compassion fatigue- is reduced. Beyond that it affects the outcomes for business, it can lead to high turnover, disengagement, reduced productivity, absenteeism, and spiraling healthcare costs, to name just a few.
Moving Forward
Supporting the mental health and well-being of employees does not detract from the goals of a business but instead enhances its success. If organizations understood this, they would be more likely to invest in these areas and intentionally create psychologically safe cultures to the benefit of all. Placing people as a priority supports both individual employees and the achievement of business goals because people are the lifeblood of your organization.
Recommendations for Organizations and Leaders
Some ideas for organizations and leaders to create a psychologically safe environment include:
- Encourage productive conflict and the sharing of new ideas and ensure that they are well received.
- Remove the blame from the situation and instead treat failures and mistakes as learning opportunities.
- Encourage vulnerability; get to know the people you work with and have empathy and understanding for their struggles and experiences.
- Be aware of your responses to others; ask yourself are you causing them to shut down or feel excluded? We must all consider if at times we might be the toxic coworker. Everyone on occasion says or does things that make others feel bad. The key is to increase our self-awareness and recognize when we might be the negative influence in the environment. By becoming aware and acknowledging our impact, we can then take steps to change it.
- Be conscious of your employees’ workloads or if standard processes or procedures are adding unnecessary stress to people’s workdays.
- As a leader you must model the behaviors and culture you wish to see. What you do sets the tone for your organization.
Conclusion
My own experiences working in mental health services as a clinical psychologist led me to believe that as clinicians, we are tackling these issues too late. We only offer support to people once they are in crisis and often it is difficult to turn issues around at this stage. This is an ever-increasing issue as mental health services are simply overwhelmed. Staffing shortages, a lack of qualified professionals and reduced budgets, alongside a continually growing need for these services, has resulted in access being denied to all but those in the most severe need. This is clearly unsustainable and leads to the exacerbation of mental ill heath in populations which might be more simply addressed if professionals were readily available to meet those needs. The huge stress placed on the healthcare system often subjects healthcare professionals to psychologically unsafe working conditions, placing them at the same risk of stress and burnout that they are working to treat in others.
Psychological safety alone will not prevent difficulties with mental health, nor will it solve all problems in a workplace. However, it is one factor that can be addressed and is known to have a positive effect on workplace experiences, stress, and the development of mental health issues. By addressing some of the root causes of these difficulties we can take a proactive and preventative approach to health and wellbeing. This can change the experiences of individuals and transform the systems they function within.
References
1. World Health Organization. ICD-11: International Classification of Diseases 11th revision; 2019. https://icd.who.int/ . Accessed October 14, 2022.
2. The American Institute of Stress website. https:/./www.stress.org/workplace-stress#:~:text=83%25%20of%20US%20workers%20suffer,stress%20affects%20their%20personal%20relationships. Accessed October 14, 2022.
3. Kahn, W. A. "Psychological Conditions of Personal Engagement and Disengagement at Work". Academy of Management Journal. 33 (4). 1990; 692–724. doi:10.2307/256287. ISSN 0001-4273. JSTOR 256287.
4. Edmondson, A. C. The Fearless Organization: Creating Psychological Safety in the Workplace for Learning, Innovation, and Growth. John Wiley & Sons; 2018.
Biography
Dr. Kate Price is an Organizational Culture Consultant. She has a Doctorate in Clinical Psychology and worked for over two decades in the UK's National Health Service. Kate is the author of "Taming the Culture Tiger: the art and science of transforming organizations and accelerating innovation" (Coming December 2022), Owner of DKP consulting she focuses on leadership and cultural change in healthcare and life science organizations.
Contact Information
Dr. Kate Price
Organizational Culture Consultant
DKP Consulting
kate@drkateprice.com